Happy International Day of Charity to those who celebrate, especially Californians in the 50.3% tax bracket who could definitely afford to give some more! The UN says that we just need “Global Solidarity to Eradicate Poverty” (recent archive.org version of the page). There is no possibility of non-working humans breeding faster than money and other resources can be transferred from working humans. What kind of language can be used to persuade people who already pay taxes at the highest rates in human history to pay more and, ideally, voluntarily give more?
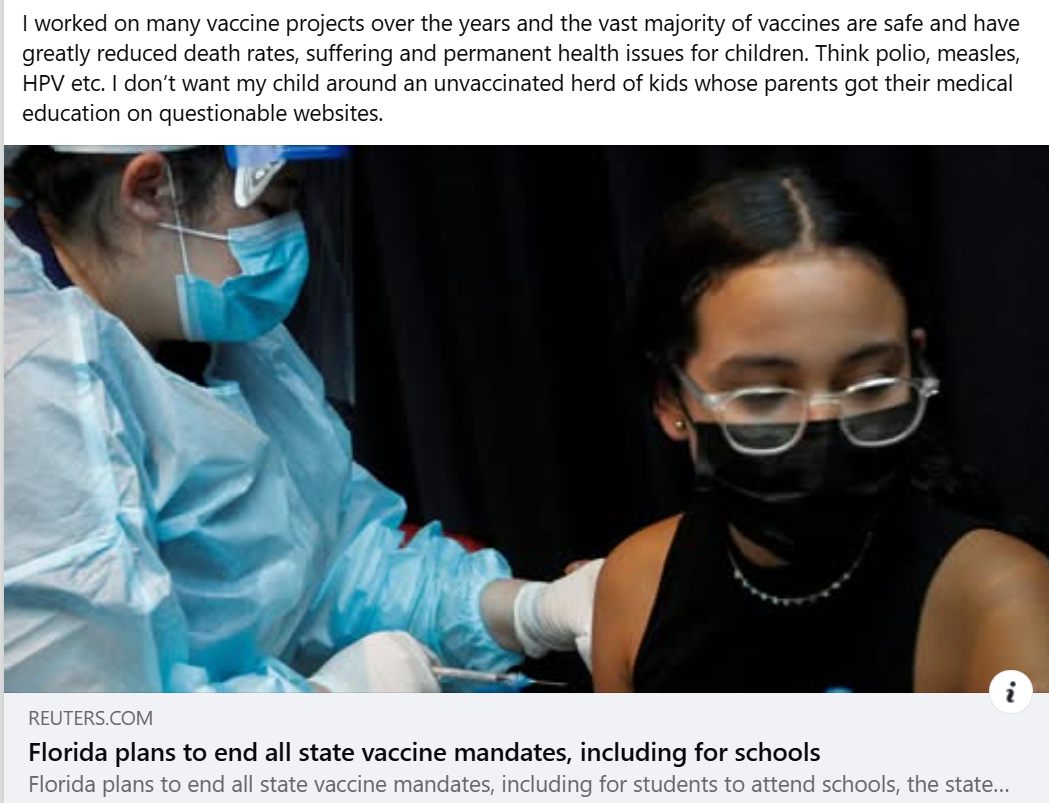
Americans don’t seem to like the idea of a “cradle to grave welfare state” yet that is what a significant percentage of us are in, sometimes for 4 or 5 generations. Right now about 40 percent of American births are paid for by Medicaid (formerly known as “welfare”) and the resulting children are on Medicaid immediately and, most likely, will be on Medicaid for the rest of their lives (health care doesn’t get cheaper; AI and continued low-skill immigration won’t make low-skill Americans more valuable as workers).
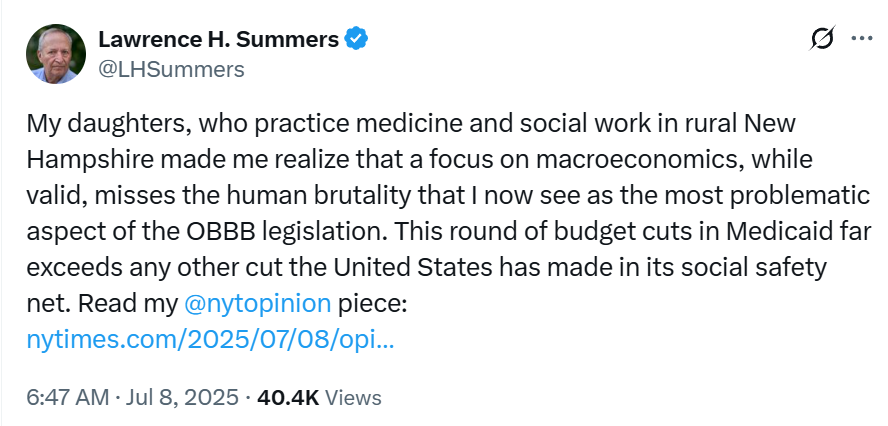
What kind of propaganda could be used to get people to vote for expanding our cradle-to-grave welfare state? How about calling what 40 percent of young Americans are on a “safety net”? You wouldn’t expect 40 percent of performers in a circus to fall into a safety net, but there is no law against using the term to describe what is, in fact, an all-day-every-day thing. Example from the former Treasury Secretary and El Presidente at Harvard:
He uses the term “safety net” three times in the linked-to NYT piece (as a Russian I know says about the NYT, “The difference between Soviets and Americans is that we didn’t believe the propaganda”) to advocate for an expanded cradle-to-grave multi-generational welfare state.
(Prof. Summers lives in Maskachusetts where, in fact, “Forty-eight percent of Massachusetts children are covered by MassHealth, according to a Blue Cross Blue Shield of Massachusetts Foundation report” (source; also says “The largest program in the state’s annual budget, MassHealth is also heavily dependent on money coming from the federal government…” (inequality is bad, but Massachusetts loves to take money away from poorer states by feeding at the federal trough!)).)
How about “dignity”? That seems to be popular now with advocates of transfers from those who work to those who don’t work or from successful hard-working societies to societies in which nobody need work (e.g., the Palestinians). When arguing for an expansion of transfers, one points out that mere survival (basic shelter, food, health care, education for kids) is not “dignified”. What would be dignified is a U.S., Japanese, or Western European standard of living.
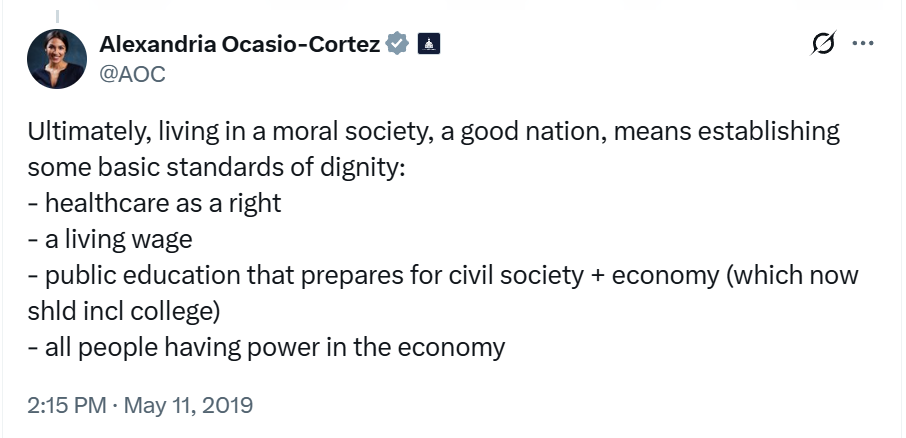
Here’s a 2019 tweet from the Democrats’ thought leader:
“all people having power in the economy” presumably includes those who don’t work.
The UN Secretary General tweets that it isn’t enough for US and EU taxpayers to fund a 100% free basic lifestyle for Palestinians everywhere. If they never work they’re still entitled to “dignity” (in fact it is an “inalienable right” that can’t be forfeited via 75+ years of not working, periodic trips into Israel to kill, rape, and kidnap civilians, etc.):
Actually, according to the UN, all humans who do no work have a right to “adequate housing … and dignity” (source):
An “overcrowded slum” is not dignity. The UN article goes on to say that affordability is also a right:
Affordability: Personal or household financial costs associated with housing should not threaten or compromise the attainment and satisfaction of other basic needs (for example, food, education, access to health care).
The use of “dignity” in connection with building support for welfare state transfers and foreign aid transfers is, I think, fairly new. It seems to be effective also. Who could be against “dignity”?
Full post, including comments