Our schools and cubicle farm offices shut down more than two months ago. Our “non-essential” stores a little less. So I think it is fair to say that today is roughly the day that we in Massachusetts enter our third month of shutdown.
Charts of new cases and new deaths don’t suggest that whatever we did during the first two months of shutdown had much effect on the virus.
How are we doing compared to the Swedes? Our death rate thus far is up to 2.3X what they are suffering in “let the virus burn through the younger than 65 population” Sweden (see “Number of new COVID-19 cases worldwide is declining now?” for my tracking of the numbers).
How about compared to the states with no income tax? Our death rate is 20X that of Texas and Tennessee, 10X Florida’s, 7X Nevada’s, 75X what they have in Wyoming and Alaska.
With the virus failing to live up to its dramatic exponential promise, but also failing to go away, we’re grasping at straws such as a recent governor’s order to fine people $300 who don’t put masks (that are impossible to purchase) on 6-year-old children (who will probably not follow WHO guidance regarding proper use of the mask!).
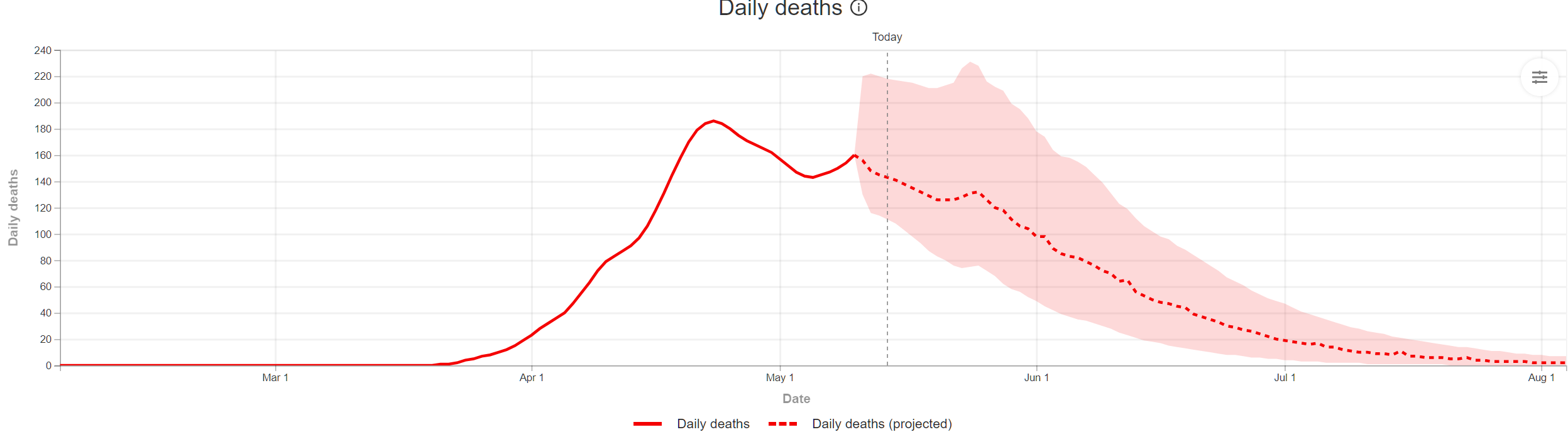
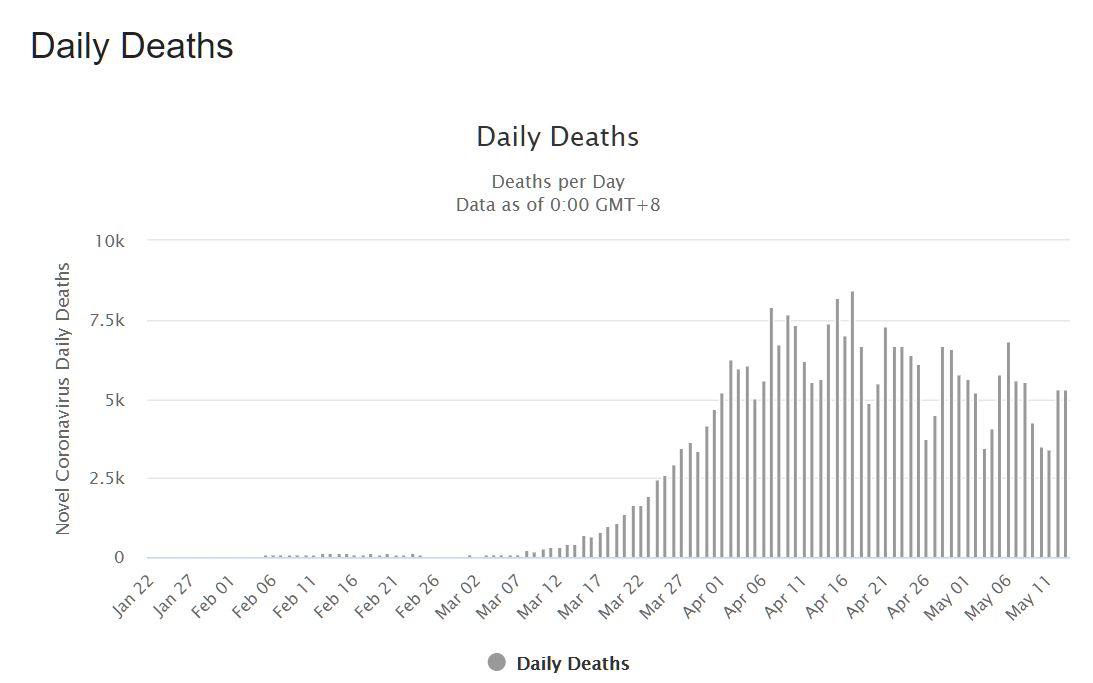
The current IHME prophecy for Massachusetts is 9,629 deaths through early August on a slow decay:
How does this compare to a country with no lockdown? The IHME prophets predict 5,760 deaths for Sweden during the same time period:
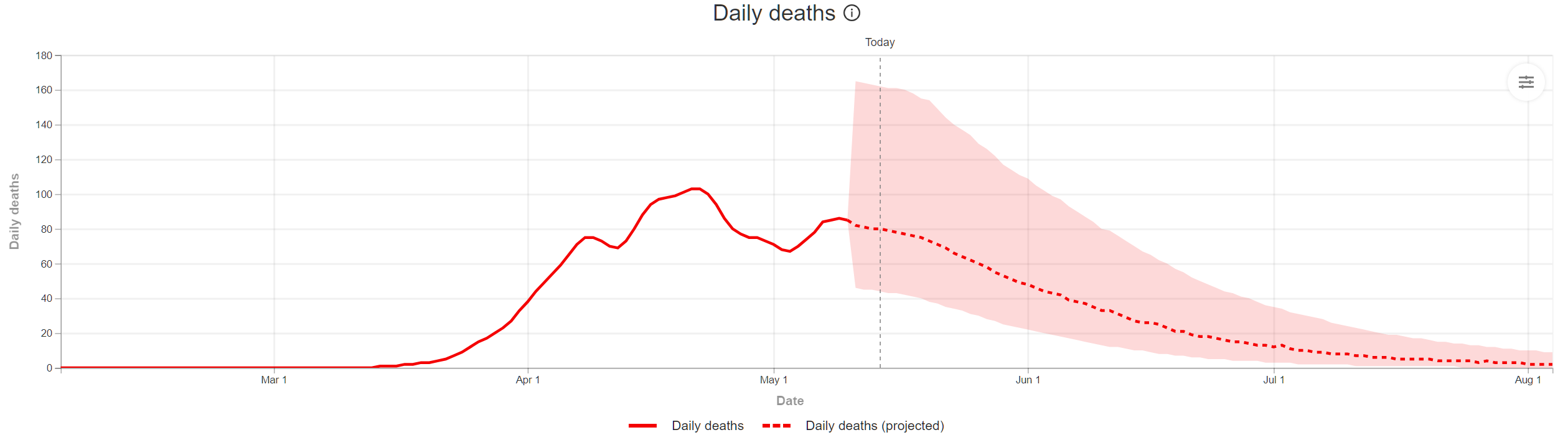
Tough for me to discern a dramatic difference in these shapes (though of course there will be a higher death rate, adjusted for population, in Massachusetts, roughly 2.4X Sweden’s if IHME proves correct).
The slow/steady curve seems to be the virus’s plan for the entire world:
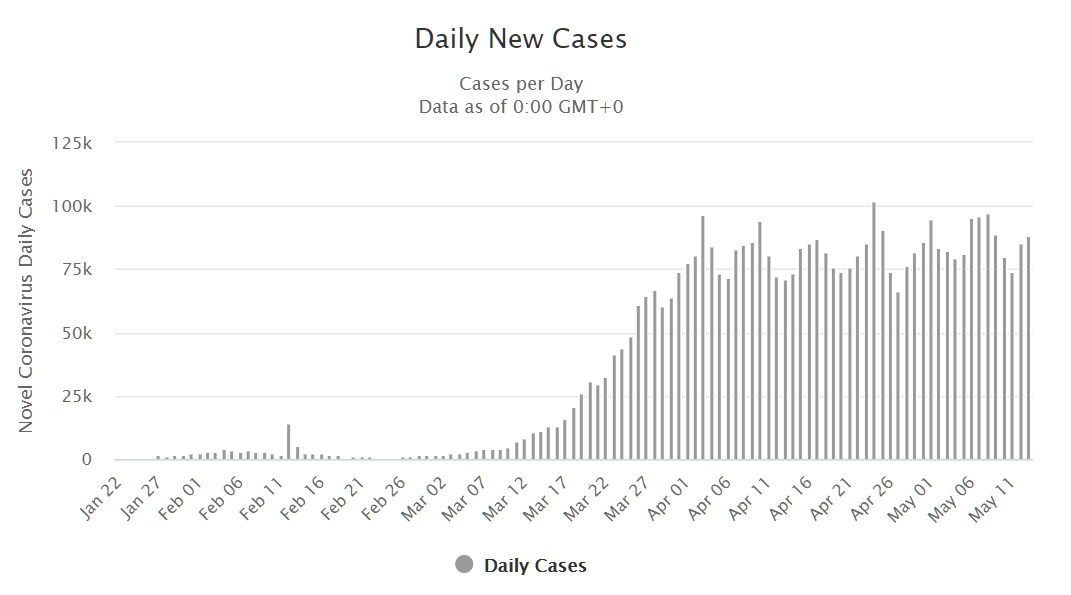
Maybe there is a downward trend visible in deaths, though? The flat graph for new cases is an artifact of increased testing?
Can barely wait for Baker’s speech on Mon. Here is a prediction – “we can sort of not really, maybe soon, reopen somethings but I can’t say which ones, we might allow to open, provided you children keep wearing your humiliation masks. And if I see one person without a mask reopening is canceled and the whole class has to come back inside.”
Obama always says if you like your quarantine you can keep it but if you don’t like it just go outside!
Cool
Huh. I wonder what MA is doing wrong? In Santa Clara County, CA (includes San Jose and much of Silicon Valley) new reported cases have drifted to zero. Maybe because a valley full of tech nerds finds it easy to stay home?
Los Angeles, not so much.
Several differences between Santa Clara County (SCC) and MA: No public transport. SCC has the highest median income in CA, and a higher fraction of people can likely work from home. It looks like there are hardly any long-term care facilities in Santa Clara. SCC started their lockdown when there were a total of about 25 cases in the county. Massachusetts started their lockdown (at the same time) when there about 500 cases. That’s about 20 days worth of exponential growth. If MA had started their shutdown 20 days earlier things would be different here. That’s probably the biggest difference: SCC got to start their lockdown earlier.
Ouch. If there were 500 confirmed cases, there would likely have been several thousand actual infections at that point.
Looks like Massachusetts is planning a more aggressive response. Jim Yong Kim, It’s Not Too Late to Go on Offense Against the Coronavirus.
Given that it’s more an artifact of the testing regime than any evolving reality, won’t “daily new cases” continue to plod along at the politically convenient rate until Drumpf is ejected from office or until there’s no one left to test, whichever comes first?
>until there’s no one left to test
You forget that once tested, people can be re-tested as many times as politically necessary!
Great minds think alike: In a March 10 email, the head of the New York public hospital system argued against closing schools and restaurants, saying that herd immunity would protect people. He Saw ‘No Proof’ Closures Would Curb Virus. Now He Has De Blasio’s Trust.
huh. whodathunkit? DiBlasio made the right call.
New York has some interesting personal dynamics in its politics. Governor Cuomo is largely loathed outside of the state of New York’s cities. Without overwhelming support in New York City, Cuomo would not be Governor. Essentially, Cuomo is the Governor of New York City. But New York City already has a chief executive in the separate person of Bill DiBlasio. Much of New York City governance is dependant on New York State authority (schools, mass transit, and health care, specifically.).
Cuomo and Diblasio personally loathe each other.
New York should split itself into two states, like Virginia did in 1861.
Three things you want to look at:
1. We are doing 2-3x the test volume we were a month ago so the positivity rate is important. In early April we were sometimes around 30% positive. Now it’s more like 15%.
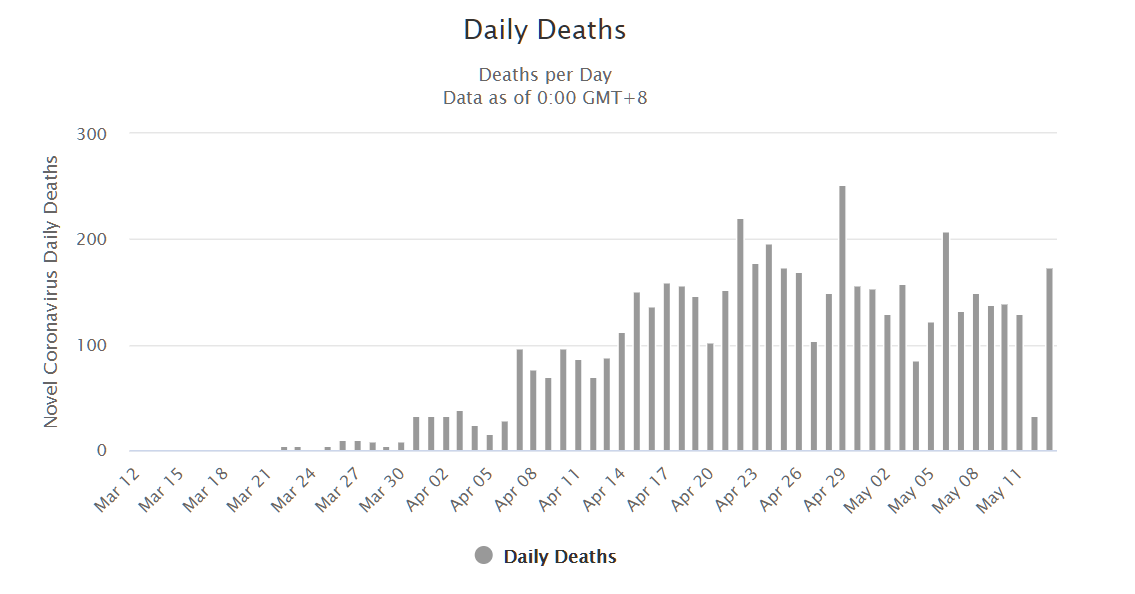
2. Daily deaths reported does not equal daily occurred. Notice the sawtooth pattern? Tuesdays have low reports consistently while Wednesday’s have high. This is an artifact of reporting process. Actual trend is smoother.
3. Number of people hospitalized is a leading indicator of deaths and the hospital population is on what appears to be a steady decline.
Data for 2 & 3 are included in the daily dashboard DPH publishes.
It may be satisfying to be snarky about how poor our governments are, but who didn’t know that beforehand. It’s totally clear that we have inflicted great self harm given what COVID-19 is and that most of us would be dead if it was what it “could” have been. You are a smart guy – why not put your “systems” hat on and put together a post outage action plan. I’ll start –
1-Restrict travel and financial flows to countries that do not have a free flow of current information
2-Require open, timely, accurate and consistent information from our countries medical facilities
3-Take a blood sample (or tricorder scan) of everyone leaving or entering the country
4-Update medical regulations to accelerate innovation
Alan: Thanks for the idea, but given the local, state, and federal governments here in the U.S. previously failing to operate efficiently, I don’t think a technocratic solution is likely here. Some individual states can do at least some of the stuff that you suggest, e.g., https://philip.greenspun.com/blog/2020/04/04/florida-the-data-smart-state-when-it-comes-to-reporting-hospital-bed-availability/
It took years for the U.S. government to set up a single ecommerce web site (healthcare.gov). States that set up their own, such as Massachusetts, didn’t do them much faster.
Even the world’s smartest and most efficiently governed nations haven’t really beaten the coronavirus, I don’t think, just as these nations have not beaten the flu. In some cases they’ve delayed infections. In some cases, they have great-looking numbers possibly because they’re in the Southern Hemisphere and it was mid-summer when the virus hit (flu doesn’t spread well in the summer either).
I’m trying to come up with a good aviation analogy for our dramatic action. A big part of aviation is acting rationally even when you’re scared. Coronashutdown is perhaps analogous to flying along in a Cessna with an engine that is running rough and you think it might fail, thus subjecting you to a 0.15% risk of death. Instead of trying to land on the nearest runway, you say “I will nurse this aircraft along until I can get to KATL and then will try a landing on the ramp so that I can destroy 15 Boeings and Airbuses in a huge fireball as I finally set this thing down.”
Phil –
Why do you think modern governments (even pathetic ones like the U.S.) can run a pretty well-functioning aviation system while being so bad at public health (again, the U.S. is an outlier, but even the much-vaunted European countries that your neighbors wish they could live in have not covered themselves with glory.) Is it just because failures in aviation tend to be immediate and spectacular?
jimbo: That is a good question. First of all, innovation and change in aviation is glacial. The most recent big changes were the jet engine, a British innovation from 1937, and Gee radio navigation from circa 1940 (also British; see https://en.wikipedia.org/wiki/Gee_(navigation) ). Second, cost is no object. The typical aircraft being separated by ATC costs $30-300 million (i.e., airliners). There are only about 44,000 flights per day handled by ATC: https://www.faa.gov/air_traffic/by_the_numbers/
The U.S. health care system actually does work pretty well on the same terms. If you model it as as a system for providing expensive intensive care for a handful of extremely sick individuals, it does what it was designed to do. Now people are saying we will use this system to provide supplemental oxygen to tens of thousands of people with simple Covid-19 infections (“simple” because there is no medical cure).
What we need to do, and it’s not clear that we have the will to do it, is have a health care system with detailed electronic records that every person in the United States can carry with them. We need uniform standards and that data should belong to every person, so wherever they go for care, they plug their health dongle into the hospital’s system and it immediately lists their preexisting conditions and health records.
Unfortunately the first thing that comes to my mind for this is the potential for widespread hacking and targeted attacks against health care computers by people who make ransomware dongles and use them to try to infect healthcare networks. We’ll have to have secure ways to connect people’s data to the system without exposing the rest of the provider’s network. That could probably be done but it’s not going to be easy.
But having that data and a standardized way of accessing it and querying it for every patient in the country would have been an enormous advantage in this pandemic. We would know with much greater specificity exactly who is dying from COVID-19 and why, everywhere in the country. We could answer questions like:
“How many people in Oshkosh, Wisconsin are over the age of 60 and have preexisting health conditions who have not yet been tested, diagnosed or hospitalized?”
There are big, big questions here regarding the ownership and stewardship of that data. Already we have serious issues regarding the ownership of the DNA that’s being collected to test people. Who owns your DNA once you’ve submitted a sample for testing?
Personally, I don’t think anywhere near “most of us” would be dead. I agree with Michael Osterholm that the virus is going to continue to infect people until 60 or 70 or more percent of the population has been infected. Without a vaccine, the people who are most vulnerable are going to die — the aged and those with preexisting health conditions — unless we find something really effective like the HIV cocktail of antiretrovirals that increase their survivability. And I think that’s going to happen whether we open the economy tomorrow or 18 months from now.
https://www.cidrap.umn.edu/osterholm-quotes
Alex: The U.S. has a multi-decade track record of failure with electronic health records. Everything that you’re proposing was proposed in the mid-1990s if not earlier. The Obama Administration put tens of billions of dollars into the hands of hospitals (which turned around and gave it all to Epic!). I don’t see how it is reasonable to say “We’ll fix this urgent problem by doing something that we’ve failed to do, despite wanting to, for the last 25 years.”
@Philg: I know. I’m being unreasonably optimistic and impossibly naive.
I’ve read your dismal assessment in connection with your health care record system proposal from long ago.
Look at what we’ve done instead: Facebook, Google, et. al. can keep intimate tabs on me, all my friends, family and contacts, everything I’m interested in doing, everything I buy, everywhere I’ve been, what I ate for breakfast, every photo I’ve ever uploaded is recognized and all the people identified, they can suggest people to me that I haven’t heard from in 30 years, and can watch my behavior on hundreds of millions of websites across the globe and feed me ads because I’m thinking of buying a new John Deere riding mower with blinking headlights, but we can’t build a health care record system that works, no matter how much money we throw at it.
Are we happier now? Are we healthier? Are we any better able to deal with a pandemic? Hell, no! But we know in detail when every one of our friends has a birthday.
And of course, we want 5G so we can know how many times we’ve flushed the toilet, how many cups of coffee we’re brewing, how many eggs are left in the refrigerator, how many revolutions each tire on our autonomous vehicles have turned, and any number of endless IoT miracles that will revolutionize our lives and surely put us on the path to sustainable Nirvana. But good electronic health care records cannot be done. What a world we live in!
And as a result, we must absolutely destroy our economy and wipe out every single gain we’ve been able to achieve over the past half century while we wage war against ourselves in the name of stopping the spread of this virus.
Every so often, Peggy Noonan catches hold of something essential and writes about it in an op-ed. Her latest one is worth reading:
https://peggynoonan.com/scenes-from-the-class-struggle-in-lockdown/
“There is a class divide between those who are hard-line on lockdowns and those who are pushing back. We see the professionals on one side—those James Burnham called the managerial elite, and Michael Lind, in “The New Class War,” calls “the overclass”—and regular people on the other. The overclass are highly educated and exert outsize influence as managers and leaders of important institutions—hospitals, companies, statehouses. The normal people aren’t connected through professional or social lines to power structures, and they have regular jobs—service worker, small-business owner.”