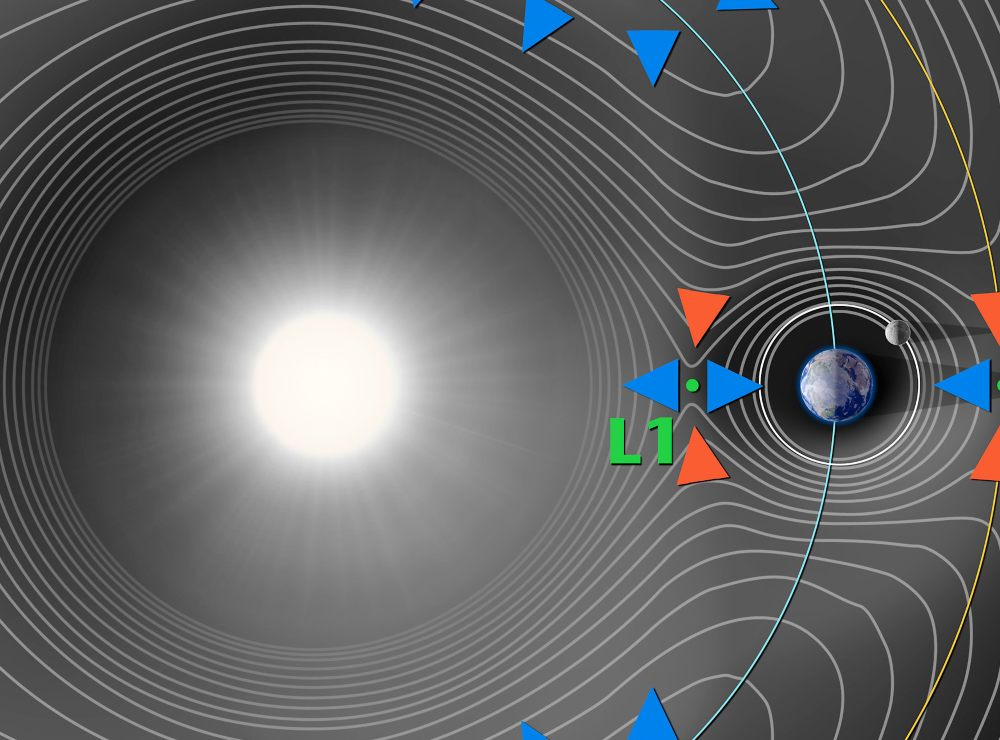
Elon Musk wants to go to Mars on Starship. What can the technology do for those of us who aren’t interested in living on Mars? How about improving our beloved Earth, or at least the biggest and richest cities, via space-based sunshades? If we wanted to help everyone on the planet we could put a 35kTon shield at the L1 Lagrange point (#Science).
But if we’ve learned nothing else from the Climate Change (TM) experts we’ve learned that the climate righteous don’t care about everyone on the planet. Greta Thunberg, for example, cares only about the noble Palestinians (today she sails to Gaza from Spain). Climate change alarmists in New York City were in favor of open borders when migrants invaded Texas and against open borders (“a crisis”) when migrants began showing up in NYC by the busload to claim their right to taxpayer-funded housing.
What about space-based sunshades funded by the richest and most densely packed cities that are aimed at cooling off only folks in those cities and only for the hottest months of the year? Grok says that New York City could be shaded for less than $5 billion. If we assume that 1 million NYC residents (out of 8.5 million) pay non-negligible taxes, that’s $5,000 per taxpaying New Yorker, essentially nothing. It’s also nothing compared to the NYC government’s $115 annual budget. Maybe Grok is wrong about the likely cost? Or Grok is budgeting for 20 years of improvements in technology?
Unlike air conditioning, a solar shade for the elite has the advantage that it will also cool off non-elite regions of the Earth, at least to a small extent. The constellation of sun shades for NYC could move to provide relief to equatorial cities in the spring and fall and then be repositioned to provide shade to Southern Hemisphere cities during their summer. Maybe a city could still hit 95 degrees due to being near a warm air mass, but there wouldn’t simultaneously be a blazing hot sun. Grok says we can get a 3.5-7-degree F local temperature reduction.
Where else could this work? I.e., what other cities tend to be too hot for some parts of the year, are densely populated, and are rich? Singapore, Shanghai, Hong Kong, Tel Aviv (cue the Jewish Space Lasers!), Dubai, Abu Dhabi, Miami, Doha, Tokyo?
Here’s Grok’s answer after I asked about shading all of Florida and then just NYC:
Technical FeasibilityBuilding a space-based sunshade for New York City (NYC, approximately 800 km² land area) that deploys seasonally from June 1 to September 15 is theoretically possible but would require significant advancements in solar sail technology and orbital mechanics. Unlike global sunshades at the Sun-Earth L1 point (1.5 million km away), a city-specific system would use a constellation of smaller, lightweight reflective sails or mirrors in Earth orbit to provide targeted shading. This draws from early concepts like Hermann Oberth’s 1920s-1970s proposals for orbiting mirrors (100-300 km diameter) to weaken solar radiation over specific regions.
Modern adaptations could leverage “statite” configurations—solar sails that balance solar radiation pressure against gravity to “hover” over fixed points, such as high latitudes.
Design and Deployment: A constellation of 10-50 sails (each 10-50 km², depending on orbital altitude) could achieve 20-50% insolation reduction over NYC during summer daylight hours. Sails would use ultra-thin materials (e.g., polymeric films with SiO₂ nanotubes, areal density ~1-4 g/m²) for reflectivity. For seasonal use, sails could be oriented edge-on to the Sun (non-reflective) outside summer, or maneuvered into storage orbits using onboard ion thrusters or solar pressure. Deployment might involve launching folded sails from Earth, unfolding in orbit, and positioning via solar sailing—reaching operational orbits in weeks to months.
Orbital Configurations: To maintain persistent shading over NYC (40.7°N), sails could use inclined geosynchronous orbits (24-hour period) or Molniya-like elliptical orbits to linger overhead during daylight. Statite modes could allow quasi-stationary hovering by tilting sails to counteract gravity, enabling seasonal activation without full repositioning.
Studies on L1 sunshades show orbiting disks can mitigate seasonal temperature variations by ~0.5-1°C globally, suggesting adaptability for targeted summer cooling (e.g., reducing NYC heat by 2-4°C).
Size and Materials: Total sail area might be 500-2,000 km² for effective shading, far smaller than global proposals (3-4 million km²). Advanced sails (reflectance >90%) could minimize mass to 1,000-5,000 tons, deployable via reusable rockets like Starship.
Challenges and LimitationsEngineering and Launch: Solar sail tech is nascent (e.g., NASA’s Solar Cruiser prototype); scaling for precision control over a city requires breakthroughs in attitude control and collision avoidance. Launching via 50-100 missions (at $50-100/kg) could take 5-10 years, with risks of orbital debris exacerbating Kessler syndrome.
Cost: Estimated $500 million to $5 billion, based on scaled-down global figures ($5-10 trillion for planetary-scale).
This includes R&D ($100-500 million), launches, and maintenance. Seasonal operations add complexity, potentially increasing costs by 20-30% for repositioning fuel/thrusters.
Environmental and Ethical Issues: Targeted shading could alter local weather (e.g., reduced rainfall or photosynthesis impacts), affect solar energy production, or cause uneven cooling in adjacent areas. Global governance is needed, as unilateral deployment raises international concerns. Sudden failure (e.g., solar storm damage) could lead to rapid warming.
Current Status: No prototypes exist for regional shading; efforts focus on global concepts via groups like the Planetary Sunshade Foundation.
Implementation might be viable in 20-30 years with investments in reusable launchers and in-space manufacturing.
In summary, while conceptually sound and more feasible than Florida-scale due to NYC’s smaller size, this remains speculative geoengineering. Ground-based alternatives (e.g., cool roofs, urban trees) offer quicker, cheaper relief.
Sustained R&D could make it a complementary tool for urban heat mitigation.
Related:
Full post, including comments