A friend’s daughter in NYC is soon to turn a disposable fetus into a precious baby. This transformation will cost her $5,000 out of pocket. She couldn’t find an ob-gyn in Manhattan without agreeing to the “concierge” plan and says that this is the direction of primary care in the city. In Maskachusetts it was difficult to find a primary care physician who was taking new patients and waiting times to see specialists were generally measured in months if not seasons. Florida is, if anything, even more stressed. Americans fleeing lockdowns have been disproportionately not doctors. A doctor who wanted to escape Andrew Cuomo would have had to get licensed in Florida, which is a complex process, and then build a practice here. Compare to a laptop-based worker who could pick up and move over a weekend.
Can waiting a few months to see a doctor result in death? Yes, concludes “Delayed Access to Health Care and Mortality” (2007):
Veterans who visited a VA medical center with facility-level wait times of 31 days or more had significantly higher odds of mortality (odds ratio = 1.21,p = 0.027) compared with veterans who visited a VA medical center with facility-level wait times of < 31 days.
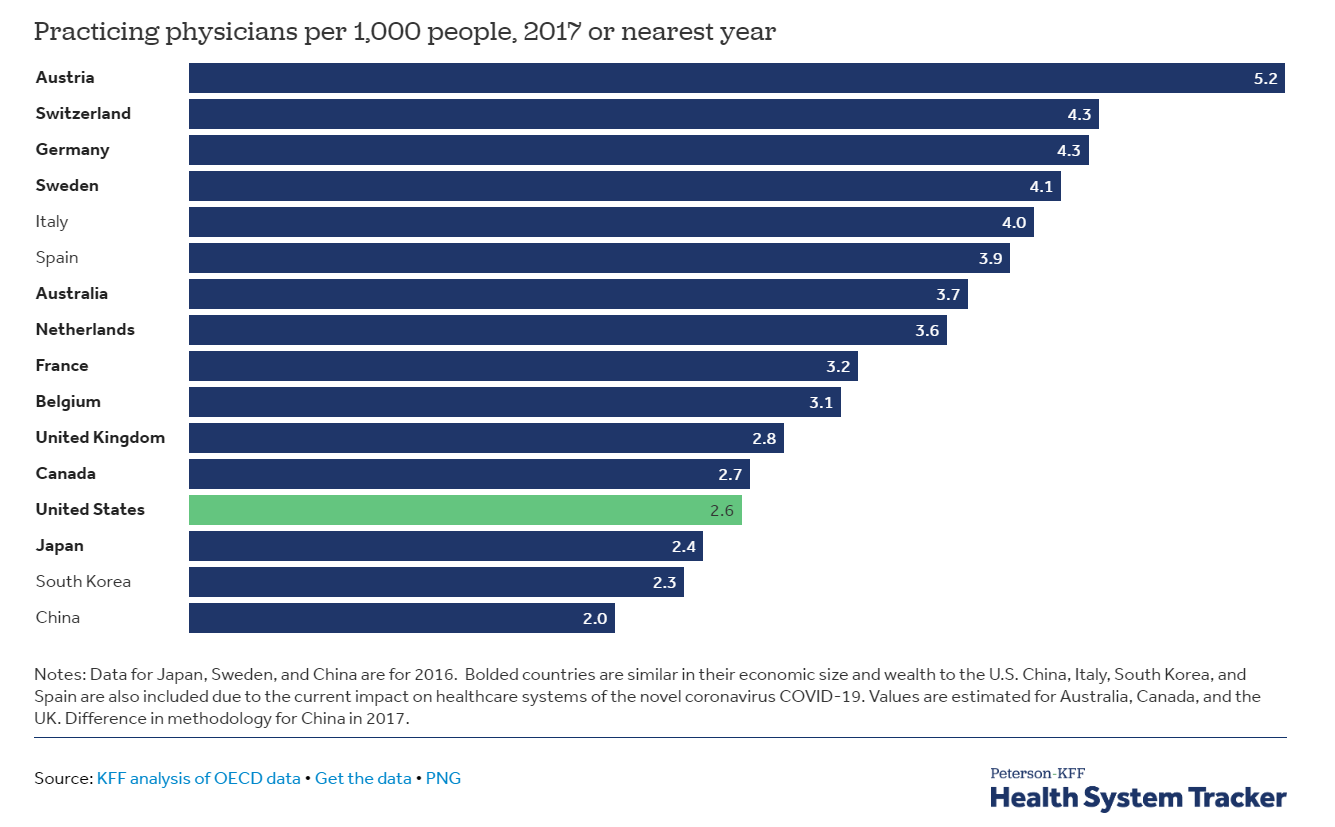
“The U.S. Has Fewer Physicians and Hospital Beds Per Capita Than Italy and Other Countries Overwhelmed by COVID-19” (KFF, 2020) includes a chart with 2017 data:
Our World in Data shows that there was an upward trend from 1960 to 2004, as the U.S. became wealthier and medicine more advanced, but now we’re in a downward trend as our population expands via low-skill immigration.
Maybe the shortage of docs can be addressed via using non-doctors to do what doctors in Switzerland, Germany, and Sweden do? The trade union for docs says this doesn’t work… “3-year study of NPs in the ED: Worse outcomes, higher costs” (AMA):
Nurse practitioners (NPs) delivering emergency care without physician supervision or collaboration in the Veterans Health Administration (VHA) increase lengths of stay by 11% and raise 30-day preventable hospitalizations by 20% compared with emergency physicians, says a working paper published by the National Bureau of Economic Research.
Overall, the study shows that NPs increase the cost of ED care by 7%, or about $66 per patient. Increasing the number of NPs on duty to decrease wait times raised total health care spending by 15%, or $238 per case—not including the cost of additional NP salaries. In all, assigning 25% of emergency cases to NPs results in net costs of $74 million annually for the VHA.
They don’t bother to try to figure out whether the patients lived or died or what quality of life they might have experienced, but it seems safe to say that “preventable hospitalizations” are not beneficial.
Rich people can buy their way out of waiting to see primary care docs and, perhaps, a handful of specialists who are affiliated (or bribed?) by a concierge practice. A 50ish friend in Boston pays $8,000/year for this. But even the rich may experience a long wait if they need to see a specialist outside of their concierge network.
There have been some recent articles decrying a decline in U.S. life expectancy (example from the public health folks at Harvard, taking a rare break from their mask and COVID-19 vaccine advocacy). But none mention population growth combined with relative stagnation in the number of physicians.
Related:
- Shopping for health insurance on healthcare.gov (in which I learn that Medicaid is much better than even the $60,000/year Obamacare policies if you want to see top specialists)
You are absolutely right. The very artificial shortage of physicians in the US is a well-known phenomenon. So why there is no widespread outrage about it? I think it is a lot easier for groups representing interests that don’t benefit the general public to affect policy in the US than in Europe.
“Physicians are a giant rent-seeking conspiracy that’s taking money away from the rest of us, and yet everybody loves physicians. You can’t touch them.”
Nobel Prize winner Angus Deaton
Tell your friend that is a lot easier to find a good physician in NY or MA than in many other states….
https://www.beckershospitalreview.com/workforce/this-state-has-the-most-physicians-per-capita.html
Large numbers of immigrants are also having an effect on the health care resources of Europe, but they are in a much better situation.
After failing to get accepted into a US MD program immediately after undergrad, a family member attended and graduated from a US Osteopath school over 30 years ago. She was a 10-year employee of a successful family practice in the northeast before being recruited to a position as an Associate Medical Officer for a large, international health insurance company. Eventually earning quadruple what she would have earned as a family doc, and retiring with a very generous retirement package after 20 years in his late 50s.
My government job offers a decent Aetna HMO, $0 premium for the employee on the individual plan. $400/mo employee premium for the family plan. Retiree individual plan for $300/mo.
A Docter fauci might have availability? An expert on Wuhan flu, among other things, I have heard.
I think it is interesting to consider immigration’s effect on the widespread access to healthcare that every American deserves by right. The issue with only looking at immigration in regards to the decrease in healthcare access and quality in this country is you’re missing the problem. Yes, immigration contributes to the amount of people waiting for healthcare. That is a symptom of the actual problem: how our nation handles healthcare (private medicine is a mistake), how it incentivizes (or, in truth, doesn’t) becoming a healthcare professional by placing mountains of debt (for anyone who isn’t already wealthy) between any given healthcare professional and a job that actually pays well, and how it limits access to becoming a medical professional due to rules we have had in place for decades that were originally meant to limit doctors by race using the fact that newly freed slaves had no money to pay for medical school. You compare us to various European who are doing better. Why are they doing better? Socialist policies. There are Asian countries doing even better than that. Why not mention them? Is it because they’re not white? To answer the question posed in the title of this blog post: No, immigrants are NOT killing “native born Americans”, Republicans and the corporations in their pockets are.
Yes, let’s enslave ourselves, become poorer and destroy our culture and identity to more efficiently treat diseases that require over the counter medications. See cancer tourism tourism to USA from Canada and UK, at least pre-coronavirus