I met with a cardiologist friend last night. He says that he is working roughly 60 percent as much as he was pre-coronapanic. “Where we would do five procedures per day, we can now do only two,” he said. “That leaves enough time for deep cleaning between patients. Also, they’re reserving 20 percent of the rooms in the hospital for Covid patients, just in case.”
He and his colleagues have already had multiple patients die while waiting for heart valve procedures that were considered “elective”. (see “StayHomeSaveLives or #StayHomeTradeLives?” and the link to the NEJM article) He gets paid in full despite the reduction in work and billing, and is at a vulnerable age for Covid-19 (70s), but is nonetheless anti-shutdown: “It was only a few years ago when parents were supposed to make sacrifices for their children. Now it is the other way around.”
Today is #ShutDownSTEM day. Plenty of righteous posts on Facebook from friends who are professors of various flavors of nerdism. They’ve been sitting on their butts for three months now, taking baby steps in the direction of online teaching (nowhere near as competently as faculty at Western Governor’s University, which has been online since the mid-1990s). Today they will sit on their butts even more firmly? It has been a struggle for me to refrain from asking “How could you possibly do less than you’ve been doing since mid-March?”
(Not all professionals are idle. A friend Facebook messaged me today about some divorce litigators who are fully engaged on an issue of life insurance. The defendant father wants to have the beneficiaries of his life insurance be a trust for the children (tweens). The plaintiff mother wants to ensure that the life insurance cash is paid to her, to compensate her for any reduction in profits from alimony and child support. The parties are divorced, but the litigation lives on (legal fees on both sides paid for by the father’s earnings that would have been the children’s inheritance).)
Speaking for myself, I participated in a Zoom meeting regarding some health records data analysis today, but all of the coding was in SQL so I am not sure if that qualifies as “STEM”! Later today it will be time to fly the helicopter, which can be considered a “STEM” activity by American journalists when a member of an officially recognized victim group is at the controls. One of the participants in the call is a third-year medical student. He won’t be able to do a clinical rotation until about a month from now (i.e., he will miss at least three months of clinical training).
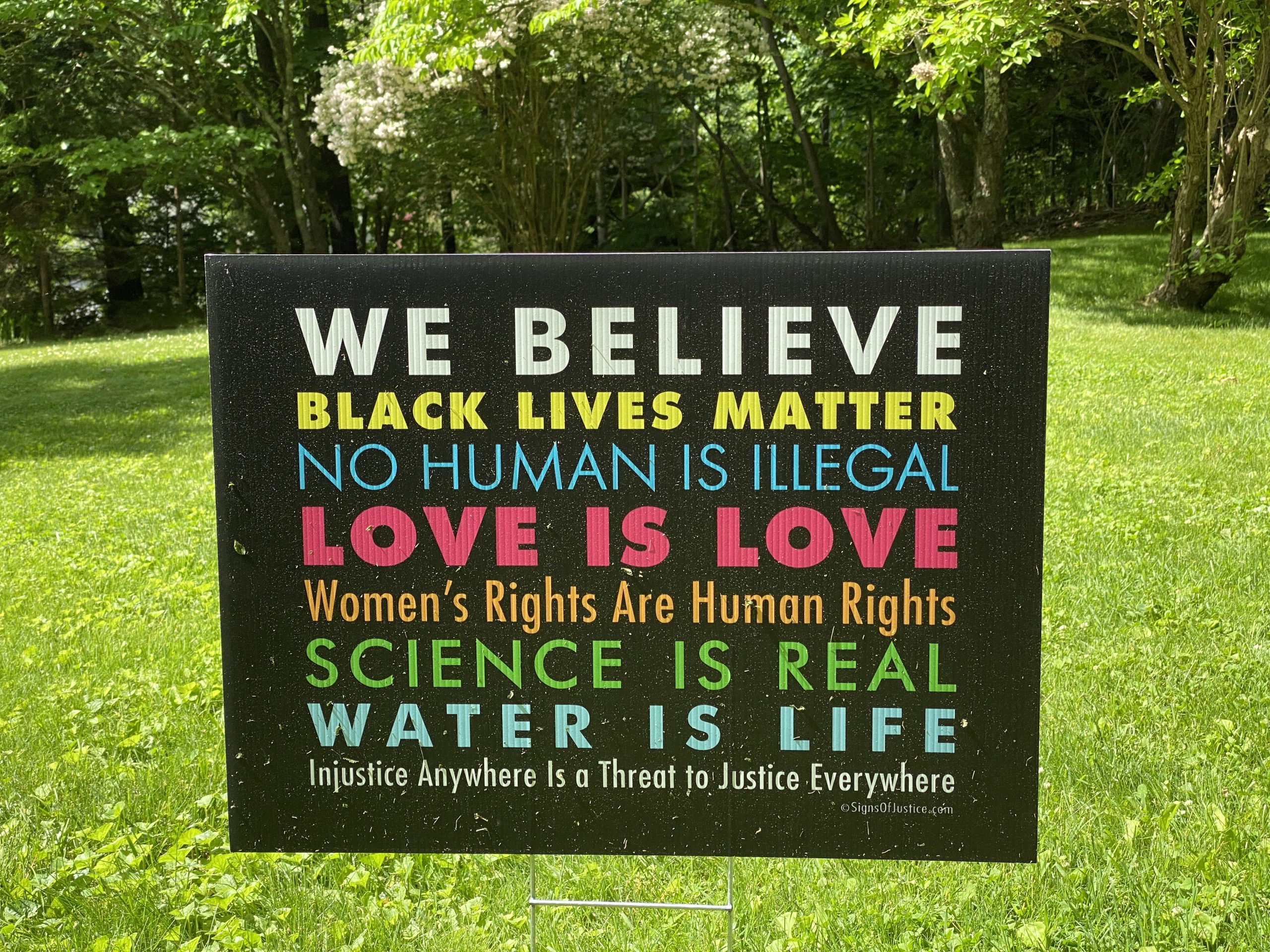
From a neighbor’s front yard, “Science is Real” (but also not so important that you’d want to do it every day?):
From a recent visit to the doctor’s office in Concord, Massachusetts to get some blood drawn in advance of a regular checkup:

(any of 50+ gender IDs is okay, but we will depict, recognize, and give priority to only two?)
Check out the guidelines for school reopenings in MA: Class sizes of no more than 12 people, everyone in PPE, 6 foot spacing between students, etc., etc. Impossible to do without significantly decreasing classroom hours and/or adding a lot more teachers.
“While students would be expected to bring their own face coverings to school, school systems would be required to purchase one mask per student per week as a backup. To avoid supply chain backups, schools are expected to have a 12-week supply of disposable masks on hand when schools reopen.
They also need 10 gowns, 10 pairs of gloves, two sets of eye protection, two face shields and 10 N-95 ventilating masks ***per staff member per week***. A school would need a gallon of hand sanitizer each week for every classroom”
https://patch.com/massachusetts/medford/s/h5241/back-to-school-plans-take-shape-in-massachusetts
If you look at the guidelines (and there are a lot more) you realize that when schools eventually do start to reopen, they’re going to need hundreds of millions (maybe in the billions) of dollars to buy all the PPE, hire all the new teachers, hire support staff to maintain the inventories of PPE and keep each classroom, teacher and student stocked up, and by the time they get through implementing the guidelines each day, what time or energy will they have to teach anyone? Then if one kid gets sick, what do they do? Shut down the entire school and spend how much money on a Class V Cleanroom CDC approved deep disinfection.
It’s a madhouse. They’re better off keeping the schools closed and letting the teachers continue to do next to nothing from home.
@Alex, take a deep breath and relax. It is possible. Norway did a very similar thing when the schools reopened, and the world didn’t explode. Classes were shortened, and that means each class “lost” a few kids to other classes. Instead of sitting together two per desk, then each kid had one desk. There are teachers for several subjects, these changes just meant teachers had to spend more time teaching than on other duties. The length of the school day was shortened so there would be no shortage of rooms. Also, when at school kids spend more time outdoors. Some tasks were kept online, e.g. some group work, or other individual assignments. There were no gowns/gloves/masks or other barrier protection, just hand sanitiser and more spacing. (The sanitiser did not run out, most kids in fact washed their hands instead — took a while but was doable.) Besides splitting the classes, each class was also sub-divided in smaller groups, with kids usually only interacting with others in the small groups. This was to help in case one kid got sick, there was only need to quarantine the kids in the small group.
Overall, it worked. Now it has been further relaxed and it’s basically back to normal. From the perspective of parents, even the “reduced school” was very much as the normal school. YMMV.
Jarle: Thanks for the on-the-ground info. As I pointed out in a response to a comment on another post (https://philip.greenspun.com/blog/2020/06/08/u-s-should-approve-a-saline-injection-as-a-covid-19-vaccine/ ), the U.S. always seems to swing to extremes compared to Europe. So if school ever does restart here in Massachusetts I wouldn’t be surprised by drastic measures.
———– my comment on the other thread
The U.S. tends to be one of the worst-governed wealthy countries due to a generally hysterical population. So we overreact to almost everything. Are there some poor people in our neighborhood? We are so upset by this that we make welfare more lucrative than work at the median wage (https://www.cato.org/sites/cato.org/files/pubs/pdf/the_work_versus_welfare_trade-off_2013_wp.pdf ). Is there a single parent struggling to afford a comfortable house? We’ll make having sex with a dermatologist more lucrative than going to medical school and working as a primary care doctor (works best in Massachusetts and California! http://www.realworlddivorce.com/ChildSupportLitigationWithoutMarriage ). Did we hear someone say something unkind about people with certain characteristics? Let’s roll those characteristics into a new victimhood group and give them preferences in college admissions, hiring, etc. There are some dangerous neighborhoods in a city? Equip the police with enough tanks and machine guns that they could fight off an attack by a small country’s actual army.
Medical errors are thought to kill ~250,000 American per year (some sources claim 400,000):
https://www.hopkinsmedicine.org/news/media/releases/study_suggests_medical_errors_now_third_leading_cause_of_death_in_the_us
So it’s not clear that postponing/canceling elective procedures is actually killing people rather than saving them. Even if you think the above number sounds too high, there’s ample evidence that when elective procedures are canceled because healthcare workers go on strike, mortality either stays the same or goes down:
https://pubmed.ncbi.nlm.nih.gov/18849101/
Medical deaths: that all began with the Makary/Johns Hopkins paper, which was so widely disseminated and quoted that it took on a life of its own, despite having serious flaws methodologically and by the most basic test of common sense. The numbers are are **hotly** disputed. The claim of ~250,000-400,000 deaths per year would make medical errors responsible for more than half of the hospital deaths in the United States. The lawyers who push medical malpractice litigation love the big numbers. > 700 deaths a day! Nobody should *ever* go to a hospital without a lawyer at their side, for God’s sake!
https://sciencebasedmedicine.org/are-medical-errors-really-the-third-most-common-cause-of-death-in-the-u-s-2019-edition/
https://www.medscape.com/viewarticle/917696
https://www.sidgilreath.com/learn/medical-malpractice-death-statistics.html
One way we can assess how frequent various causes of death are is to look at how many celebrities die of them. A number of high-profile celebrities are thought to have been killed by malpractice. Neil Armstrong died after complications from coronary artery bypass surgery. Michael Jackson famously died of an overdose from drugs provided by his personal physician (several other celebrity deaths fall into this pattern except the drugs were self-administered, e.g. Marilyn Monroe, Elvis, Prince, and Anna Nicole Smith). Joan Rivers died from complications of a throat surgery. Andy Warhol was killed by a botched gallbladder operation.
The reason medical malpractice is so common is that, unlike in aviation, where every time a serious incident occurs, a postmortem is performed to come up with recommendations to prevent it from ever happening again and/or mitigate the consequences if it does (although something seems to have gone wrong here in the case of the 737 MAX, which crashed *twice*), doctors cover up their mistakes to avoid being sued. Surgeons routinely do things like operating on the wrong patient, performing the wrong procedure, and amputating the wrong limb (these are termed “never events,” despite the fact they occur quite frequently).
Ryan –
“Surgeons routinely do things like operating on the wrong patient, performing the wrong procedure, and amputating the wrong limb”
It’s too bad I wasn’t trained in or even given the opportunity to passively witness any of these routine malicious procedures during my surgery internship.
I have to admit — I’m getting tired of all the debates about these things. Everyone has an agenda with research numbers and advocacy, all contradictory and at each other’s throats. Today I was listening to NPR and they were supposed to be focusing on renewable energy. The debate wound up ranging over everything from Black Lives Matter, diversity, the number of women on the boards and as CEOs of public companies. Then it devolved into even more nonsense: one commentator basically opined that renewable “smart grids” were worth any price we had to pay for them because they were “better technology.” So if the cost was 25%, or 50%, or 200% higher for electricity, it didn’t matter because the technology was better. So if you’re already paying exorbitantly high rates for electricity because nobody will build more central power station capacity for our electric grid, businesses and everyone else just need to dismiss their cost concerns and smile. No evidence presented, no numbers, no objective comparisons, it’s all just blind-faith hocus pocus and propaganda.
I think it all has to fall apart, and it will.
If you neighbors believe No Human is Illegal and Love is Love, you should pitch a tent on their nice lawn, bring a few friends, and tell them you’re camping out in their yard until you find a permanent home. They’re not using it for anything except the sign. Tell them you’re going to crap in their back yard and you’ll need some water from their hose for cooking and bathing. A couple of towels would be nice, and ask them if they can spare some food. Tell them your business failed, you lost your house, and you don’t want to live in a homeless shelter. Better yet, recruit some actual homeless people who are non-illegal migrant humans, pitch the tent, tell them you have a nice yard for them to stay in, and see how long your neighbors go for it.
Follow up report on my recent hospital visits: after two trips to the hospital for blood draws and a CT scan wherein I was practically the only patient on the premises, today I had an cystoscopy done as an outpatient procedure at my urologist’s small practice. I had to wait outside in the blazing sun and humidity, because the door was locked and they were admitting only one patient at a time, so I sat in my mask in a lawn chair on the front porch for 15 minutes until the receptionist unbolted the door, cracked it open two inches and started with the questions:
“In the past two weeks have you come in contact with anyone who was diagnosed or has symptoms of COVID-19? Do you have a fever, shortness of breath, any respiratory problems….” etc., etc. I answered in the negative and was admitted into the office, where I sat at the opposite corner of the waiting room from another patient who had arrived about 15 minutes before I did. He was still filling out the 8 pages of forms with a ballpoint pen, trying to balance the clipboard on his knee with his glasses falling off his face, wearing a mask that kept drooping. Meanwhile the wall-mounted jumbotron was running a loop about social distancing with Dr. Birx and the Surgeon General punctuated by travel suggestions for Australia and a story of some goofball people entertaining their neighbors during COVID-19 by parading through their neighborhood wearing dinosaur costumes. It was all very surreal.
The results weren’t conclusive enough. At least the doctor was thorough and I felt every second of it. Now he wants to do another, more invasive look using a hospital operating room which will require me to be anesthetized while they probe around with the larger catheter/endoscope. I asked him how long it would take to schedule: “I’m going to check that this afternoon and do my best to get you in within a month and a half. We’re just opening back up for the hospital procedures.” So this whole thing is now extending past three months from initial contact, which will be four to four and a half before I have a conclusive diagnosis. Normally this would have been something that was handled in less than a month from end to end.
And I am passing blood, but have no apparent infections. The cytology results on my urine didn’t show any signs of cancerous cells, at least, but something is clearly wrong and I’m waiting like everyone else for these “elective” procedures to move forward.
The kicker: On the way back home I stopped at the local McDonald’s for some unhealthy food, which I felt I deserved (or at least, I didn’t want to think about making anything healthy for myself this evening) to soothe the pain from the still-throbbing urethral spelunkering I had just endured. I drove up and placed the order.
I was still tuned into NPR. The topic was now the pressing need for people who have had strokes to immediately seek medical care, the faster the better. “With some types of strokes, millions of neurons are dying every second, so you reduce the damage enormously the faster you get care.” Of course, this is true for many other things as well. I glanced at the time/date display on the infotainment console instantly calculated how long this diagnosis had taken so far, while the ” : ” on the time display blinked. Good thing I had put it in Park. I zoned out.
“Sir…? Sir…? That’ll be $11.43 please..Sir?”
I realized I’d been completely lost in miasma of brain fog for about 30 seconds and didn’t even see the young girl at the window asking me for my money. I turned to get a good look at her. She was perhaps 17 years old, maybe 18, but the older I get the tougher it is to accurately gauge. She was beautiful. Long brown hair done up in a neat bun; long, slender fingers with pretty nails, and big, gorgeous brown eyes, fireworks for a smile and just-a-teeny-bit crooked front teeth. She had never had braces, but basically didn’t need them. Petite. My kind of girl, 30 years ago. I was in a time warp.
“I’m so sorry, jeez…hang on just one sec, OK?”
“Oh, it’s NO PROBLEM at all! Take your time.”
“Thank you. I keep finding out what it’s like to be a million years old.. Today’s a million years and one day.”
She laughed. She’s handling it all pretty well. Bless her, and thanks for her.
Your neighbor’s sign forced me to catalogue my own beliefs. It goes something like this:
Worship no false idols
Do not take the Lord’s name in vain.
Honour the Sabbath and keep it holy.
Do not bear false witness.
Do not commit adultery.
Honour thy mother and father.
Do not murder.
Do not steal.
Do not covet thy neighbor’s wife.
Do not covet thy neighbor’s goods.
This list used to be taught in schools and churches and synagogues, but now the schools and churches and synagogues are more interested in your neighbor’s point of view.
George Carlin managed to shorten the list:
https://youtu.be/CE8ooMBIyC8
They’re pretty tough to beat. There are a lot of other belief systems that purport to do better with much more complicated metaphysics, but they really don’t work very well.
> He and his colleagues have already had multiple
> patients die while waiting for heart valve procedures
> that were considered “elective”.
The benefits of lockdown are only just getting under way. Here is an interesting contrast between two analyses, one mainstream (based on models) and one not (based on history).
Mainstream: Virus deaths ‘could have been halved if UK entered lockdown week earlier’ from the famous Neil Ferguson. His demonstration that lockdown did not apply to himself hasn’t diminished his authority with the media. He remains a member of the SPI-M committee advising the British government. Costs and disadvantages of lockdown are not mentioned in the article.
Not mainstream: Remember how public health COLLAPSED after Soviet Union fell? from British doctor Malcolm Kendrick. The article examines the increases in death rates in the post-Soviet period of economic turmoil, turmoil of the kind we are just beginning. It describes the resulting poverty and stress as the biggest killer of the 20th century after famine and war.
@LP: An interesting paper from 1996 providing historical context on the Soviet healthcare system, its origins, development, collapse and attempts at “resuscitation” as of 1996.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1380507/pdf/amjph00514-0021.pdf
“In the years that preceded the collapse of
the USSR, the Soviet Union was the only
major country where the percentage of
the gross national product going to health
care decreased. Although the Soviet Union
boasted more physicians and hospital
beds (both absolutely and per capita) than
any other country, Chazov often found
their quality to be abysmal, well below
world standards. Corruption, including
bribery in the admission and graduation
of physicians (a shocking proportion of
whom could not perform the simplest
medical procedures), had permeated the
entire system. Largely as a result of the
very low salaries they drew, some health
personnel demanded large sums of money
from patients to provide services they
were supposed to provide for free. A
shortage of pharmaceuticals and other
medical supplies intensified, leading often
to gray or black markets. And on top of all
this, the system was paralyzed by a
suffocating bureaucracy and a command
mentality.8” …
“In the final years
of the Soviet Union, national health care
budgets were in the range of 3% to 4% or
even less (accurate figures were never
available) of gross domestic product
(GDP).28 Of this amount, as much as half
went to finance the “fourth department”
of the Health Ministry that provided care
exclusively to political elites, who accounted for less than 1% of the population.”
And then it got worse! Kendrick is right to point out that the economic and political collapse of the Soviet Union precipitated a grave health care crisis from which Russia and other states have yet to fully emerge. Inflicting one on ourselves is going to do much the same thing here, even though we started with a much more functional system.
The “Love is Love” motto from those on the left is interesting.
Since they are also the same people who deny the “love” than can exist between a 65 year old man married to multiple 18 year old brides, who wish to consensually enter into such polygamous relationships. The left are opposed to that sort of love since it appears to be “religious” and involves women supposedly being “exploited” by men.
Of course a 65 year old man with multiple 16 year old boys would be fine – since we are not allowed to be homophobic.
I just read the post-divorce litigation chapter from RWD http://www.realworlddivorce.com/PostDivorceLitigation I think the state should just give the guys who keep getting shipped to jail and/or are crushingly indebted for life the option of physician-assisted suicide. Since men actually do kill themselves about 3.5 times more often than women and with the plight lot of these men best described as “utterly hopeless” I’m surprised there aren’t more detailed public health studies examining the correlation between suicide and post-divorce litigation and incarceration. Hundreds of thousands of these guys are doomed. I’m not surprised a lot of them kill themselves, and without “bonafide” research to put a number on it, it’s going to keep going.
https://afsp.org/suicide-statistics/
I can’t find any serious studies – all the reports are therefore anecdotal and personal – and nobody seems to care. Where’s Mike Bloomberg’s School of Public Health? They care about gun fatalities. But why are these men pulling the trigger on themselves?
In fact, if you go the the afsp.org link above, they have a search tool to look up suicide research by keyword, so I tried it out:
https://afsp.org/research-grants?query=Divorce
One very preliminary study, in 2012, and not focusing on divorce and post-divorce litigation, it’s much broader. That’s it.