I spent some time recently with two Harvard undergraduates who are camped out in a Cambridge apartment. I’m the oldest person that they’ll have any contact with for the foreseeable future, yet these 20-year-olds behave as though they either worked or lived in a nursing home for 90-year-olds. Asked why they put so much effort into mask-wearing and deny themselves so many social opportunities that they would previous have jumped at, they say that they are personally afraid of getting coronavirus. They’re not obese or chronically ill, so their statistical risk of being felled by Covid-19 is low (see
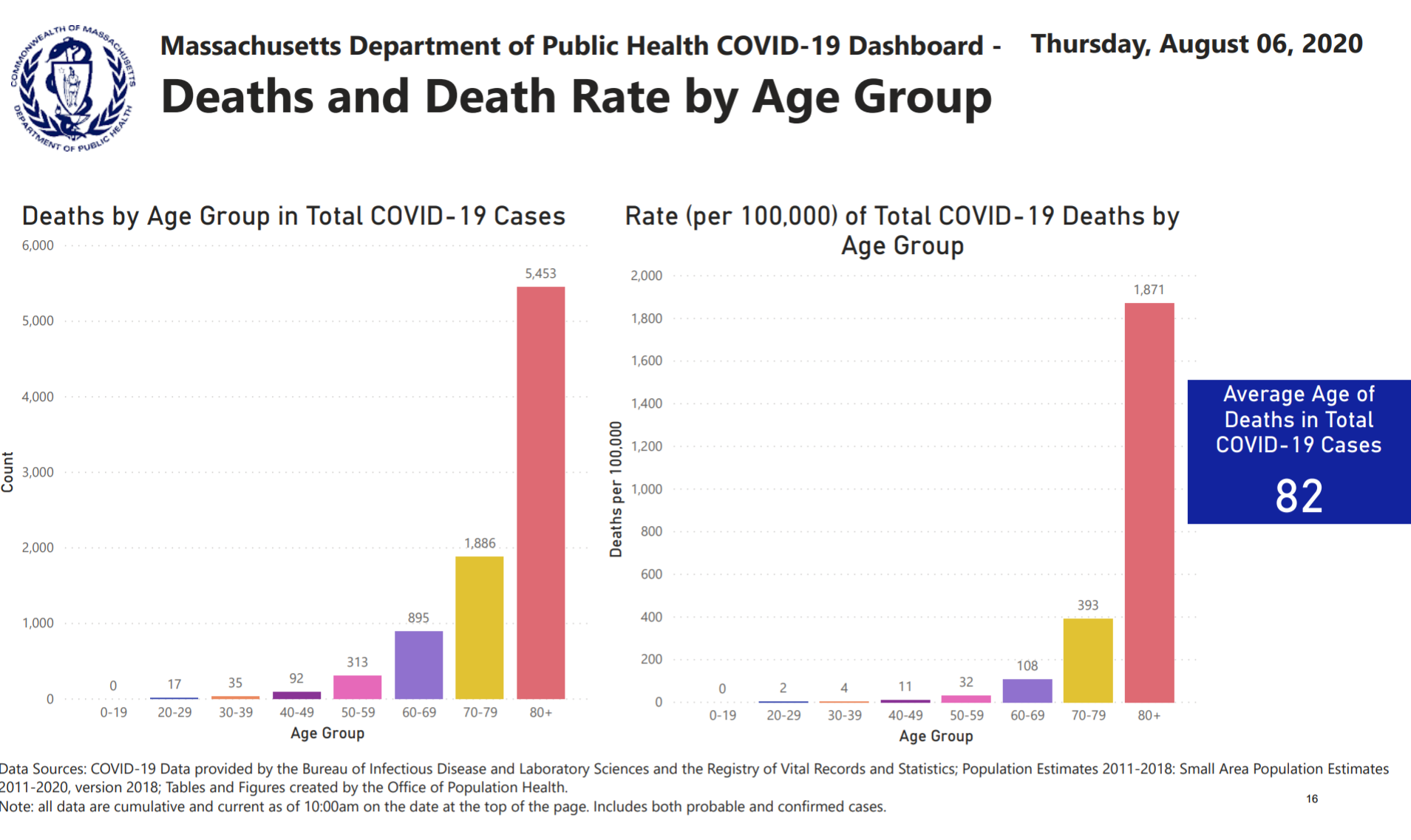
from mass.gov, statistics that have now been removed), but they seem to perceive Covid-19 as the main risk to their lives and health. They won’t take off their masks, for example, even when outside in mostly-deserted Cambridge. After talking to and observing them, I concluded that, at least for young Americans, Covid-19 is now primarily a disease of the mind. Support for my theory: “We’ve Hit a Pandemic Wall” (NYT, August 5)?
New data show that Americans are suffering from record levels of mental distress.
Let’s start with the numbers. According to the National Center for Health Statistics, roughly one in 12 American adults reported symptoms of an anxiety disorder at this time last year; now it’s more than one in three. Last week, the Kaiser Family Foundation released a tracking poll showing that for the first time, a majority of American adults — 53 percent — believes that the pandemic is taking a toll on their mental health.
This number climbs to 68 percent if you look solely at African-Americans. The disproportionate toll the pandemic has taken on Black lives and livelihoods — made possible by centuries of structural disparities, compounded by the corrosive psychological effect of everyday racism — is appearing, starkly, in our mental health data.
Turns out the extra ten extra pounds around my middle have moved in and unpacked, though I’d initially hoped they were on a month-to-month lease.
The newspaper that has been cheerleading for Shutdown now is surprised that there are some negative consequences? How did the coastal elites not figure out that not everyone’s shutdown experience would be positive? A friend in the Boston suburbs, who was a work-from-home consultant long before the Age of Shutdown, was telling me that his 8th grader hadn’t minded being at home for three months with minimal instruction being provided by the lavishly funded public school. Therefore, he concluded, shutdown was not a big deal, and if the school shutdown lasted another year that was okay too. His son would do fine practicing on the grand piano, learning from Ph.D. Dad and super smart stay-at-home Mom, etc.
I pointed out that not every American child lived in a 6,000 square foot $2 million house with two biological parents who get along at least reasonably well. Would he acknowledge that an inner-city child crammed into a two-bedroom public housing unit with mom, a step-sibling, and mom’s latest boyfriend might have a less favorable view of school shutdown? (he did!)
(see also “Coronavirus impact: Chasm grows between whites, people of color, California poll finds; Spanish-speaking Latinx voters say COVID-19 has seriously hurt their ability to pay for food and rent” (Mercury News, August 6))
Some top-voted NYT reader comments:
This is like the Twin Towers imploding all over again – except this time, one story collapses each day, and there is no ground floor.
The pandemic in and of itself is stressful but then add the stress of Trump’s daily tweets. The thought that he might get re-elected makes the stress almost unbearable.
What I think has caused the national stress-out, Ms. Senior, is that America now knows that it’s on its own. We don’t have a president who actually understands and cares about us.
I stress over the corrupt Republican leadership, so unconcerned for 99.9% of Americans that they let a a spoiled child throw our health, education, and welfare out the window, …
A coworker yesterday confided that about 15 of her relatives are COVID positive after a big family graduation party 10 days ago. I couldn’t hide my disgust. She is a very highly paid executive. We work for a research university health system!!! My neighbors just had a 40-person party for their 9-year-old. And seemed miffed and befuddled that many of us on the block declined to attend. They were all crammed under a tent shoulder to shoulder. Nary a mask in sight.
Maria from Maryland: The thing is, a lot of us are coming to the conclusion that all our problems are the same problem. Botched coronavirus response? Republicans. Insisting on doing things that spread the disease? Same. Economic deprivation? Republicans again. Two generations of failing to address racial issues? Again. Two generations of banging our heads against the same gender barriers? You guessed it. Failure to deal with climate change? Do you need to ask? Guns? Infrastructure? Science? Arts? They’ve been at it my whole adults life, ruining everything. And at their apex, they produced the very worst man in the world. There will be a vaccine for the virus, but what about the humans who are ruining our lives?
Coronaplague wouldn’t bother them at all, apparently, if Joe Biden were the Great Father in Washington right now!
Coronaplague obviously is a real problem for the elderly/vulnerable. And in societies where it is allowed to run wild, e.g., Sweden, it will kill approximately 0.05 percent of the population within a few painful months. But will readers agree with me that if young people are afraid of getting the disease personally, despite having no actual or planned contact with the old/vulnerable, then coronavirus has mutated into something whose main effect is mental illness?
Related:
- “Coronavirus Pandemic Causing Anxiety, Depression in Americans, CDC Finds” (US News): “MORE THAN 4 IN 10 Americans are struggling with mental health issues stemming from the coronavirus pandemic, a new survey found.”
It’s odd how purportedly educated people just repeatedly ignore anything about coronavirus that’s not mortality. Are they just pretending they don’t see the reports about post-coronavirus morbid conditions in the formerly healthy? Especially when the local baseball team just lost a pitcher for the year due to complications of coronavirus?
I think the 20 year olds know what they’re doing.
+1
Given they are finding this virus all over the body in people who have died from Covid, I am more than a little concerned about long-term effects, even among those who are asymptomatic. Wearing a mask isn’t that big of a deal. Surgeons do it all the time.
GC – could you please be more specific about “finding virus all over the body”? Namely what kind of magical technology was used for that finding?
Because neither RT-PCR, nor ELISA can do this kind of “finding”.
Re: long-term effects. What is the prevalence of these long-term effects? As far as I could discern the reported cases of that could be counted on fingers. (Complications resulting in long-term health effects from a normal flu usually run in tens of thousands every year).
Wearing a mask… Surgeons replace masks many times a day and are trained in proper donning and removal. Even with that there’s no clear evidence the masks do anything positive even for this cohort of people constantly exposed to sick patients. (A propos: surgical masks are not filters, they are mechanical shields preventing spittle from landing in open wounds and incisions.) They’re worse than useless in general population.
I agree.
It is about the same here in NYC too — the only people on the street are young people and they are all tightly masked while they walk aimlessly, cycle or run. I called a young woman who works for me to ask when she would be returning to work. She said she didn’t know because she said she was afraid to leave her apartment & get on the subway. The subway in fact is the most pleasant it has ever been– the cars are spotless because the system is now shut down for four hour each night to clean and empty. The vagrants and zombies have all been moved above ground, where they have now built shanty towns all over the place or stagger about in a stupor.
The young doesn’t have the benefit of much experience with real life – this being the natural outcome of spending too much time in coddled safe-space of academia.
They don’t understand that there are people who lie for living. And these are exactly the people who work in mass media and governments.
It’s not so much an illness as it is a plot device from a poorly written movie that does whatever the writer needs it to from one scene to the next, regardless of logic and continuity.
Phil, because of people who think like you, the US is now a pariah nation. If I wanted to travel to Canada to escape all the chaos going on in the US, they wouldn’t let me in. Does that not seem like a problem to you? Not even frickin’ Canada will let Americans into their country right now. I’ve spent months applying for jobs in better-run countries that aren’t falling apart. Many countries (I’ve run into trouble with Singapore and Australia so far) are not accepting even skilled immigrants from the US right now.
I couldn’t go to Coachella this year because the California government decided that having ~100,000 people drive or fly in, hook up with each other in porta potties, and fly home, posed a public health risk. Gee, go figure. Students at many universities can’t attend classes in person. Even if you think they’re all low-risk, which they’re not (some students have pre-existing health problems that increase their risk, and the probability of suffering long-term health consequences is of course higher than the probability of dying), many of the staff members they come into contact with (e.g. professors) are much older and are not. With the numbers involved, it is all but inevitable there will be stories this fall about students contracting coronavirus at a frat party and going home and killing one or both of their parents. And of course, if you pick up a COVID-related chronic health condition when you’re ~20 years old, you’re going to be dealing with the consequences for a loooong time.
We’ve tried “reopening” without fixing the underlying problem and found that it doesn’t work. People still lose their jobs and businesses still go out of business because people are afraid to expose themselves. All these problems will continue until the virus is under control. All the students therefore have a strong interest in getting the virus under control, as many other countries have done, which they can help out with by not spreading it. The sad part for everyone trying really hard not to contribute to the problem is that a substantial fraction of the US population is trying their hardest to make it worse, e.g. 300,000 people attending the Sturgis rally and refusing to take any precautions whatsoever.
Coronavirus is a problem all over the world, but the ridiculousness of our response is uniquely American:
https://twitter.com/TBPInvictus/status/1281256803788107776/photo/1
You wrote “And in societies where it is allowed to run wild, e.g., Sweden, it will kill approximately 0.05 percent of the population within a few painful months.”
Actually, there’s no guarantee it will stop there, since ~0.28% of NYC’s population died of coronavirus. The whole thing was a stupid gamble with tens of thousands of people’s lives at stake. The idea that cases necessarily go down after a few months and the problem goes away on its own is disproven by the current situation the US is in.
Ryan: I don’t think our perspectives are contradictory. If you want to say that these gals are protecting society and your ability to go to Canada by limiting their activities and wearing masks all the time…. great. (And, per the recent post about Biden ordering Americans to wear masks, I would pay young people for this service to the elderly.) But if they are limiting their activities and wearing masks in the 90-degree heat out of a fear for personal safety, that’s a sign of mental illness given the relative risk of Covid-19 for people their age compared to the risks of driving, flying, etc.
(I don’t think NYC is an example of a “society” and New Yorkers exhibited some unique incompetence, e.g., deliberately putting infected patients into nursing homes. NYC has a huge percentage of immigrants, who may be 10X more likely to die from Covid-19 than the native-born population. See “Large differences in excess mortality in the spring of 2020 based on country of birth” from the Swedish medical society. https://lakartidningen.se/klinik-och-vetenskap-1/artiklar-1/originalstudie/2020/06/stora-skillnader-i-overdodlighet-varen-2020-utifran-fodelseland/
People born in Somalia, Syria and Iraq, who are likely to be weakly established in Sweden, had a marked increase in mortality compared to people born in Sweden, the EU, the Nordic countries or North America in the spring of 2020 (Figure 2). A similar picture, but offset in time, is seen even if Stockholm County is excluded (not shown). In the age group 40–64 years, in March – May 2020, 122 deaths occurred in immigrant groups that are likely to be weakly established in Sweden, compared with an average of 38.5 in 2016–2019, a death rate of 220 percent. In the same age group, 1 percent lower mortality was seen among people born in Sweden, the EU, the Nordic countries or North America. Among those over the age of 65, there was the same excess mortality in the group with probable weak establishment (220 percent), but also some mortality (19 percent) among those born in Sweden, the EU, the Nordic countries or North America.
Ryan: In other words, NYC’s death rate is a good guide to what happens if you jam randomly assembled humans, who don’t have a language or culture in common, into a tight space. Millions of people all collecting welfare (e.g., living in “means-tested public housing” or subscribing to Medicaid) in the same geographical location are not a “society”.
Ok, the Coachella reference had me convinced this was a troll, but the rest of it seemed real (if demented)…
Anyway, I really hope one of those countries ends up accepting you eventually. I’d hate to have the chance of running into you.
I agree that NYC is a horrible place where everyone hates each other. I’m confused though about what physiological property people born in Somalia, Syria, and Iraq have that makes the virus 10x as deadly to these people. Surely such a discrepancy could only come from differences in behavior (whether voluntary or motivated by the circumstances, e.g. living with 20 roommates), which would seem to imply that the fatality rate *does* heavily depend on how we change our behavior in response to the virus.
jimbo: My coworker described going to Coachella for the first time as being better than losing his virginity (“it was the best weekend of my life”)
jimbo: I’m with Ryan on Coachella (how many more times can I go to Burning Man, after all?). It is California, so maybe we would find Willie Brown there meeting some ambitious 29-year-olds ready for political appointments?
Despite being a Church of Sweden member, I think it is premature to declare that only the Church of Sweden is the true religion. I’m still in the phase of trying to understand the perspective of the Church of Shutdown rather than being 100% sure that the Church of Shutdown is false. As noted elsewhere on this blog, a lot of the arguments that are purportedly about “science” are really about preferences and tradeoffs. Is educating children actually important to a society? If so, they will run schools and maybe, if someone asks, try to come up with a scientific justification for why it is okay to run schools. Is maximum safety from Covid-19 what matters? That society would probably not run schools and try to manufacture a scientific argument for why it was denying children what had been their right. You can’t say that the Europeans (run schools) are right and the Americans (don’t run schools) are wrong “scientifically”. These groups of people have different goals.
“travel to Canada to escape all the chaos going on in the US”
Mask wearing rate in Canada is lower than in the US, though. By this criteria alone, Canada is more chaotic:
https://www.ctvnews.ca/health/coronavirus/how-canadians-and-americans-are-responding-differently-to-wearing-face-masks-1.5013802
Ivan: Mask-wearing in Canada is less common?!?! And they have minimal coronaplague by comparison? Now we need to bring in the Divinity School scholars to work on this https://en.wikipedia.org/wiki/Theodicy problem.
Phil:
Well, they list other things that *may* be more useful to lower mortality, but people are looking for easy solutions in this country, e.g. just wear the damn mask ! … and everything will be as good as in Norway (where about 10% of people wear them).
Another interesting fact is that whites’ (to exclude other races for simplicity) mortality rate in MA is 3 times as high as this country average and 7.6x that of CA. It’s even higher than in NY. I cannot even guess why that is the case, with “the most advanced medical service in the world” and all.
https://www.apmresearchlab.org/covid/deaths-by-race#white
… as of Aug 4th.
> My coworker described going to Coachella for the first time as being better than losing his virginity
Either I’m not going to Coachella right, or he’s not having sex right.
Today I had a primary care appointment with my doctor, who practices at a local hospital. As has been the case with all my previous hospital visits since April, the hospital was virtually empty. A tiny trickle of patients come through the doors every 15 minutes or so, the parking lots are less than half full. The hospital was spotlessly clean. Every surface looked as though it had been washed, buffed and polished. Signs on the wall announcing the closing of the gift shop through the end of May were still hanging near the elevators. It looked as though nothing had been touched in the entire facility for months.
The fun, this time, was seeing how well the hospital system is caring for its most important patients – the physicians. Back in June I had a telemedicine visit with the same doctor, who I guess has been forced to actually spend a few hours at the hospital in the past couple of months. The procedure was:
Wait in the observation room for about 15 minutes while an assistant does the blood pressure test, asks me all the questions and clicks through two dozen screens on the PC, then disrobe, etc. Sit down in the chair and – get this – wait 10 more minutes for the doctor to ** call me on my cellphone from his office down the hall **. This is to “limit exposure” to anyone who potentially has the plague. I’ve been tested negative twice in the past month, so I’m sure I’m OK. So I’m sitting in a chair in the obs. room while he chats with me on the phone, but the cellphone reception deep inside the hospital is terrible, and the call drops out. He has to call me back. I struggle to hear what he’s saying, but I can literally hear his voice from his open office door 20 feet away. Once he’s gathered whatever information he needed, I wait another 15 minutes while he gets ready to run the gauntlet by actually seeing me live and in-person. He walks into the room wearing *two* masks, glasses and goggles, and latex gloves. This so he can put a tongue depressor in my mouth and check my nose, ears, eyes and reflexes. He asks me a couple extra questions, backing away from me carefully on his way out the door. His total “exposure time” was about 4 minutes.
It has become perfectly clear to me that the single most important priority in health care where I live is to protect the doctors and the buildings they work in at all costs.
I had my physical exam this past Monday, at local office not hospital.
The day before, someone from the office called me and asked me what car I will be coming in with? I said why you need to know? She said so I know how to find you. I had to wait in the car and was walked into the office and exam room by the nurse who was in full protective gear wear top to bottom.
My Dr. was the same, he had full protective gear on him and kept his distance of about 5-6 feet and when was wearing gloves all the time and did minimal touching when examining me.
When I was asked to give a sample of my urine, I was surprised I was let go alone to the bathroom to do my thing. Someone before me or I could have spit all over the bathroom, door handles, etc. and transmitted the Covid-19 to me or others. I almost wanted to call this out to my Dr. but given how he was geared up, I know there is no point.
The whole thing felt like I was in a movie script.
Another story.
My local library is finally open, sort of. You can request material online and pick them up in person. It takes at least 2 weeks for the item to be ready. Why? They have to disinfect them before they hand it out to you, in a bag.
Pickup is by phone appointment only and you have 15 min to do so from you appointment. The few staffs are behind glass wall and you can only walk into the open front door.
After having this experience few times in the past month, I cannot wait to see what they will do at public schools, if and when they open.
@George A.:
That sounds about right and it’s impacting a lot of small-town libraries very hard. Why wait two weeks to get a book printed on dead trees? A lot of people just won’t bother.
I’ve done some work in the past for a local library in a small town. It’s one of those little places staffed primarily by volunteers who absolutely love their town, the people, and what they’re doing, while always teetering on the brink of insolvency because of the Internet and all of the profound changes it has wrought in our culture. So in the past 10 years, they’ve vastly expanded their “extracurriculars” in an attempt to bring more kids and families to the library, through a plethora of varied programming beyond the traditional “borrow a book, or sit in the library and read it.”
Well, they’ve been hammered by COVID. In addition to following all the sanitation guidelines you mention, the fact is that fearful parents just don’t want their kids going anyplace “unsafe” – much less bringing anything unsafe home with them – so their already small daily traffic has dwindled. This is a real shame. Even in the best of times, the Library runs annual fundraisers, bake sales, potlucks, etc. to keep the lights on, and now they may close for good after more than 125 years in continuous operation and a history dating back to the Revolutionary War.
They didn’t close during World War II, but coronaplague may get them, despite the fact that there have only been a handful of positive cases in the town, and zero deaths.
People might say: “Well, we don’t have glass-blowing works, blacksmiths and cobblers any more. Why do we need libraries?”
Well, I guess we don’t *need* them. But they’re very nice places to go. Quiet, a little out-of-the-way, and a safe place to read and think when you’re a bookish person trying to be alone with their thoughts. And Kindle (or any other e-book) still isn’t the same, or as good.
Hospitals are of course one of the most dangerous places you can be in a pandemic (or really at any time) since they’re where sick people congregate.
I, for one, fully expect to see “COVID Brain” included in the DSM-6
The mortality rate is not the issue for young people, its the risk of chronic illness upon exposure. The risk of pulmonary damage after recovering from infection is a not insignificant in patients 20-34 (26%), and it is looking more like a pulmonary fibrosis post-infection that can have lifelong consequences. Studies show 57-65% of recovered patients have “ground glass opacities” visible in lung CT scans that indicate incipient fibrosis – the first stages of a lifelong course of irreversible interstitial lung disease .
https://www.cdc.gov/mmwr/volumes/69/wr/mm6930e1.htm#F1_down
https://www.cdc.gov/mmwr/volumes/69/wr/mm6912e2.htm?s_cid=mm6912e2_
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7228737/
Pharma Guy: If you are sure that young people who are exposed to coronavirus generally become cripples, why not trade on this information? Short the Swedish market and go long New Zealand, Vietnam, Laos, Cambodia, and Australia, for example. The Swedes did not wear masks and did not close their schools. Thus, it is now a nation of people whose health is seriously compromised. Shouldn’t that slow down their long-term economic growth? With some leverage, you could become wealthy enough to purchase a Gulfstream!
Given that Sweden is a wealthy developed country with a large welfare state, it seems totally reasonable to assume that Vietnam, Laos, and Cambodia are harder-working than Swedes and their economies will grow faster. Australia and New Zealand rank very highly for economic freedom (http://www.heritage.org/index/ranking) and are currently very well-positioned to attract capital and high-skill immigrants (e.g. say Google wants to expand in a country where people can actually work together at an office), so we can also expect their economies to do well for the immediate future. This is even before taking COVID into consideration.
What’s the case for why anyone should move to Sweden? Pay higher taxes and increase your chance of getting coronavirus? So that’s a high-tax country that’s not competitive at attracting capital or labor, where the large welfare state discourages people from working very hard or starting a business (this appears to be the future of the US as well).
Pharma:
Did you read your own references ? When you twist the words from the original articles
so much, you lose credibility:
1. The article #1 does not say that “risk of pulmonary damage after recovering from infection is a not insignificant in patients 20-34 (26%)”. Instead, it says “symptomatic respondents reported not having returned to their usual state of health by the date of the interview (median = 16 days from testing date), including 26% among those aged 18–34 year”.
2. Article #3 does not say “Studies show 57-65% of recovered patients have “ground glass opacities” visible in lung CT scans “. Instead, it says that “In this series[first series of hospitalized Wuhan patients], 36 (26%) patients required intensive care, of whom 22 (61%) developed acute respiratory distress syndrome”. The article *speculates* that there may be consequences, rightfully so, but so far there is not much statistical, not fear mongering, evidence to that effect: “No post-discharge imaging or functional data are available for patients with COVID-19”.
Anecdotal evidence regarding recovery time. An acquaintance of mine who is a 40 year old marathon runner (Boston, NY, etc) got sick in April (corona infection was confirmed by post recovery antibody tests), spent 8 days with high fever, did not bother going to the hospital for fear of getting invasive treatment, resumed exercising 3 days after temperature became normal. Recovery took longer than from flu, about two weeks. He started with 5miles, now runs the usual 10m.
It’s been a mental disease from the start. Personally I think these people are permanently scarred from the sniffle-plague pysop and will not be right in the head for a long time if ever. If they think a vaccine is going to end the ‘we’re all going to die’ media onslaught, and bring peace inside their heads, they will be disappointed. This thing has given two-bit governors so much power they ain’t ever letting go.
Yes, Ivan you are correct, I was mistaken about the pulmonary complications post-infection. The correct number is 83%, not 57%.
The correct numbers are: ground-glass opacifications – 83%, ground-glass opacifications with mixed consolidation – 58%, adjacent pleural thickening – 52%, interlobular septal thickening – 48%, air bronchograms – 46%. Of course, these numbers demonstrate multiple pathologies in patients that can occur simultaneously due to inflammatory lung damage.
This was from a review of chest CT studies published in the last 6 months: https://pubmed.ncbi.nlm.nih.gov/32283052/
Not including hematological problems (e.g., lymphopenia in 67-90% of patients with the disease) and other non-pulmonary complications, it is not a trivial disease.
https://www.nature.com/articles/s41591-020-0968-3
Pharma:
You are not stating your case in good faith again:
1. First, you claimed that “the risk of pulmonary damage after recovering from infection is a not insignificant in patients 20-34”. The first reference in your second message does not say anything about young patients at all but rather says that “The detection of COVID-19 chest CT imaging is very high among symptomatic individuals at high risk” likely based on Wuhan studies. We know that 20-34 yr olds statistically are not “individuals at high risk”.
2. Second, neither of you references “show 57-65% of recovered patients have “ground glass opacities” visible in lung CT scans (your claim) because “No post-discharge imaging or functional data are available for patients with COVID-19” (from your own first message reference).
No one disputes that corona is a non-trivial disease for 80 yr. olds, but the original comment was about 20-year-olds for whom indeed it is trivial, on average.
People are not understanding the COVID paradox
In the USA,the exposed cases are at least 20 times the number of the current detected cases,of 3.5 million,AND THE ACTUAL INFECTED CASES ARE AT LEAST,1O TIMES the current detected cases.
The current daily count in the USA is around 70000 and was around 25-30,000,a fortnught ago.These incremental 35000 were EXPOSED around 27 days ago (at the earliest) and were INFECTED ENOUGH,to take a TEST (after the symptoms came to light – 27 days,hence)
Therefore,it is safe to assume that for every 70000 cases today, there are at least 70000 more INFECTED, BUT NOT WITH SUFFICIENT SYMPTOMS TODAY,plus some more,WHO DO NOT WANT TO GET TESTED AT ALL.
Further,for every 1 COVID positive person WITH SYMPTOMS – it is safe to assume an EXPOSURE RATIO OF 10:1 IN A SPAN OF 30 DAYS – starting from the time when the COVID +ve person was 1st EXPOSED.We are ignoring the AYSMPTOMATICS – who CAN ALSO INFECT.
So for the 70000 cases today, there are AT LEAST 70000 more COVID positive persons (based on 1 day’s data),which makes it 140,000.These people have exposed,at least 1.4 million, in the last 30 days !
So,if you look at the number of cases in the USA, in the last 30 days,at 30000 a day,so you have a ROLLING stock of , 6 million EXPOSURES just in 30 days – who will show symptoms in the next 7-30 days,and so,the numbers will skyrocket.
Based on a population of 350 million – IT IS ONLY WHEN THE USA has 17-20 million DETECTED CASES – that the COVID saga will end.There WILL be NO CURE,AND NO VACCINE – just trial and error diagnostics.
So we are a long way away.dindooohindoo
30 days ago,the USA COVID cases were around 1.5 million and so the EXPOSURES were at 30 million.From that 30 million – in the last 30 days – the USA has had around 35000 cases per day,in the last 30 days – which is around 3% of the EXPOSURES,as of 30 days ago.
The Rolling stock as above,WILL DOUBLE IN A MINIMUM OF 30 DAYS, and the 3% will also DOUBLE, IN EVERY 60 DAYS, at the minimum.These are the coordinates of doom.
There is NO STATISTIC on 1 PARAMETER.How many COVID discharged humans in the USA were re-infected,and in what duration ? That is the ONLY HOPE – id.est., to be infected and survive.Can it REALLY BE ZERO ? Or does it show THAT releasing a COVID cured patient into the jungle – is the biggest disaster – a ticking neutron bomb ? These are the VULNERABLES – whose immunity and anti-bodies,CANNOT last very long. That is HOW the VIRUS was PLANNED.
USA numbers look devastating,as they have the infra,to test on that scale.The situation in other parts of the world, is BEYOND redemption.
Even in the USA,the sharp rise in Cases,is NOT DUE to the re-opening of businesses – BUT DUE TO LACK OF TESTING.It is the people who WERE NOT TESTED,in the last 30 days, AND HAD synptoms, in the interim – which is reflecting in the current data,of 70000 a day.
You can imagine the CATASTROPHIC DOOM,in Brazil and India – where THEY WILL NEVER be able to test,on the American scale.
In essence,the entire population of 7 billion,HAS TO BE infected,and at least 10%,will die due to COVID,and 10% more will die,due to other morbidities,which will have no medical attention and another 10%,will die due to starvation.
The persons who will die,are those,with a weak and infirm constitution,and low natural immunity – and whose body,is already damaged by medicines,steroids,nicotine, cocaine, adulterated food and alcohol.
A Perfect Constitution,is an essential,for a Perfect Brain
This is the Greek Formula,updated for AI + Robotics + Nanotech
The Greeks used to discard their defective samples,at BIRTH,on Mt Olmypus,for the ravens and vultures.That was he Priori Best Practice.2000 years since then, AI + Robotics + Nanotech, has made Humans obsolete.
Thence,comes in COVID – just like Pure Providence.After the 10+10+10% culling – we will get the NEXT virus – which will be in action,by November 2021.That virus will target,in Phase 1,the clowns CURED BY COVID – as the COVID bird has laid its nest in them.Then it will target those who were infected by COVID but did not show the symptoms.
Like a never ending Geometric Progression – towards redemption and salvation,like Zeno’s Paradox.