The problem with socialism is that it was never given a fair chance or a proper technocratic implementation, e.g., in the Soviet Union. Once President Harris or President AOC appoints properly credentialed agency heads, American Democratic Socialism will serve as a City on a Hill-style demonstration to countries around the world.
My Facebook feed is alive today with Bigger Government enthusiasts decrying the fact that state health departments (New York’s has more funding than the entire Russian military, but our media characterizes these departments as “chronically underfunded”) are not managing to distribute the vaccines that the Feds shipped to them. Presidents Biden and Harris will fix the problem starting on January 20, according to my friends, but we are still left with three weeks of what is, in their view, incompetent and slow distribution (at current injection rates, the U.S. is on track to lose 40% of the paid-for vaccines to expiration).

(Note that New York and New Jersey collect more in state/local taxes, as a percentage of residents’ income, than 47 other states, but they’re still on track to have expired vaccine doses.)
An interesting aspect of this is that the failure of central planning for vaccine distribution has not dimmed anyone’s enthusiasm for more central planning in other parts of the economy. The solution for dealing with scarcity is not a market and prices, but rather more and better technocrats.
Separately, I’m wondering how anyone who has recently gotten a flu shot in the U.S. thought that this would go quickly. From Do they still line up kids at school and give them shots? (2018):
The other day I was waiting for a friend at CVS so decided to use the time to get my “free” (i.e., included in my $10,000/year Obamacare policy) flu shot. Ten minutes later my friend showed up. It took roughly another ten minutes before the shot was “ready.” It turned out that three health care professionals had to process various forms on a computer screen, get a one-page questionnaire from me, and finally deliver the shot with a simple needle (less than one minute). A licensed pharmacist was required as part of the paperwork pipeline.
I wonder if something more like a market economy could have done this better. The bureaucrats can send free vaccine doses to hospitals, medical and dental offices, and nursing homes. Whatever is left over goes to whatever clinic or facility bids the highest. The bidding process is necessary to ensure that clinics that have the most streamlined and efficient procedures are the ones who will get the vaccine and also to ensure that clinics won’t let doses get spoiled or expire.
The auction-winning clinics and facilities can then use conventional web-based services to let people book slots and pay for vaccines at whatever prices they want to charge. Presumably the people who are at highest risk will recognize their risk and be willing to pay the most.
The obvious objection to the above is fairness. Rich people who aren’t scared of the barely tested vaccines will happily offer their Platinum cards. But maybe this is actually good from an epidemiological and economic point of view. Rich people tend to travel a lot (via private jet, of course, and including internationally throughout all of 2020) and, if the vaccines do stop transmission, vaccinating them will slow down the pandemic. Those rich people who are vulnerable and/or especially fearful and who have therefore been hiding in oceanfront bunkers will go out and spend a lot more money once vaccinated.
We could deal with the unfairness by simply sending out money to the people whom we want to get vaccinated. Use payroll data to send out checks to essential workers. Use Social Security data to send our checks to old people. Use insurance claim (including Medicaid and Medicare) databases to send out checks to those with BMIs over 30 (goal!) or other health conditions. The check recipients could decide whether to stay bunkered, N95-masked, bathed in hand sanitizer or to use the check to pay the going rate for the vaccine.
At least to judge by my Facebook feed, there are a lot of suburban white and Asian Americans who feel that the cost of lockdown is negligible. They’re happy to work from home (4,000 to 6,000 square feet), order deliveries, refrain from socializing in person. These folks don’t need a vaccine because if the government recommends that they stay home for the next 5 years they will cheerfully comply. But, on the other hand, there is no central database of the Happily Shutdown. Thus, the market would be the best way to keep these folks from clogging up the vaccine line. They know that they’ll be home for another year or two, so why should they pay $500 for a shot? They’ll wait for the price to come down to $100.
Update… We can watch the needle sticks unfold in real time:
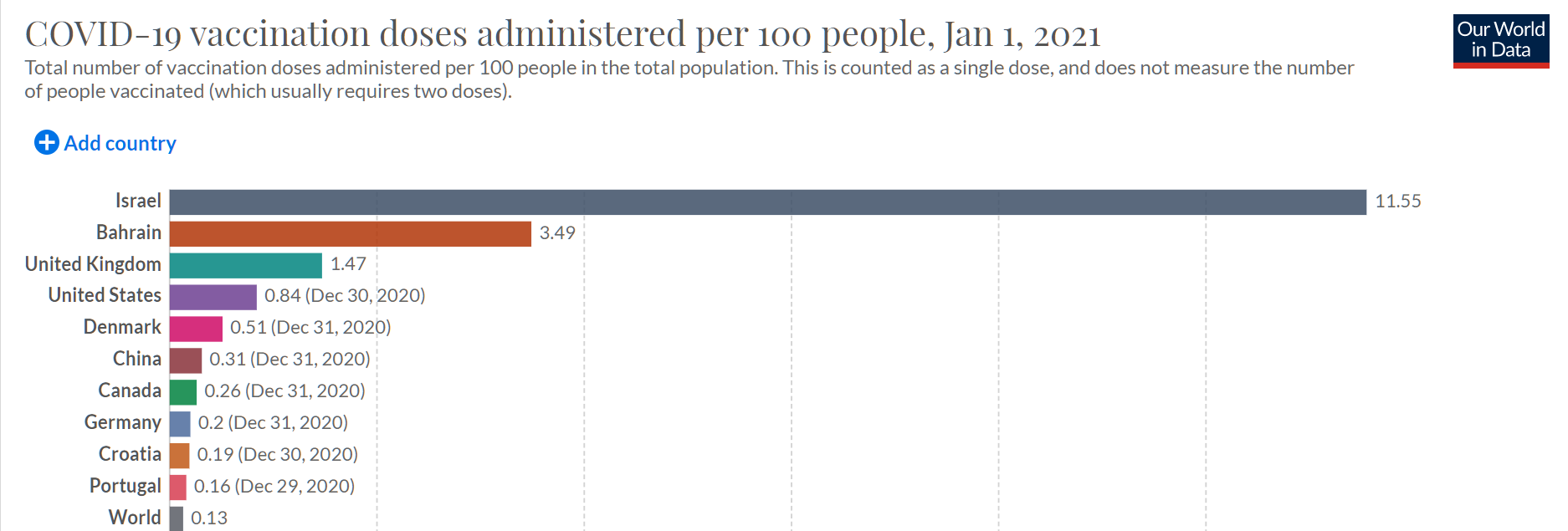
Universal health care is plainly way better than whatever we want to call our system, since Israel, Bahrain, and the UK are well ahead of us. Also, universal health care is plainly way worse than the U.S. system: Denmark, Canada, Germany, Italy, and France are way behind us.
Second Update: We could also run this as a bounty-based system. The government gives away the vaccines to existing state-licensed clinics, such as CVS MinuteClinic, etc. Then the government says “You get $500 for every person over 80 whom you inject, $250 for every person over 70, and $100 for anyone else. There is a bonus of $200 for every shot in a person with a BMI over 40 and $100 for everyone with a BMI over 30.” Would we have vaccines expiring in freezers? The FAA did this with pilot briefings back in the 1980s. They let two contractors compete to offer computer-based weather information to pilots so as to discourage pilots from calling human briefers. The two contractors ran advertisements, enhanced systems, built web versions at around the same time as Amazon launched, etc. Other than writing checks, the FAA never had to do anything to get people to switch to briefing via computer system other than open up an API on their mainframes.
Related:
- “Here’s Why Distribution of the Vaccine Is Taking Longer Than Expected” (NYT): Health officials and hospitals are struggling with a lack of resources. [18% of GDP is not sufficient to run a health care system] In Puerto Rico, last week’s vaccine shipments did not arrive until the workers who would have administered them had left for the Christmas holiday. [Coronaplague is an emergency, but not such a serious one that people should work through traditional vacation periods] In one notable blunder, forty-two people in Boone County, W.Va., who were scheduled to receive the coronavirus vaccine on Wednesday instead were mistakenly injected with an experimental monoclonal antibody treatment. [18% of GDP is not sufficient to run a system in which people get the intended shots]
- Roughly half of the front-line health care workers whom the central planners targeted for #1 priority don’t want to be early adopters of these vaccines and are refusing to be injected: NBC
- Update: a reader pointed me to “Free Market Vaccines”, a December 7, 2020 post by the always interesting John Cochrane: economics should start with “to the highest bidder,” and come up with some well documented market failure, and a public allocation system that mimics the highest bidder allocation. … In India, meanwhile, that bastion of… informal.. if not free markets, it appears you can sign up to buy the vaccine, for about $8.”
As with all good communist regimes, here in New York, our elected officials are cracking down on capitalism playing a roll in vaccine administration. Providers and recipients are subject to potential million dollar fines if they do not follow ever-changing capricious executive orders.
https://nypost.com/2020/12/28/gov-cuomo-ag-to-probe-vaccine-fraud-vows-1m-fines/
Happy New Year! L’Chaim!
Hey Philip, Looks like American Indian, Black and Hispanic groups are experiencing higher rates of Covid-19 related effects. How well would your proposals work for those groups?
Rate ratios compared to White, Non-Hispanic persons
1. American Indian or Alaska Native, Non-Hispanic persons
2. Asian, Non-Hispanic persons
3. Black or African American, Non-Hispanic persons
4. Hispanic or Latino persons
Group 1. 2. 3. 4.
Cases 1.8x 0.6x 1.4x 1.7x
Hospitalization 4.0x 1.2x 3.7x 4.1x
Death 2.6x 1.1x 2.8x 2.8x
https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-race-ethnicity.html
Patrick – that is where philg’s hyper-efficient new government-agency-in-charge-of-handing-out-money-to-the-most-deserving-so-they-can-buy-the-vaccine-on-the-free-market comes into play!
@LinePilot, thanks, now it’s all clear to me! Except for maybe a few small details on how to determine who should get the money and how much.
Patrick: This is easily dealt with under the system proposed in the original post. If you believe that the groups you’re talking about have a vulnerability to COVID-19 that isn’t captured via the other factors (being on a payroll as an essential worker, BMI, diabetes or other disease in the medical claims database) then use the recently completed 2020 census data to send out extra cash purely based on self-identified race.
(It is a lot easier to work with a computer database and a check printer than it is to work with vaccine that has to be refrigerated, administered before it expires, etc. The government already has multiple agencies that work with these databases and send out checks. The Social Security Administration and IRS being the most obvious examples. If new software is needed rather than an extra SQL JOIN on existing systems, just bring in the Obama administration officials who oversaw the healthcare.gov IT systems.)
“Whatever is left over goes to whatever clinic or facility bids the highest. The bidding process is necessary to ensure that clinics that have the most streamlined and efficient procedures are the ones who will get the vaccine and also to ensure that clinics won’t let doses get spoiled or expire.”
How likely is it that the facilities bidding the highest will be concentrated in the neighborhoods with the highest rates of Covid-19 effects? Or maybe part of the formula is accounting for the costs that be required to travel safely from neighborhoods where the high risk populations live to the high efficiency facilities? Then there’s the logistics of routing people from high-risk neighborhoods to the facilities with the vaccine supplies.
Sorry Philip, I only saw your parenthetical remarks after I posted my last message, which addressed my admittedly minor quibbles. Obviously this is a serious proposal that you’ve put a lot of thought into!
Patrick: My proposed system isn’t perfect, I’m sure. And people wishing to be vaccinated may have to rely on roads, automobiles, and public transit. But that’s also true of a centrally managed system. The advantages of my proposed system are that the vaccine gets moved from refrigerators to bloodstreams substantially faster and that wastage due to expiration is minimized. If you believe that vaccines are effective at slowing transmission and saving lives, therefore, you should, I think, be happier with my system than with a more equitable system that is slower. If vaccinating people faster reduces COVID-19 prevalence in the overall population then it should also protect the non-white people you’re concerned about. (An American of color cannot be protected from COVID-19 by a vaccine shot that sits in a state public health department refrigerator until it expires.)
Another possible tweak to address your concerns would be to say that we use a market system, but exclude anyone who appears to be white (as measured with a color meter if we want this to be objective) from being vaccinated. So we still get high efficiency for vaccine distribution and we don’t waste doses on the white people who themselves constitute a pernicious plague in American society (see https://www.apha.org/topics-and-issues/health-equity/racism-and-health/racism-declarations and https://www.usatoday.com/story/entertainment/books/2020/12/01/ijeoma-oluo-mediocre-book-white-male-america/6466188002/ ).
@philg The point I was trying to make – evidently poorly – is that a bidding system to allocate vaccine supplies to facilities may have additional costs or lower level of service due to the possibility of less than optimal locations of the winning facilities. In particular that might be true for high risk populations, but the distribution of winning facilities could easily be highly uneven – to the detriment of other neighborhoods as well.
Patrick: I do love your thinking. COVID-19 is a public health emergency, which is why schools need to be closed for a year or two or three. But it is not such a severe emergency that anyone should be expected to travel beyond his/her/zir/their immediate neighborhood in order to be vaccinated against this deadly pathogen that has already infected 160 million Americans (20 million lab-confirmed “cases” times the CDC’s multiplier of 8; https://www.npr.org/sections/coronavirus-live-updates/2020/11/26/939365087/government-model-suggests-u-s-covid-19-cases-could-be-approaching-100-million ) and may soon harvest 170 million additional souls.
Market solutions are highly-efficient mechanisms for delivering services – especially in emergency situations. Toilet paper supplies back in March, for example.
@philg When vaccines can be efficiently delivered to people’s workplaces and residences, as in the initial distribution to health care workers and nursing homes, the cost and efficiency *should* be reasonably high. But once you have to start routing people to facilities out of their familiar neighborhoods, the cost / level of service could be significantly worsened.
@philg I love your thinking too! A health emergency is the perfect time to require people to travel long distances to unfamiliar places.
Patrick: It would be like everything else in American retail and services. There would be a huge concentration of potential buyers with money in, say, downtown Boston. Yet all of the suppliers would be a 2-hour drive away in Pittsfield, Maskachusetts. That is how the market works and why central planning yields far superior matching of buyers and sellers.
(One of our neighbors actually did have to drive to Pittsfield recently in order to get something done with the Massachusetts Registry of Motor Vehicles. There were no available time slots at any closer RMV and the RMV had not established procedures for doing what she needed via mail or Zoom. So it was an all-day odyssey for her and her boyfriend.)
@philg Everyone from Boston must get their vaccinations in Pittsfield? 135 miles away? Sounds like a plan!
> I’m wondering how anyone who has recently gotten a flu shot in the U.S. thought that this would go quickly
I got my flu shot at Kaiser in Richmond, CA a couple months ago. They setup the workers in an empty parking garage, you drive in, show your card, and stick your arm out the car window. Somebody puts a needle in your arm and presses the plunger, and then you drive away. It was less than 3 minutes from when I drove up to the parking garage to when I drove out.
This just isn’t that hard, it is simply a failure of will to do the job. I don’t see anything that needs to be done that isn’t well understood.
@SK: I agree, I’m surprised Philg even had to think up this post. I’ve been tested for COVID three times now in tents like you mention and I would have thought that once the vaccine was available at hospital locations things would go much more smoothly.
SK: South Dakota, Montana, North Dakota, Nebraska, and West Virginia are obviously doing something like what Kaiser set up. They’ve administered more than half their vaccine doses (https://www.bloomberg.com/graphics/covid-vaccine-tracker-global-distribution/ ). But California is at 22.8% right now. I.e., 4 out of 5 vials sent to California are sitting in a fridge. Bad as the traffic is in Los Angeles, I think it should be easier to reach people in California than in Maine or South Dakota.
https://nymag.com/intelligencer/article/americas-vaccine-rollout-disaster.html says that, at the current pace being set by the states, 6 out of 10 million doses will be administered before the vaccines expire.
One problem with central planning, even if executed perfectly, is already apparent. Roughly half of the front-line health care workers whom the central planners targeted for #1 priority don’t want to be early adopters of these vaccines and are refusing to be injected: https://www.nbcnews.com/news/us-news/many-frontline-workers-refuse-covid-19-vaccines-distribution-rollout-struggles-n1252617
The problem is that 18 percent of GDP is not sufficient: “Health officials and hospitals are struggling with a lack of resources.” https://www.nytimes.com/2020/12/31/health/vaccine-distribution-delays.html?action=click&module=Spotlight&pgtype=Homepage
(same article reminds us that it is an emergency, but not such a serious one that people should work all through December: “In Puerto Rico, last week’s vaccine shipments did not arrive until the workers who would have administered them had left for the Christmas holiday.”; this is my favorite though: “In one notable blunder, forty-two people in Boone County, W.Va., who were scheduled to receive the coronavirus vaccine on Wednesday instead were mistakenly injected with an experimental monoclonal antibody treatment.”)
Alex: Here in eastern Maskachusetts, getting a COVID test requires visiting hundreds of web pages in hopes of finding an available testing location/time slot. Once secured, usually 2-4 days later, the actual test is a straightforward drive-through process. As an experiment, I just now went to the Project Beacon web site in which samples are sent to the Broad Institute (supposedly massive capacity). It was impossible to make an appointment. All five locations say “No upcoming times are currently available for this location”.
@Philg:
That’s a good point. I’ve been able to get tested easily because I appointments to be in a hospital. It was very easy then – I was scheduled immediately, told exactly where to go at what time, and the results *had* to turn around quickly because otherwise, I couldn’t go into the hospital for the procedure.
I’m wondering now whether the Governor’s vaccination roll out plan is going to work at all? It’s all right there on the Mass.gov website, but how does anyone know where to go and what to do? It’s just a picture and a link that takes you to another page. There’s no way to check which tier you’re in, find a place to get vaccinated, etc.
I don’t know for sure, but it looks to me like the Baker-Polito Administration has the plans, but don’t really care much about the implementation. Until after the inauguration.
https://www.mass.gov/info-details/when-can-i-get-the-covid-19-vaccine
They’re all dragging their feet for Biden so that he can achieve his “100 million doses in 100 days” pledge, with the accompanying funding.
You have to realize, it’s not counting the vaccine availability that matters. It’s those who count the doses administered. It must be unequivocal: the Biden Administration MUST save the United States from COVID-19 and all the malfeasances and incompetence of the Trump Administration. It’s going to be a very clear, bright line.
@Philg: If you really think about it, what do people like the equivalent of Fauci in all 50 states *DO* all day long? Most of the leg work is delegated to functionaries. What they mostly do is sit around and think about how the politics are going to play out. They read polls, they read the news, they talk to their higher-up politicos and they plot strategy to save their jobs and funding. This isn’t about efficiency or helping people not get sick, it’s about who is going to get the credit, and who is going to get the money.
YOU have probably done more honest work in terms of epidemiology and all the other aspects of COVID than anyone in the higher echelons of government has. They don’t sit around and think about this stuff all day long. They think about who is going to get the credit and the blame.