Since all that hospitals are generally doing for COVID-19 patients is providing supportive care (i.e., not treatment) and, in fact, patients can do just as well at home with an oxygen bottle (nytimes), it seemed like an obvious idea to look for a way to handle COVID-19 patients somewhere other than a hospital. If nothing else, this would prevent the COVID-19 patients from infecting workers and patients within the hospital. If we could build renal dialysis capacity, why not COVID-19 treatment centers? is my idea from April 2, 2020:
On the one hand, the U.S. health care system is kind of lame. It consumes a ton of money. New York State spends $88 billion per year on its Department of Health, $4,400/year for every resident, mostly just for people on welfare in New York; Mexico spends about $1,100/year across all citizens, including those with jobs. The U.S. health care system delivers feeble results. Life expectancy in Mexico is 77 versus 78 in the U.S. Despite this prodigious spending, New York has completely failed to protect its residents from something that isn’t truly new.
On the other hand, the U.S. managed to build enough renal dialysis capacity to keep 468,000 Americans with failed kidneys alive. This is a complex procedure that requires expensive machines, and one that did not exist on a commercial basis until the 1960s.
…
Of course, one issue is that we had decades to build up all of this renal dialysis capability while we have only about one more month to build COVID-19 treatment capacity. But once we have built it, can we sail through the inevitable next wave or two of COVID-19?
(Looks like I can take credit for predicting “the inevitable next wave or two of COVID-19” (the U.S. is officially in Wave #3? BBC).)
If renal dialysis can be delivered in a strip mall, why not COVID-19 care? Florida has taken a step in the direction that I suggested nearly 1.5 years ago. From https://floridahealthcovid19.gov/monoclonal-antibody-therapy/ :
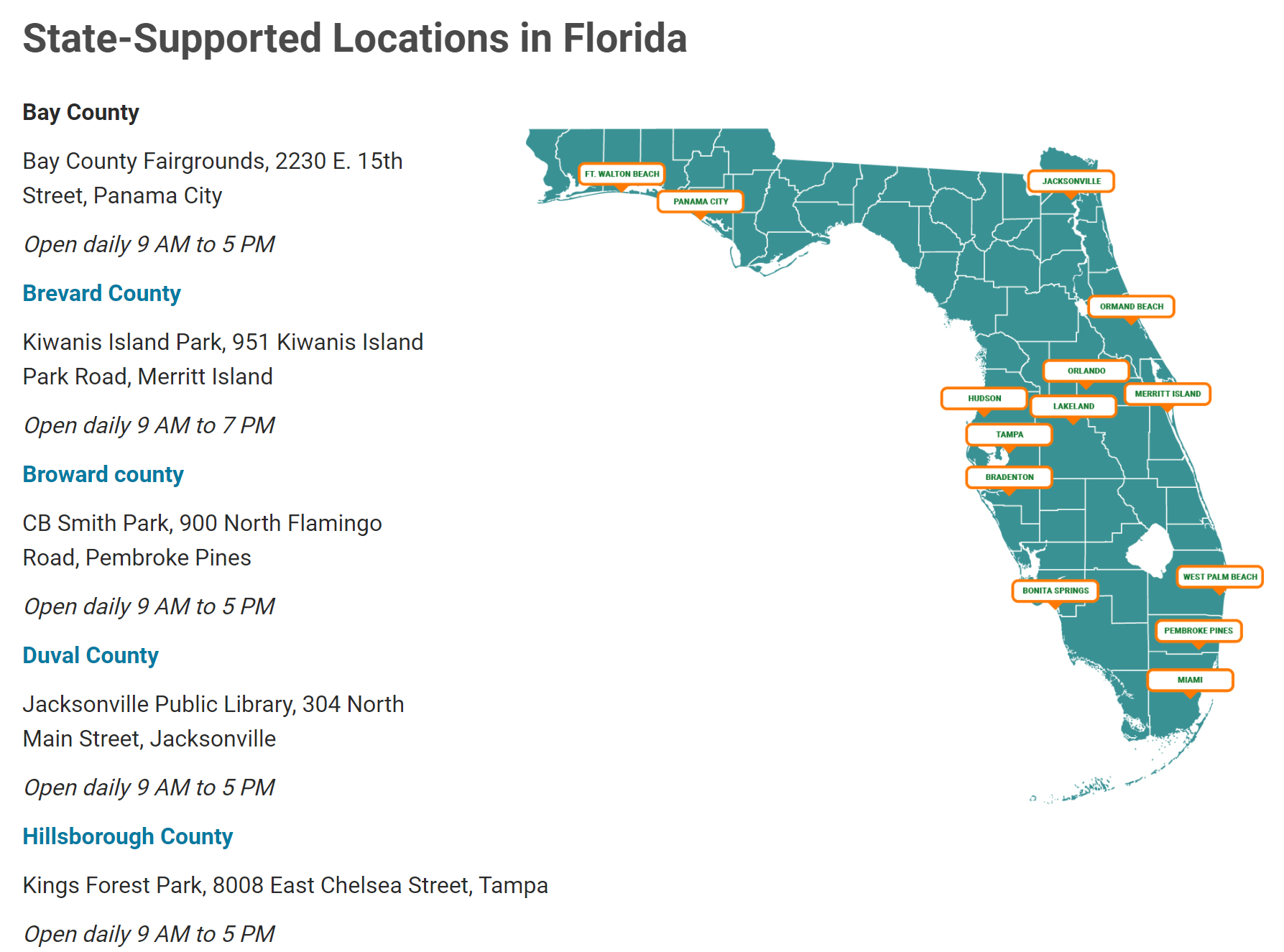
Note that the locations are not hospitals. They’re not empty strip mall shops or big box stores as I’d expected, but rather parks and libraries (i.e., existing state-owned facilities). But maybe this is because these are the state-run operations rather than private sector. (Also, as far as I have seen, South Florida isn’t in the Zombie Apocalypse retail vacancy situation that Boston is.)
Also, I wonder if the 9-5 hours support my analogy between the Vietnam War and our War on COVID-19. We were in a fight where the fate of democracy all around the world was at stake… but the upper-middle class back home kept playing tennis and golf and President Johnson and Congress kept larding on social welfare programs without considering the cost. Right now we’re in an unprecedented emergency. Our best and brightest technocrats are using advanced technology and trillions of dollars against an enemy that has already killed more Americans than all wars combined… but we will fight the enemy from 9-5. (I don’t think this is completely fair because the Florida state government has treated COVID-19 as a respiratory virus to be managed like the flu, not as an entirely new phenomenon nor as something that can be vanquished by government action.)
Smart Americans have been treating their Covid-19 at big box feed and grain stores for at least a year now. No hospital needed. Allegedly better results than most hospitals.
Not a respiratory virus: an epithelial virus that spreads through respiratory aerosols.
Otherwise, a good idea.
A better idea: the Florida AG should bring charges against the people who approved and funneled US Tax money to fund Gain of Function research on bat coronaviruses at the Wuhan Institute of Virology.