“Boosted Americans 97 times less likely to die of virus than unvaccinated” (USA Today, 2/2/2022):
As the U.S. inches up to a 64% vaccination rate for the entire population, only 42% of those eligible for a booster have gotten the extra shot, and experts aren’t sure what will move the needle, so to speak.
Fully vaccinated Americans are 14 times less likely to die of COVID-19 than those who haven’t gotten the shots. Boosted Americans are 97 times less likely.
Those were the figures presented Wednesday by Dr. Rochelle Walensky, director of the Centers for Disease Control and Prevention, based on reports from 25 jurisdictions in the week ending Dec. 4. For every 100,000 people, 9.7 of those who were unvaccinated were killed by the coronavirus, compared to 0.7 of those fully vaccinated and 0.1 of the boosted.
Science (the CDC) tells us that the COVID-19 vaccination, in a full three-dose series, is the most effective pharmaceutical intervention ever developed. Although of course we believe Science and trust in the CDC, some questions are raised by this astonishing 97X risk reduction. At least over in Sweden, pre-vaccine SARS-CoV-2 wasn’t dangerous enough to justify terminating citizens’ right to gather, children’s right to attend school, etc. Nor was it dangerous enough to justify ordering people wear masks. We’re told that we a 97X reduction in risk is available and yet American schoolchildren, down to age 2, are ordered to wear masks and subject to various other restrictions. Vaccine papers are checked at restaurants (e.g., for those 5+ in Boston) to make sure that the unclean don’t mingle with the sacred. A range of restrictions are applied to discourage travel. But if the sacred have cut their risk by 97X, why are they worried about the 5% filthy untouchables (unvaccinated)? Is our tolerance for risk 97X lower than what prevails among Swedes? That is contradicted by the fact that Americans refuse to accept my proposed 35 mph speed limit, which would save more life-years than curing COVID-19.
We don’t order all road travel to cease because some people insist on riding statistically dangerous motorcycles. Why do we have COVID-19 orders in place when a 97X reduction in risk is as close as the nearest CVS? The people making the orders are Democrats and we are constantly informed that it is only Republicans who refuse to accept all three Sacraments of Fauci. Why do Democrats care if SARS-CoV-2 winnows out some of the Deplorables who could potentially vote a fossilized Donald Trump into a renewed dictatorship?
Another possibility is that the 97X risk reduction, while proven by Science, isn’t real. Here’s some data from Israel, famous for early adoption of vaccines and boosters:
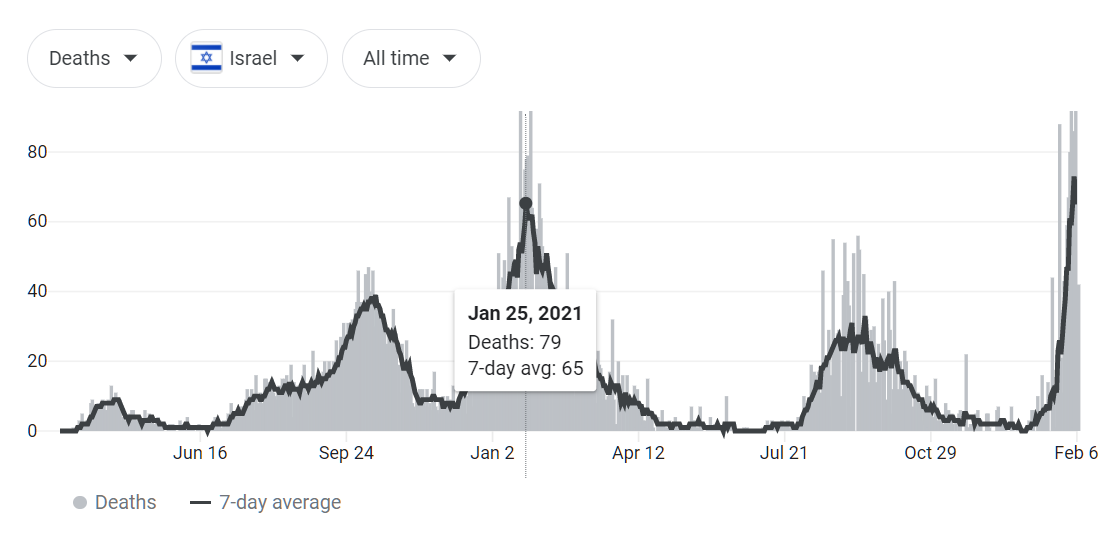
Deaths tagged to COVID-19 are at an all-time high. This, despite the fact that those who aren’t boosted are excluded from public life. “Israel’s bet on early COVID booster shots pays off” (DW, 11/11/2021):
To enter the club, people must present their green pass, which includes an ID number and a QR code. “When somebody wants to go either to the pool or the gym, we check the green pass. Everybody has it on the phone these days. Sometimes it’s a little bit of an inconvenience, but people understand and cooperate,” said Levi.
In October, Israeli authorities canceled the green passes of those eligible for the third shot but who hadn’t received it yet. Those who don’t have a green pass can get a 24-hour pass by taking an antigen or “fast” test to enter facilities.
I’m wondering if the spectacular cited effectiveness of booster shots among Americans is partly due to the demographics of those who choose to get boosters. In Why rich white Americans believe in masks (October 22, 2020), an MIT professor:
It’s the usual causality problem with epidemiology. Upper middle class Northeasterners (like me) are adamant about mask wearing, and they rarely get sick. So it must be working.
(He added that a mistaken belief in mask efficacy would still be a positive because it would help assure a Biden/Harris victory. He bought his house, his cars, and his common stocks pre-2020, so the first year of the Biden Administration has been fine for him, financially.)
What would the “usual causality problem with epidemiology” look like in the booster world? What if the people who have the time, patience, and inclination to get boosters are rich white people who have the luxury of staying in their suburban bunkers 98 percent of the time? They weren’t likely to get COVID-19 in the first place and they’re not getting COVID-19 during their twice/week N95-masked excursions to the supermarket.
Note that this is not to suggest that the booster shot has no effect (see Maybe it is time for that booster shot? for why you might want to get one even if you think it has no effect!). But a post-boost 1/97th risk level seems tough to achieve by pharmaceutical means alone and without some help from Dr. Differential Demographics.
Related:
- “Unvaccinated vs. Boostered: What the COVID Death Toll From Israel Reveals” (Haaretz, 2/6/2022; remember in reading this that “partially vaccinated” in Israel means just the first two shots while “fully vaccinated” is three): “According to ministry figures, on January 31 the death rate per 100,000 people for the over 60s stood at 16.3 for unvaccinated individuals, as opposed to 0.9 for the fully vaccinated.” (1/18th the risk for boosted versus unvaccinated, not 1/97th!) Buried near the end, the demographic angle: “there is also a clear variation in death rates between groups with lower and higher socioeconomic status.”
- Why doesn’t the raging plague in Maskachusetts cause doubt among the true believers in Faucism? (1/3/2022; the Google shows that deaths in MA right now are at roughly the same level as the January 2021 “second wave” peak)
> What would the “usual causality problem with epidemiology” look like in the booster world? What if the people who have the time, patience, and inclination to get boosters are rich white people who have the luxury of staying in their suburban bunkers 98 percent of the time? They weren’t likely to get COVID-19 in the first place and they’re not getting COVID-19 during their twice/week N95-masked excursions to the supermarket.
Yours Truly, a Data Point: I was Pfizered in March/April of 2021 and boosted with Moderna later that year. I wear an N95 mask whenever I am in an indoor setting other than my home or car. I live in a semi-rural area and because of my illness and treatment (which tipped the scales for my vaccination in the first place) I have become very adept at keeping my distance from people. I have eaten at zero sit-down restaurants. I’ve visited the grocery store exactly twice, late at night when it was closing and almost empty. When I enter convenience stores I try to wait until the parking lot clears out and then another few minutes for their ventilation systems. I do my absolute best, in other words, to keep myself as far as possible from people with the virus.
I have spent a considerable number of days in a hospital or other healthcare setting over the past 18 months. I always try to schedule my appointments early in the mornings and my condition itself does not usually entail very many comorbid patients waiting with me. I try to hit the appointment times “on the nose” so that I don’t wait long.
My life has been rearranged by my medical treatment such that I do not find myself in close contact with even my older parents very often. It’s been a little lonely, for sure, but I have tested PCR negative for COVID-19 six times now. I do not think I have ever been close enough to someone long enough to be infected. Therefore I have no idea whether the booster shot helped me or was completely irrelevant.
I will note, however, that the last time I went to the hospital, I parked in their outdoor garage on an upper floor, which meant that took the unheated elevator to the lobby level. Once the elevator doors closed, I could the vapor contrails of my aerosolized breath spread through the air around me every time I breathed. This was wearing a “properly fitted N95.” I am aware of risk-compensation phenomenon (in part thanks to this blog) and it was vivid example of why masks are *utterly useless* in a setting where people are gathering close together because they “feel protected” – particularly if they remove those masks to drink, eat., etc.
Fingers Crossed! I still believe Judith Persichilli from March of 2020: “I’m definitely going to get it. We all are.” https://www.nj.com/coronavirus/2020/03/im-going-to-get-it-we-all-are-njs-top-health-official-says-as-she-leads-the-states-coronavirus-war.html
I have done everything above so that when I do, I will be as healthy as I possibly can be in every other respect.
Addendum: One thing that I cannot estimate accurately. Since the immune system is adaptive and under normal circumstances requires exposure to pathogens/antigens to optimize its responses, I wonder if my meticulous self-quasi-isolation has not, in fact *weakened* my system’s “fitness” and I will be more susceptible to illness for a period of time after I emerge from my “bubble?” I wasn’t a particularly “sickly” child or adult, and I’ve never been a germophobe (as some of the places I’ve slept in my life attest.) So I might have to be more careful than usual about becoming sick in the more mundane, ordinary way. Time will tell!
There is such a thing as: “Too Clean!”
https://www.frontiersin.org/articles/10.3389/fimmu.2017.00292/full
@Alex – thanks for sharing what you have going through, dealing with, and doing. Wow. Thanks for your continued postings, info, wit, and humor, and here is to your health being ok!
@Paul B: Thank you very much. Like most people, I never really expected to have to cross these rivers, but I’m doing the best I can and I’m trying to convey the experience accurately here when I think it is appropriate. I truly thank our host for putting up with that – he certainly doesn’t have to – but I am trying to be at least truthful even when I cannot be completely accurate. I’ve learned a lot about myself and the nature of my existence and marvel at it and appreciate it more. It’s a very humbling experience.
The 97x figure sounds ridiculous. Perhaps the Unvaccinated should move to Israel, where the vaccine does not make any difference:
https://www.israelnationalnews.com/news/321674
“Are Israeli hospitals really overloaded with unvaccinated COVID patients? According to Prof. Yaakov Jerris, director of Ichilov Hospital’s coronavirus ward, the situation is completely opposite.”
“‘Right now, most of our severe cases are vaccinated,’ Jerris told Channel 13 News. ‘They had at least three injections. Between seventy and eighty percent of the serious cases are vaccinated. So, the vaccine has no significance regarding severe illness, which is why just twenty to twenty-five percent of our patients are unvaccinated.'”
(I’m aware of the fact that if 99% of Israelis were vaccinated, most of the hospitalized patients would naturally be vaccinated. But only 66% are fully vaccinated and 55% fully boostered.)
The state of California provides a sizable population of inhabitants and some data on mortality of unvax/vax/boosted here that you may find interesting:
https://covid19.ca.gov/state-dashboard/
Scroll to: unvaccinatied & vaccinated data -> Deaths
30x, not 97x. Which is right?
The reality is, people up to 14 days after vaccine (the second dose, if applicable) are considered “unnvaccinated” according to CDC reporting guidelines. So most of vaccine adverse reactions get reported as COVID (signs of spike protein toxicity are the same, as the protein is the same) and deaths due to vaccination are counted as “unvaccinated” deaths.
A basic scientific literacy must include firm understanding that numbers mean absolutely nothing if you don’t understand how these numbers are collected and what they actually represent.
This very lengthy paper shows the intricacies involved in collecting and interpreting the data:
https://www.researchgate.net/publication/357778435_Official_mortality_data_for_England_suggest_systematic_miscategorisation_of_vaccine_status_and_uncertain_effectiveness_of_Covid-19_vaccination
Page 10 supports averros’ hypothesis:
“In all three figures we see peaks in mortality risk for the unvaccinated across each age groups that occur almost immediately after they had received the first vaccine and peak at consecutively later times in line with when vaccine was administered for that age group. The fact that the peaks in mortality are not temporally aligned strongly suggests that this is not caused by natural events. Nor can it be argued that it is caused by undiagnosed covid infection [32] given that the peaks in non-Covid mortality occur later than the much earlier peak in covid infection, especially for the younger age groups. As reported previously [16], such a phenomenon would be inevitable if the deaths of people who die shortly after vaccination are miscategorised as unvaccinated.”
I think the people who collect the data do not have time for fine grained data collection. The people who write medical papers do not have statistical knowledge or patience for detailed analyses. Every medical study should be reviewed and fact-checked by a statistician.
I got my first 2 shots but I am not getting a booster. I am done.
As Obama used to say:If you like your 2 shots you can keep yours 2 shots.
And you still don’t care about Black Lives Matter!
randall g: Nobody should care about Black Lives Matter. It was and is a ChiCom sponsored front group. Former Trained Marxist Patrisse Cullors is very well aware of that, but Xi got a lot of laughs while Chinese printers and manufacturers profited off the sales of BLM signs, T-shirts and other paraphernalia while the Useful Idiots marched and burned and tore down American monuments while Mayor of Washington DC painted city streets proclaiming their message. Patrisse is now a Millionaire many times over and she’s been featured recently in the Hollywood Reporter talking about her new life changes.
@randall g: Now she’s featured in the Lifestyle section of The Hollywood Reporter with her new chunk of cash and an art gallery! She’s also got a deal with Warner Brothers, so she’s gone from Trained Marxist Revolutionary to Bourgeois Influencer almost overnight. A few million dollars will do that for anyone!
https://www.hollywoodreporter.com/lifestyle/arts/patrisse-cullors-interview-book-black-lives-matter-1235079401/
@randall g: In fact, BLM was a such a success that we now have a whole new group of academics teaching students how great they are with taxpayer dollars and who can’t be fired! I have to hand it to Xi Jinping: he knows how to spend his money turning American streets into riot zones with monuments to his understanding of American culture, such as it exists now. They’re way inside, and it goes higher than you might think.
I wear mask and never got sick during last 2 year while working from home
There is extremely good Israeli data for the delta variant: (https://www.nejm.org/doi/full/10.1056/NEJMoa2115624). This compares death rates between fully vaccinated and boosted for Delta. So I am puzzled why do you think the American numbers which are consistent with the Israeli numbers are so far off.
Death rate boosted 65/758,118=.0000857
Death rate non boosted 137/(843,028 – 758,118) =137/84910 = .001613…. or about a 19X reduction in the death rate of boosted vs fully vaccinated for delta. While one can argue that unvaccinated people engage in riskier behavior than fully vaccinated people, a further 5X or so reduction seems completely justified. (In fact, the reduction is s >10x but that includes all groups of all ages.)
The CDC says Delta doesn’t exist any longer (<0.1%) which is why they rescinded the EUA for mAbs.
https://covid.cdc.gov/covid-data-tracker/#variant-proportions
We shouldn't be using efficacy data for a variant that is no longer circulating.
Of course Illinois reported that Delta was 15.42% of infections the same week that the CDC said Delta was <0.1% nationally.
https://dph.illinois.gov/covid19/data/variants
The vaccines are highly effective for a grand total of four months after boosting, against a variant that is no longer circulating. C’mon now, everyone get boosted! — CDC
Gary: Thanks for the NEJM paper. I don’t think it is inconsistent with the original post. The authors say “Participants who received a booster at least 5 months after a second dose of BNT162b2 had 90% lower mortality due to Covid-19 than participants who did not receive a booster.” But the study period was August 6-Sept 29, 2021, which is prior to the government coercion described above (expelling the unclean from public life by revoking their green passes). So it was a self-selected group that got boosted.
Pre-Covid we wouldn’t have accepted studies like this, but would have demanded a randomized controlled trial. Or at least one that controlled for patient demographics (though I think Karenhood and bunker-fondness is tough to measure).
Imagine a study of children exposed to second-hand tobacco smoke versus children not exposed at home in the U.S. We would find that the kids exposed to the smoke had all kinds of bad health problems. But if we don’t control for the fact that kids exposed to smoke are in lower-income households, the study wouldn’t be worth anything.
https://www.thelancet.com/journals/lanam/article/PIIS2667-193X(21)00111-3/fulltext
says “we find that [Mexicans] in the lowest income decile still had a probability of dying from COVID-19 five times greater than those at the top decile.”
https://www.ama-assn.org/delivering-care/health-equity/data-10-cities-show-covid-19-impact-based-poverty-race
“In [U.S.] counties where the population was substantially non-white with a median income defined as $60,240, the COVID-19 death rate was more than nine times higher when compared to counties that are substantially white with the same median income.”
Regardless of booster sacrament, COVID-19 has a tougher time reaching the Progressive righteous in their $9.6 million suburban houses than it does reaching the Latinx essential workers in their urban apartments. (see https://philip.greenspun.com/blog/2021/01/02/the-social-justice-of-coronashutdowns/ )
If you read the nejm paper they did try to look at subgroups like haradim but that is irrelevant because the numbers are so large, the sample of Israelis so diverse, and the data so clear, a randomized trial is irrelevant. When the sample sizes are large, the confidence intervals are good, a randomized trial is overkill. At least for Delta the evidence of a risk reduction on the order of >=19x is overwhelming. Do you know any any biostatician who is saying otherwise about the Israeli data? Ioneedes certainly hasn’t said anything about the Israeli data to the best of my knowledge for example
Now I grant you omicron is a whole different kettle of fish because the case fatality rate is so low…
Gary: I’m frankly not sure what to make of these Israeli data. I don’t think Israelis are as incompetent as we are with medical record systems so I believe that they can at least accurately tag people as vaccinated or not. And, unlike some of the commenters here, I do think that the vaccines can have some protective value to individuals (we may yet find that universal vaccination was a mistake, however, due to the pressure that universal vaccination applies for the virus to mutate). But the 97X risk reduction seems too good to be true without a lot of help from mistakes in gathering and processing the statistics. What else in pharma works that well? (And if the vaccines are working that well, why the massive plagues in places that are heavily vaccinated and boosted, such as Maskachusetts and Israel?)
It is possible for a great vaccine to have that kind of reduction or even better. Measles and in the old days smallpox, vaccines have even better death rate reductions for example. What is amazing is that the mRNA vaccines are giving you measles and smallpox level reductions. My virologists friends all thought that we would be lucky to get flu vaccine like reductions when this was first happening, thankfully they were wrong.
And remember we are talking about death rate reductions, not infection reduction. Completely different kettle of fish
Gary: Do you have a source for the measles death rate reduction? A “97X reduction” implies that the measles vaccine should be 99% effective in preventing death in an environment where measles is spreading, right? But where can that have been measured? Once measles vaccines were introduced in a country, the infections stopped. We would need a significant number of people who were vaccinated against measles and who then visited a place with a measles outbreak.
https://www.science.org/content/article/measles-outbreak-traced-fully-vaccinated-patient-first-time (2014)
is an anecdote that I found. Some people who were vaccinated against measles got infected by measles and did not die. But, on the other hand, most unvaccinated people who get measles also do not die.
look at historical measles death rates starting in the late 50’s, early 60’s to the death rates from measles in the mid to late 60’s. There were roughly 500 deaths per year in the earlier period and essentially none in the later period. I didn’t bother running any fancy statistical tests for significance cause 500->0 doesn’t need them, no?
But I want to stress death rate reductions are very different then infection reductions. While I’m not a virologist or an MD, there is no reason why one couldn’t have essentially no deaths after a vaccine but no significant reductions in infection rates. If you think about it right, that is what happens with rabies,no? You won’t die but boy will you be sick
The 97x figure comes straight out of Pfizer marketing materials. Based on “studies” which remain top secret. Yeah, the same kind where they vaccinated their control group and which will not be published for another 50 years or so.
Since many people believe this number, I guess I’ll start investing into bridge sales.
So would you think this professor, who is working in a corona ward, is lying or is being misreported (this is Omicron though):
https://www.israelnationalnews.com/news/321674
I’m not an anti-vaccine hawk, but I don’t believe the 97x numbers for Omicron. I also think that in the U.S. and continental Europe medical professionals are heavily censored. All free news comes from Israel or Britain.
Like most MDS he knows almost nothing about statistics, it’s frightening how bad most drs are when thinking about statistics. The following paper has it’s results replicated every few years:
https://www.nejm.org/doi/full/10.1056/nejm197811022991808
This md’s statement is a classic case of the base rate fallacy and would be laughable if it wasn’t so scary
https://slate.com/technology/2021/08/what-it-means-when-75-percent-of-covid-19-cases-occur-in-vaccinated-people.html
Phil,
1. My understanding is that the vaccines are better at stopping replication in lungs and organs, but worse at stopping replication in bronchus or sinus. That explains the high fatality protection and low spread protection. It is also why some people want to research nasal versions of a vaccine.
2. Interestingly, Omicron has the same dynamic as the vaccinated Delta; Omicron reproduces much faster in the bronchus and sinus, but slower in the lungs due to different membrane proteins. This explains the tremendous spread and low fatality of Omicron, for basically the same reasons the vaccine helps against Delta.
3. There’s a tremendous sleight of hand in using Delta efficacy studies and Omicron case rates to justify tyrannical mandates. It’s like two different diseases and the severity reduction from the vaccine and Omicron is driven by a similar mechanism. The vaccine is nearly useless against Omicron, which the CDC claims is now 99.9% of cases.
4. In the famous words of Dr Emmitt Brown, “Marty, you’re not thinking fourth dimensionally!” There are serious risks to repeatedly vaccinating people with a vaccine that only offers strong protection for four months, and only against defunct variants. That is true for people who may experience side effects, or antigenic memory toward old variants (implying weakened immunity to new variants), or cumulative allergies from the vaccine. And as you already mentioned, there are evolutionary risks to using the same narrow spectrum vaccine on an entire society.
Gary: If you “look at historical measles death rates” aren’t you looking at combined effects from infection reduction and death reduction? There is no way to tease out from those measles death rates, in which the infections themselves were extinguished, what the protection from death in a measles-plagued environment would have been, is there?
I guess there is something of a precedent for a vaccine that is highly effective against death but doesn’t do much (other than spawn mutations) for infections. https://en.wikipedia.org/wiki/Marek's_disease has a vaccine that perhaps does reduce death rates dramatically, but doesn’t interfere with infection.
The 97X claim is inconsistent with what the British are saying. They’re saying “95 percent”. See https://www.gov.uk/government/news/boosters-provide-high-level-of-protection-against-death-with-omicron
95 percent is more like 20X, not 97X.
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1052353/Vaccine_surveillance_report_-_week_5.pdf
is the basis for the British statement. Confusingly, it shows a “hazard ratio versus mortality” of 0.12 after dose #3. I’m not sure how they get 95% from that (some background at https://healthjournalism.org/blog/2020/10/know-the-nuances-of-vaccine-efficacy-when-covering-covid-19-vaccine-trials/ ).
(If the hazard ratio they’re publishing is risk-for-triple-vaccinated divided by risk-for-unvaccinated then you’re about 1/8th as likely to die if you’ve had three shots compared to if you’ve had none. That seems more consistent with the raging plagues and continued deaths in countries where three shots are common.)
Trust Israeli data more than UK data.
Death rate reduction means death rate reduction it has no thing to with infection reduction and for many vaccines, infection reduction is not particularly correlated with how well it reduces the infection rate
While, it would possible to do a paired retrospective study on death rates for vaccinated people from measles in the period after the introduction of the vaccine vs the period before, no biostatiscian I know would think it necessary. When you go from 500 deaths from measles to basically 0 in a population as large as the us in 1963,4,5 etc, you know the reduction of risk from deaths is astonishing. This reduction in the risk of death has nothing to with the reduction in infection rate. Yes the absolute numbers are small and so the %of people who die after a measles infection even smaller but that isn’t what you are calculating. You are talking about comparing ratios of deaths in two groups.
Gary,
You are being unfair to the Israeli Prof. I think he does understand the math. Before you start laughing or getting scared at/of hist statement, please check your own reference and the high school math referenced in the article. As someone pointed out, if at 80% of the total Israeli population were vaccinated, then vaccination would not matter judging by the Prof’s data.
Now, if his demographics consisted solely out of 90% vaccinated people you might have had a point, but you don’t know that without making assumptions. According to the Lancet only 67% of the Israeli population is vaccinated.
re: ” What if the people who have the time, patience, and inclination to get boosters are rich white people who have the luxury of staying in their suburban bunkers 98 percent of the time?”
Yup, I suspect selection bias and correlation explains part of the difference results seen between the boosted, those with only the initial vaccination, and the unvaccinated. I hadn’t checked to confirm, but I’m guessing they didn’t control for various factors like obesity, or behavioral differences between the groups.
Those who fear covid may be more likely to get a booster, to hide away from getting covid, and perhaps to be more paranoid about health risks in general and therefore less likely to have controllable risk factors for serious illness&death like obesity.
Apparently, the web site being cited for that “Israeli Prof” is BS. The true story may be found here it seems.
https://www.techarp.com/science/yaakov-jerris-vaccine-severe-covid/
So, first off, he isn’t a professor but an internal medicine doctor and the main issue is his original statement doesn’t seem to have been anywhere like the one quoted. (And I’d bet he really doesn’t understand the math, it’s an unusual dr that does – even at Harvard Medical School apparently – as the article I cited shows.)
But let me be clear, the statistics for Omicron are completely different than for Delta. Vaccines are somewhat helpful for Omicron but by no means as important as they were for Delta where they really did an amazing job of protecting people. You could even make an argument that vaccines for Omicron are overdone for non-vurnable populations (well if we knew the risk of long covid from Omicron which we don’t…)
As best I can tell from what I read, Omicron is not as bad as the flu but people do get pretty sick from the flu even though it is unusual.
Gary, I read the same report in Israeli press, the professor/ doctor is the head of COVID ward in a major Israeli hospital. The rest is exactly as reported here.
If you look closely at what he apparently said, it was that the people are being admitted “with covid” not “for covid”. In that case, given that people admitted to a hospital are more like to have co-morbidities and so be fully vaccinated (in Israel people with comorbidities are >=85% boosted), this is so obviously a case of the base rate fallacy, you could use it in teaching the concept
He said “with covid” for all covid cases, not just recent. He is a professor and he was addressing Israeli cabinet (executive branch of government consisting of ministers) Sunday one week ago. Here is the best translation of Prof. Yaakov Jerris: ““Defining a serious patient is problematic. For example, a patient with a chronic lung disease always had a low level of oxygen, but now he has a positive coronavirus test result which technically makes him a ‘serious coronavirus patient,’ but that’s not accurate. The patient is only in a difficult condition because he has a serious underlying illness.””
Not sure why you are trying to discredit the poor Prof. Firstly, he is, in fact, a Prof.:
https://il.linkedin.com/in/jacob-giris-46309185
Secondly, his name is roughly rendered as Yaakov, in Hebrew: יעקב
Thirdly, I’d bet he knows more math you ever will.
Oh, while not getting into the details, the chances of him knowing more math than I do would be rather slim – probably impossible. I have met a couple of people who know more biostatistics than I do who have MD’s but that isn’t what I trained in or did research in.
(I have met MD’s who left mathematics to become MD’s to be sure – but they left mathematics early on – usually before they got tenure. I don’t know any who kept on doing mathematics …)
GC, I doubt that good professor needs to derive probability of series at infinitum on a topological space. I hope that you teach at Cornell because applicant and student hard math level there is laughable.
If I’ve learned anything from this topic, it’s that contrarians are never wrong–that’s everyone else’s job.
Philg – how about a review of the vette? I’d love to hear your thoughts on it. Seems like some remarkable engineering in terms of price vs performance.
SP: Certainly Science has never been wrong with respect to coronaplague and therefore should not be questioned, even when a 97X reduction in death is promised. The general public should not buy or wear masks, for example. Then, the general public should not buy or wear N95 masks. COVID-19 is spread by respiratory droplets, not aerosols. Unmasked, unshut Sweden would have a higher death rate than U.S. states and European countries that donned masks and locked down. Etc., etc.
Philg – Why wear masks now that there’s a vaccine? Because contrarians who second guess the experts have convinced the general public that behavior which has been universally accepted, mandated, and ubiquitous for decades–getting vaccines–is now risky, with zero credible evidence to support the claims. As a result, we have a very low vaccination rate. Not to mention some fraction of the population which cannot be vaccinated. And, masks work, with zero downside. They reduce viral load if nothing else, so even if you’re vaccinated, there is a benefit. If the Canadians woman’s hockey team can wear them during the match and win Olympic gold, surely fragile, contrarian Americans can too.
Again with Sweden, which has significantly higher death rates than it’s neighbors. Also, they did take precautions including some form of restrictions on gatherings and wearing masks. Perhaps they faired better because they don’t have a large contrarian movement and people acted responsibly of their own accord.
By this logic, sheep should have upper hand in the wild. No contrarians there, unity would defy them wolves. Like it does viruses.
Senorpablo: South Africa, which is being denied vaccines by white supremacists and has fewer regulations than the U.S., has a far lower cumulative death rate than the U.S. Also it produced the weaker Omicron variant.
Earlier pandemics like the 1918 flu were shorter without the precious vaccines.