The wicked Swedes who refused to lock themselves down, refused to pull their children from schools, refused to follow WHO advice (the latest advice, that is, not the June 4 advice) to wear masks, and refused to stop going to work will suffer 5,754 deaths from/with Covid-19 through October 1, 2020, according to the prophets at IHME:
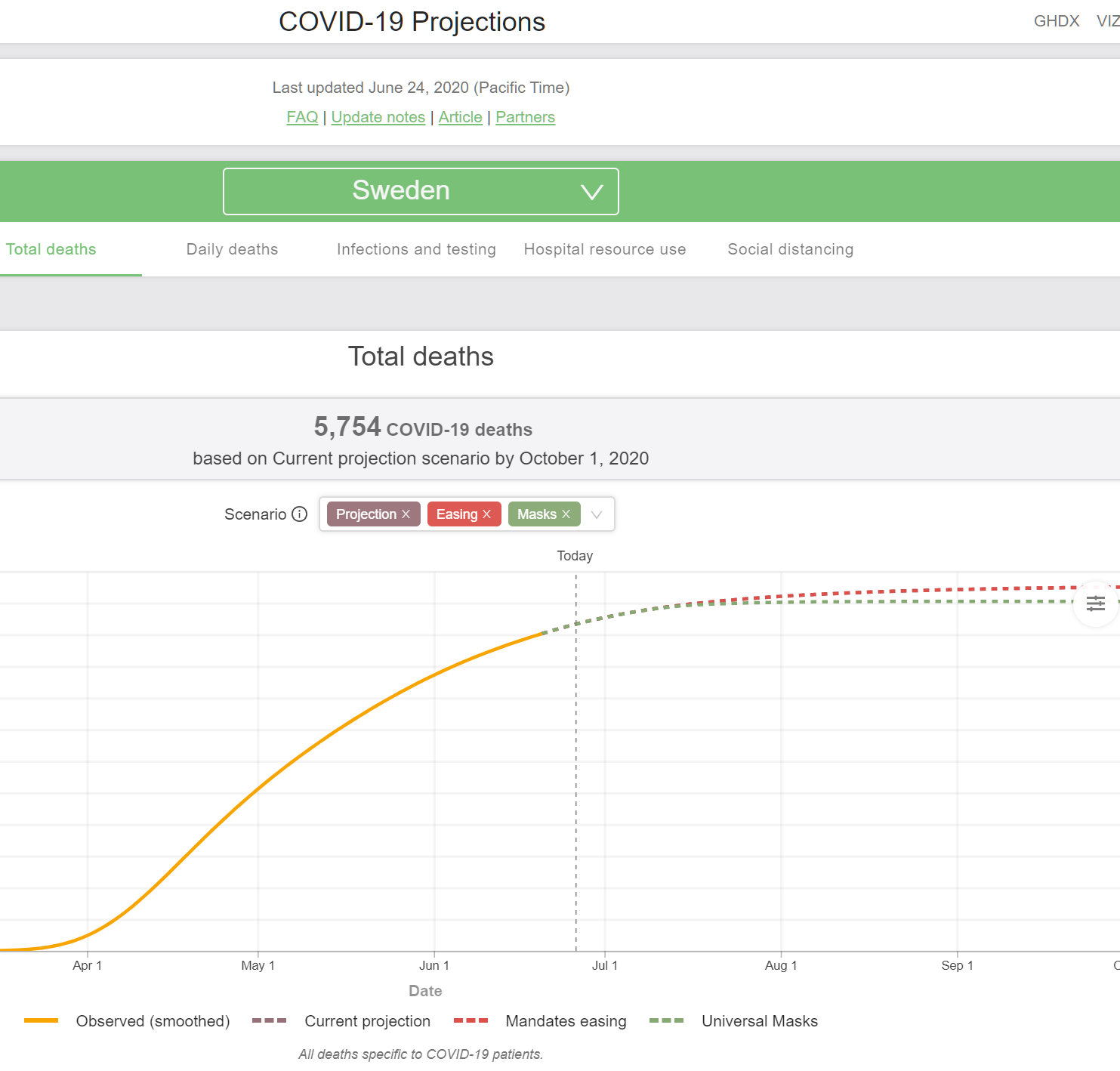
The infidels who refused to accept the true Church of Shutdown will lose 0.056 percent of their 2019 population of 10.23 million.
The latest (June 24) IMHE prophecy for the U.S. is that 179,106 residents will die from/with Covid-19 through October 1, 2020:
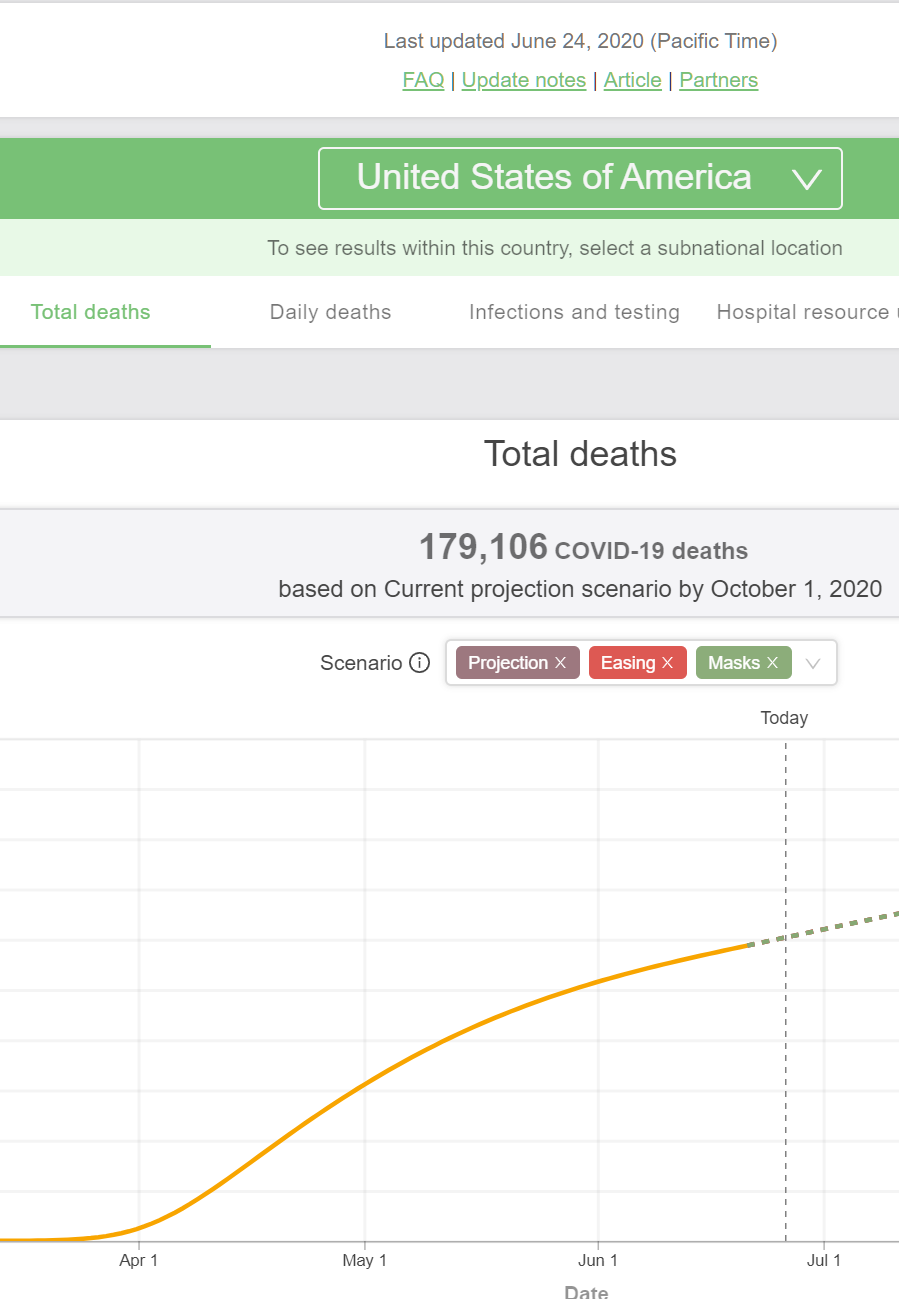
Compared to the 2019 U.S. population of 328.2 million, that’s a rate of 0.055 percent.
In other words, the U.S. and Sweden will have almost exactly the same death rate from coronaplague.
Yet for Americans believers in the Religion of Shutdown, Sweden remains the touchstone example of disastrous “experiment” and folly. (It is not an “experiment” to lock people into their apartments for three months in hopes of stopping a viral plague, nor to shut down K-12 schools nationwide for the first time in U.S. history. These are examples of wisdom and being “conservative”.)
An example from yesterday, by a Harvard Law School professor, “Is Digital Contact Tracing Over Before It Began?” (Medium, June 25):
The first scenario is roughly the same as Sweden’s approach: re-open all but the most high-spreading services and events; ask people to exercise social distancing where they can; have people wear cloth masks to minimize the spread of the moisture in their breath to others; and try to make available testing so that people who wish to know if they’re infected can find out and then self-isolate if they test positive or show worrisome symptoms. We might call this the YOLO scenario.
This approach risks lots of preventable misery, and death, should hospital capacity be exceeded, or the disease affect far more people than it would if we were able to mitigate spread before a vaccine or treatment is available. (The architect of Sweden’s YOLO plan has expressed some regrets over it, though the numbers appear to be attenuating at the moment.)
The author simply neglects to mention that the death rates in the U.S. and Sweden are on track to be within 3 percent of each other. For the American readers, this isn’t necessary because, to the extent that Americans die it will be because we are imperfect creatures. We try to follow the God of Shutdown, but sometimes we slip and need to ask forgiveness of Him/Her/Zir/Them.
(The article also shows the American faith that the God of Shutdown will protect the righteous and punish the wicked among us:
With the President resuming his campaign rallies, the line between partial re-opening and full re-opening may become quite blurred.
I.e., a Trump rally will spread coronaplague among the stupid/racist/sexist Deplorables, but the virtuous BLM protesters who gather in similar numbers will be protected by their faith.)
From across the river, a former Harvard Med School/School of Public Health professor writes “A Warning From Sweden’s Coronavirus Response” (Forbes, June 4):
Sweden now has among the highest per capita death rates from Covid-19 in the world. Why?
The answer is simple. Sweden was lax in its implementation of protective measures in the face of the outbreak, refusing to implement broad stay at home orders for residents, or to enforce recommendations to wear masks or social distancing measures.
Sweden’s story is a lesson for all of us around what happens when we pull back on social distancing and prudent epidemic control measures.
… one can’t help but wonder if perhaps the plan is to pin all hopes on a vaccine rather than use the public health tools we know can work to control the pandemic. If that is the case, we should be aware that our hope in a vaccine is far brighter than preliminary public data suggests it should be. The current generation of vaccines are likely to offer only partial protection, and likely only to some of us not all. With the new vaccines will come new risks, and unknown safety profiles.
The guy who looked at numbers for two decades at the School of Public Health can’t be bothered to compare the forecast death rates from Covid-19 for Sweden and the U.S., plus add to the U.S. numbers all of the deaths going forward from weight gain during lockdown, lack of exercise during lockdown, alcoholism and drug addiction acquired during lockdown, lack of education during lockdown, rioting as we emerged from lockdown, etc.
(He also sounds like an anti-vaxxer! “New risks” and “unknown safety profiles” from the rushed-to-market vaccines?!? So… if we aren’t going to have an effective or safe vaccine, doesn’t that make the Swedes ever smarter? Are we capable of staying shut down for 10 years?)
I still think that, 10 or 20 years from now when the U.S. has finally figured out how to deal with coronavirus (maybe just a psychological adjustment, as we’ve had to make for influenza, the common cold, and most other viruses), the most interesting writings on this period will be from scholars of comparative religion.
The comparative religion point is the right one. So here in NYC hundreds of people have set up a shanty town outside of City Hall advocating the abolishment of the police, certainly a religious idea based on the notion that human beings are born good but corrupted by the structures of society. https://nypost.com/2020/06/25/more-protestors-are-joining-the-occupation-city-hall-park/
Too bad none of these people ever bothered to read Hebrew scripture because if they did a few pages in they would have come upon the first human beings born of natural parents, Cain and Able with Cain murdering Able because Cain felt insulted and therefore envious, i.e., in the state of nature human beings are violent, vengeful and irrational. Not exactly John Lennon’s Imagine.
I did similar calculations using the model at covid19.projections.com (I know @Alex thinks this has some of the “better” modeling, and I have heard that from several friends – none or course are epidemiologists!) and the numbers are surprisingly close:
US death rate as of Oct 1, 2020 (projected): 0.058%
SW death rate as of Oct1, 2020 (projected): 0.062%
Of course, the US’s numbers may have been worse early on if the Church of the Shutdown was at least not partially obeyed (due to projected ICU/Hospital capacity being exceeded). And I assume the projected US death rate is slightly less than Sweden because the wicked Swedes are apostates of Mask’ology!
The main reason I cite Youyang Gu’s model is because in comparison with other major models, it has performed consistently well. ( https://covid19-projections.com/about/#historical-performance ) Hey, it could get worse, maybe he’s missed something, but he’s very attentive to the details.
I do enjoy the idea that a single, well-educated individual ( https://covid19-projections.com/about/#who-we-are ) writing his own code and not taking any money from outside organizations can produce a model that performs so well. You can run it on a laptop computer running Python and don’t need a cluster, a supercomputer, or a cloud account, so you could literally take the whole thing with you and teach a course with it.
He’s been working on it for less than three months and he’s standing tall against organizations like Los Alamos National Laboratory. That’s a tour de force for an individual during an era where we can’t seem to get good results out of huge organizations comprised of hundreds or thousands of people for millions of dollars. The fact that he’s not trained as an epidemiologist is icing on the cake, to me. More power to him.
@Alex – thanks. Agree, I like his attention to details. And fascinating about his background and his great thinking and programming skills. As you say, more power to him.
Wrong bogey. Comparing two failed approaches, Sweden and the US, isn’t going to yield much of interest.
Compare the US result to Japan, South Korea, or Taiwan.
They are crushing it. We are failing.
@G C — Excellent point (and New Zealand?). Of course all smaller island nations (not S Korea, but only one land border and not much travel there). They also have histories with epidemics and lots of mask wearing. It will be interesting to see if other non-isolated large countries do much better over the long haul, and what we learn.
China (a large, not island country) is kicking our asses right now. While American thought leaders were telling people to go out and protest (whether or not the protests were for a good cause, and whether or not they actually were a significant source of viral transmission, this definitely convinced a bunch of people that social distancing rules were bullshit and it was now OK to start absolutely ignoring the problem), some of the smartest people in China were keeping the virus from hardly spreading at all in China. China is reporting about as many cases per day as our being reported out of one bar near my hometown:
https://www.wilx.com/content/news/COVID-19-cases-associated-with-Harpers-continues-to-climb-571503181.html
“China (a large, not island country) is kicking our asses right now.”
Ryan,
Assuming the Chinese corona numbers are correct, their approach can hardly be emulated by probably any Western country. The US, as one such example, has more individualistic culture with distrust of the government. If the government tried to introduce strong measures on par with what China did, it could have caused an equally strong reaction and worse outcomes than the rather mild measures that people might agree to (Stalin could have eradicated coronavirus in one day — just shoot the carriers on spot).
The practical inability to “crash the curve” rather than “flatten the curve” is the cost of having a non-conformist individualistic society with decentralized government vs. its opposite. Some additional measures like contact tracing may work in states like NY, MA, NJ, etc, but hardly in TX, AZ, or FL.
Also, some medical “experts” lost any shred of credibility by stating nonsense like crowds when rioting are good because of their cause but e.g. when going to the church they are bad, offering contradictory advise that masks do not help, and then masks all of a sudden do help, etc.
Other countries S. Korea, Japan, although more democratic than the ChiComs, have societies with a much higher degree of government and societal trust, collaboration and conformism than any Western democracy plus they have other favorable features already mentioned here (Hawaii has similar advantages). Lastly, I am not sure whether it would be practically possible to implement real border controls (as in China, Japan, S Korea) to prevent infected people entry via the southern border from South America even in the unlikely case this country did decide to implement stricter quarantine measures.
“Illegal immigration rose nearly 40% amid coronavirus reopenings”
https://www.washingtontimes.com/news/2020/jun/12/illegal-immigration-rose-nearly-40-amid-coronaviru/
Listen to the things Zittrain calls “well-considered plans”:
“Harvard’s Safra Center (“We need to massively scale-up testing, contact tracing, isolation, and quarantine — together with providing the resources to make these possible for all individuals”), the Center for American Progress (calling for “instantaneous contact tracing and isolation of individuals who were in close proximity to a positive case”)
Then he goes on to cite the AEI, etc.
What CAP’s plan really mean? It means you’re walking around with your phone, you get within 6 feet or 12 feet or 15 feet (whatever the GPS resolution is, I guess that’s about 15 feet) of someone who has tested positive or – someone talking with a contact tracer says they were near you and they tested positive. You get a call from the local Board of Health, enforced by a police officer, that says: “You can’t go to work tomorrow. If you’re at work now, go home. (If you’re in Massachusetts and work in a restaurant, the restaurant must also close for 24 hours and be deep-disinfected). You can’t leave your house. You can’t stay in the same area of your house with anyone else. Don’t get near your children. Stay right where you are. For two weeks or more.”
And he really wants all of this as a “centralized effort” run by the Federal government, with everyone in a database, being tracked, “instantaneously isolated” and monitored in real time. Private efforts by individual companies are inadequate because most people won’t receive the “benefits” of them.
They’re totalitarians. COVID-19 has exposed these people for what they really are. Zittrain https://hls.harvard.edu/faculty/directory/10992/Zittrain is a tenured professor at Harvard Law School and also teaches at Harvard Kennedy School of Government, etc., etc. His compensation has to be comparable to Elizabeth Warren’s, and she made $429,981 at Harvard from 2010-2011.
And I mention his compensation for two reasons. First of all, you can’t find it anywhere – Harvard doesn’t publish the numbers, but he’s an endowed chair and he teaches in several different places at Harvard, he’s one of the rockstars, so presumably he’s very well compensated. I don’t think he has the slightest idea of what it means for most people in this country who have already been locked down since late March or early April. His job and livelihood and future are secure. It would literally take a nuclear attack or a meteor strike to knock Jonathan Zittrain into anything like precariousness. And he doesn’t care what it costs – which is why he doesn’t even attempt to put a number on it. He wants that goddamn federal database, though, and the army of people needed to enforce it, at whatever cost it takes.
I really invite everyone to read the Center for American Progress’ “well-considered plan.” This was their totalitarian COVID manifesto as of April 3.
https://www.americanprogress.org/issues/healthcare/news/2020/04/03/482613/national-state-plan-end-coronavirus-crisis/
They want isolation of not just people who have tested positive for COVID-19, but also those who *have a fever*.
“Isolation of individuals who test positive for COVID-19, individuals who have a fever, and front-line health care workers”
They want all the data hosted by some “trusted” nonprofit entity, except that the data may be shared with the CDC (of course!) They talk about anonymizing the data, and at the same time they want “Public alerts and mapping to inform the general public of the location of COVID-19 cases.”
How do you anonymize a public map of the location of COVID-19 cases? You’re driving down the street with the map on your phone, the next house has a big red marker on it. That’s Jonathan Zittrain’s house! So you know right away: “The Zittrain family has at least one person who has tested positive.” Later that day you see Zittrain at Pappa Razzi in Wellesley. He’s sitting at a table with a few friends eating Fusilli Affumicatti. You saunter over to the table: “Professor Zittrain, I was just reading your article in Medium and I noticed that your house is marked on the public COVID-19 infection map. Does the management of this establishment know?” You call the manager over: “Look, it says right here. Guess you have to close this restaurant down for 24 hours. And everybody has to go into quarantine. Including me.”
Harvard Law School seems to promote contempt for basic individual rights with amazingly weak public order / public health justification. Scary.
Philg, our goal was not to prevent deaths, because eventually everyone will die, nor to prevent infections, because eventually everyone will be infected, but to protect our inadequate health care system by “flattening the curve”. To the naked eye it seems we have done this – our curve looks flatter.
Alan: I remember being sold on “flatten the curve” back in March! But just a few weeks later people seemed to be assuming that lockdown would “prevent” infections and deaths. And I think we’re still on that dogma. If Americans are sufficiently locked down and masked up, nobody need die from/with Covid-19.
Where does this idea that “eventually everyone will be infected” come from? Imagine you were managing an Ebola outbreak with the attitude that “eventually everyone will contract Ebola” and you were powerless to do anything except control the rate at which it happens. Makes zero sense, right?
“Flattening the curve” while allowing everyone to get infected turned out to obviously not be the best idea, looking at other countries. It essentially requires targeting an R number of just about 1 to ensure a constant rate of spread through the entire population. At that point, why not try just a little bit harder to get it below 1 and effectively suppress transmission altogether? It’s very puzzling and disheartening to me that the US continues to refuse to try to emulate the success of other nations and instead continues with mass human sacrifice for no apparent reason.
@Ryan:
It’s not much of an outside idea. It’s just not publicized very much right now. On March 21, Judith Persichilli, who is the state Health Commissioner for New Jersey leading their coronavirus response said: ““I’m definitely going to get it. We all are,” Persichilli says matter-of-factly. “I’m just waiting.”
The idea that the virus was de facto uncontainable and would eventually spread to everyone was not a fantastic concept or an outlying opinion. They just stopped talking about it that way in their efforts to slow the spread down, because it was detrimental to their efforts to close the state down, lock down people and businesses and enforce social distancing. They couldn’t keep saying: “Everyone is going to get it, but we’re closing everything down anyway and forcing our economy to take a catastrophic hit, regardless of that fact, to prevent our hospitals from being overrun.” And the unstated: “And make sure we protect the vulnerable. The rich people.”
But that’s what they did.
https://www.nj.com/coronavirus/2020/03/im-going-to-get-it-we-all-are-njs-top-health-official-says-as-she-leads-the-states-coronavirus-war.html
“eventually everyone will be infected”: that misses the point that a significant share of the population seems to be immune to being infected.
U.S.-based organization that has most impressively addressed COVID-19 indicates a US infection rate of 5%
https://covid19-projections.com/
No way is that consistent with exponential spread across five months.
Ryan – There are some fundamental differences in transmissibility between Covid-19 and Ebola, so I would not say that about Ebola.
The “everyone” for infection is not the hard 100% that death is, but our expectation for most viral infections is that everyone will get it eventually – we ask people to get a flu vaccine every year, we ask people to take special care every cold and flu season.
Ryan – “success of other nations” at this point is just unfounded bias on your part.
Mic – The impact on each person is different – those who get a vaccine, if one becomes available, are technically infected just enough to build anti-bodies, many people who are infected have minimal or no impact on their health.
Aren’t you failing to consider that the socialist Swedes are not only happier, but considerably healthier than us free-marketeers in the USA? What’s the prevalence of the comorbidities for COVID, such as diabetes, obesity, etc, among Swedes compared to Americans?
This link, for example, says American obesity is 3x:
https://www.nationmaster.com/country-info/compare/Sweden/United-States/Health
Once again I feel like I’m in a parallel universe, one where the US is experiencing a worrying surge in new cases in the south and west. https://www.wsj.com/articles/coronavirus-surge-in-south-and-west-looks-different-from-norths-11593203105 https://twitter.com/JedKolko/status/1276490565543067649?s=20
An increase in new cases was expected due to relaxing containment measures: the infected people did not just vanish. Probably, there is a combined effect of new cases and more comprehensive testing which I believe doubled the number of administered tests e.g. in Florida only during last several days.
To what degree the surge in the number of newly discovered cases will translate in the number of deaths remains to be seen in a couple of weeks. Apparently, the median age of new cases in FL is 34 years and in Texas 38. If the new cases are skewed now towards younger population, the hope is that the death ratio will be much smaller than if the situation was similar to that in NYC, assuming that the distribution of the mortality rate by age is still similar to what it was discovered to be a while ago.
Not sure what is so “parallel” in comparison to Canada today. The mortality rate in the three southern states is still below that of Canada, but as I said the picture will become much clearer later. Perhaps, it’ll be as apocalyptic as it was in NYC, perhaps not.
You’re missing the elephant in the room. If we didn’t shutdown we’d most likely have a far higher death rate than your beloved Sweden.
As I noted in https://philip.greenspun.com/blog/2020/05/01/is-the-face-mask-the-church-of-shutdowns-hijab/ : “classic begging the question: I know that shutdown works to save lives because look how many lives shutdown has saved in NYC.”
So you look at the U.S. in Month 4 of shutdown, on track to have exactly the same death rate as never-shut Sweden, and say “This proves that shutdown works because consider how many additional lives we would have lost if we had not shut down for four months and counting…”
Jim: If you’re willing to beg the question, any government policy can be justified. A governor could say, “I’m locking down this state for the next five years, with the exception of approved trips out of the house for businesses that I deem essential. Elections are suspended during this five-year emergency.” Then, at the end, say as you do “Look at the large number of coronavirus and influenza deaths. It would be been far higher if we hadn’t had the five-year lockdown.”
Phil: “Begging the question” is irrelevant. If we had carried on as Sweden, our young people would have stayed in school, visited bars, and attended large parties. They would have likely gone on to spread the virus to those most vulnerable. This is not “begging the question”. This is simple deductive reasoning based on our far lager population.
You’re seeing it happening now with most states reporting record spikes. It seems logical that record deaths will follow. To claim that the US and Sweden have the same death rate, they have to be measured under the same conditions…not one under lock down and one open.
Begging the question: “When did you stop beating your wife?”
Jim: Isn’t your theory at odds with the “flatten the curve” dogma? The Magic of Shutdown was to delay infections, not prevent infections. So… yes, we closed universities for our young people. Now they will get coronavirus somewhere other than university, maybe a few weeks after they would have gotten coronavirus at their university.
Evidence for the Flatten the Curve dogma being true is that we are forecast to converge to having almost exactly the same death rate as a country that didn’t bother to do much of anything (i.e., Sweden).
Jim (and others): From today’s NYT… “After Asking Americans to Sacrifice in Shutdown, Leaders Failed to Control Virus”. https://www.nytimes.com/2020/06/27/us/after-asking-americans-to-sacrifice-in-shutdown-leaders-failed-to-control-virus.html
In other words, it is an established fact that a human “leader” can control a virus. (If so, why not have the Great Father in Washington #EndInfluenza ? )
Extension statistics and background detail on the situation in Sweden here:
https://www.nicholaslewis.org/the-progress-of-the-covid-19-epidemic-in-sweden-an-analysis/
He claims an incredible 10x reduction in IFR over time from 0.6% to 0.06% in Sweden. Too good to be true ? Time will tell…
Ivan: Why wouldn’t we expect a large reduction in IFR for a flu-like disease? The people who are easiest for the virus to kill will die first, won’t they? And, if there is some sort of way to identify easy targets for the virus (e.g., advanced age or poor health), a society will naturally respond by isolating that vulnerable group. I haven’t read the article carefully yet, but “10x reduction in IFR” doesn’t necessarily mean for a risk-adjusted group, does it? So if the virus first hits a nursing home and then an adult soccer camp we could easily see a more than 10x reduction!
He claims IFR reduction across all age groups, and specifically 10x for the 50-59/60-69 segments, less for older groups but still 10x overall. If true, that’s very good news.