How is Sweden doing with coronaplague?
I like to check in on forecasts versus reality at three-week intervals. Maybe prophets are getting better!
Previous posts:
- https://philip.greenspun.com/blog/2020/05/24/did-doom-visit-the-swedes-yesterday-as-planned/
- https://philip.greenspun.com/blog/2020/05/03/doom-for-the-wicked-swedes-is-always-three-weeks-away/
- https://philip.greenspun.com/blog/2020/04/12/everything-the-gleeful-journalists-said-would-happen-to-sweden-has-happened-to-massachusetts/
From the first of those…
What’s the latest from the prophets at IHME? As of a May 20 update to the forecast, Sweden will have a gradually declining daily number of deaths, in more or less the same shape as still-shut-down Massachusetts. A total of 5,129 Swedes will die from/with Covid-19 (roughly one third the previous forecast). The virus will simply burn itself out, apparently, despite Sweden’s lack of shutdown. (But in other countries, the same shape decline will be attributed to a multi-month shutdown?)
That forecast for Swedish death was down from the 13,529 number in the early April forecast. As of June 5, 2020, the IHME model forecast 8,534 deaths for Sweden and the deaths will come in a Bactrian camel shape:

The forecast from June 5 predicts 60-70 deaths per day right around now. What are we seeing? Europeans refuse to work on weekends, so the reported deaths are zero for Saturday and Sunday. Even today’s report shows 0 deaths (so maybe tomorrow’s report will actually reflect three days of deaths?). The Friday report shows 12 new deaths reported in Sweden.
[Update: The Tuesday report included 69 new deaths. So that’s 81 new deaths spread over 5 days of reports (12+0+0+0+69) or 16 deaths per day compared to the forecast 60-70. In other words, the forecast was wrong by 4X.]
(Also from the Tuesday reports: Sweden has suffered 5,122 deaths from its population of 10 million. Massachusetts has lost 7,890 from its population of 7 million. In Month 4 of Shutdown, the Massachusetts rate is 2.2X Sweden’s.)
What about the former chief scientist of the European CDC who, when put on the spot, tossed out that coronaplague wouldn’t be worse than a bad flu season in terms of death? (note that assumptions regarding population fatality rate were not important for the Swedish plan; assumptions regarding the practicality of a non-Chinese country significantly changing the trajectory of infections were)
A bad season indeed was 1957-8, in which up to 116,000 Americans died out of a population of 172 million (compare to 330 million today). Applying that rate to Sweden’s 10 million people, 6,744 Swedes would succumb to Covid-19.
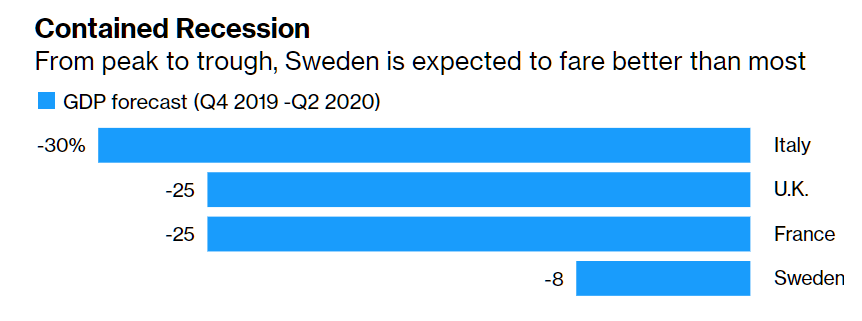
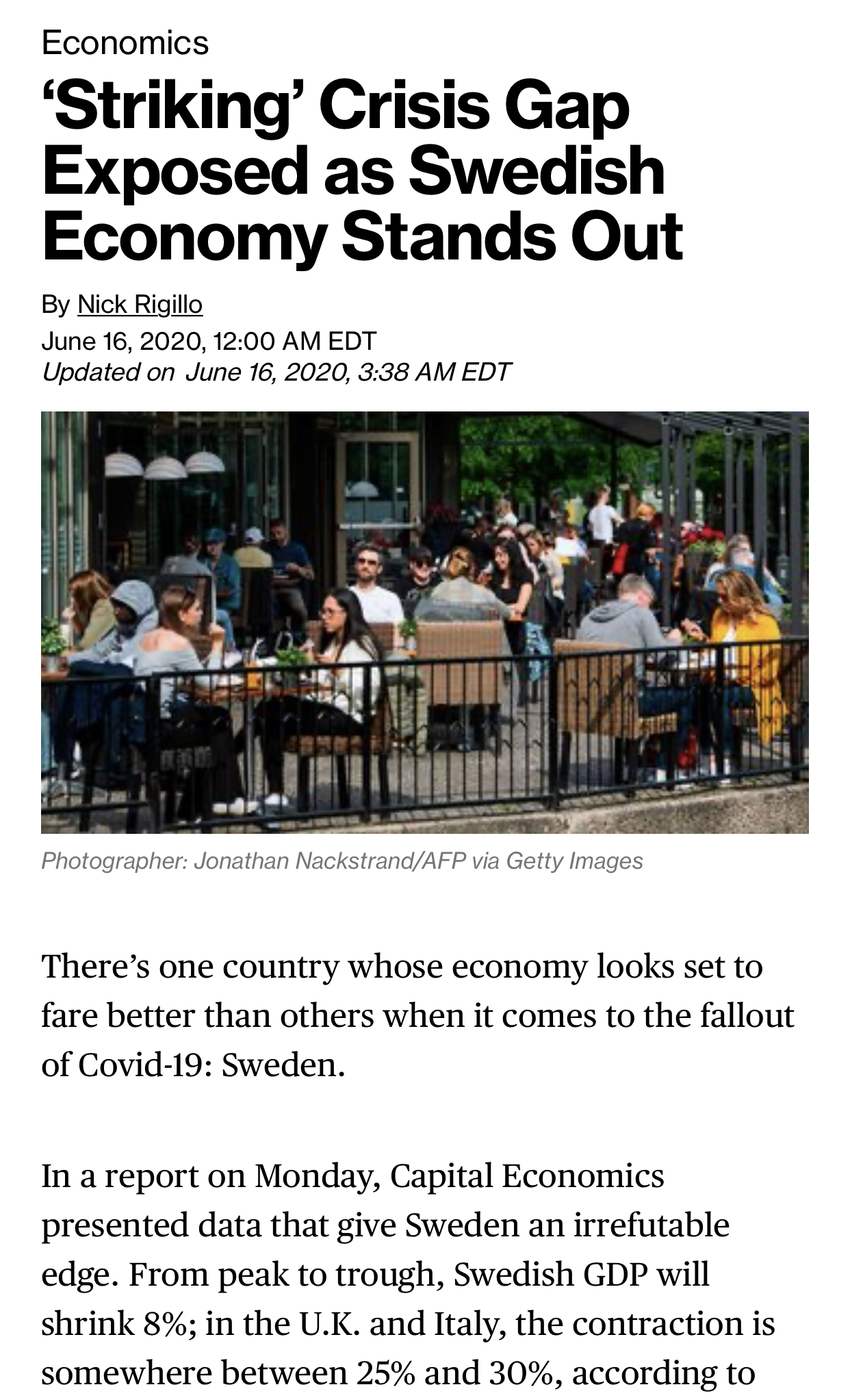
I don’t think economic arguments are highly relevant in a world where people seemingly care only about clinging to life. Nonetheless, since poverty often determines health outcomes: https://www.bloomberg.com/amp/news/articles/2020-06-16/one-economy-stands-out-as-crisis-reveals-striking-differences? (see “Most gunshot wounds are self-inflicted, coronaconomy edition”)
Readers: What’s your best guess on Sweden? How will the death rate from/with Covid-19 compare to the U.S. rate by early 2021? (right now the U.S. has roughly 71 percent of the death rate compared to Sweden, so the U.S. is better if we measure only by this one number)
[Update 6/24: the IHME prophets have released a new projection.

Instead of the Bactrian camel, Sweden is now on the dromedary shape. There is a new “what if?” capability in this model. For example, if only 10 million Swedes would put on masks, 2 lives would be saved on September 1. (but how many would be killed in car-pedestrian accidents due to fogged-up eyeglasses from the masks?). 5,754 Swedes will meet their end due to Covid-19 through October 1, 2020, a population fatality rate of nearly 0.06 percent.]
Related:
Full post, including comments