We have been barraged by emails from our kids’ schools during the Christmas vacation week. If we traveled, the public school administrators want to know where and when and they want to see medical records of a PCR test (required under the governors’ travel orders, though at this point most other U.S. states have a lower rate of COVID-19 cases within 7 days compared to MA). Example:
We will be strictly enforcing the Governor’s Travel Orders and sending students home when we learn about travel and have not received notification and verification of required test results.
The school actually requires additional testing and quarantine days (14) beyond the referenced travel order, which requires 10-day quarantines and testing for those 10 and older:
Children who are 10 years or younger are not required to have a test. However, without a test, they must quarantine before returning to school. So, families will need to choose to either have their children tested and provide the result of the test to the school nurse so that they can return to school immediately if the results are negative or they will need to keep their child home in quarantine for 14 days if a negative test is not provided.
(i.e., if children can keep quiet about that trip to Disney World, they can continue to receive an education!)
The kicker to all of this is that COVID-19 tests aren’t available, except to the mostly-imprisoned college students who don’t need them (they get tested twice/week). Here’s one self-pay $80/test service (recommended by a private school administrator) that you might think would have slots because they don’t take insurance and don’t provide the taxpayer-funded testing that was supposed to be Americans’ right:
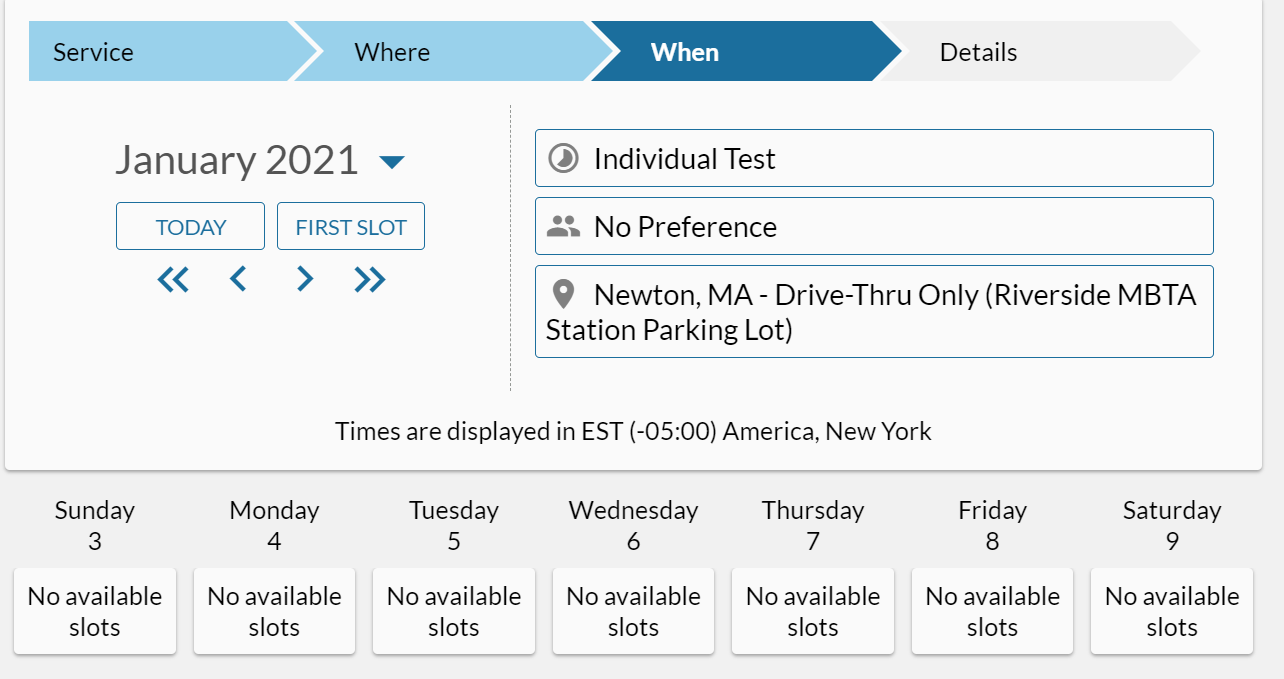
As of Sunday morning, it would be possible to get a test on Friday evening in the Cambridge location:
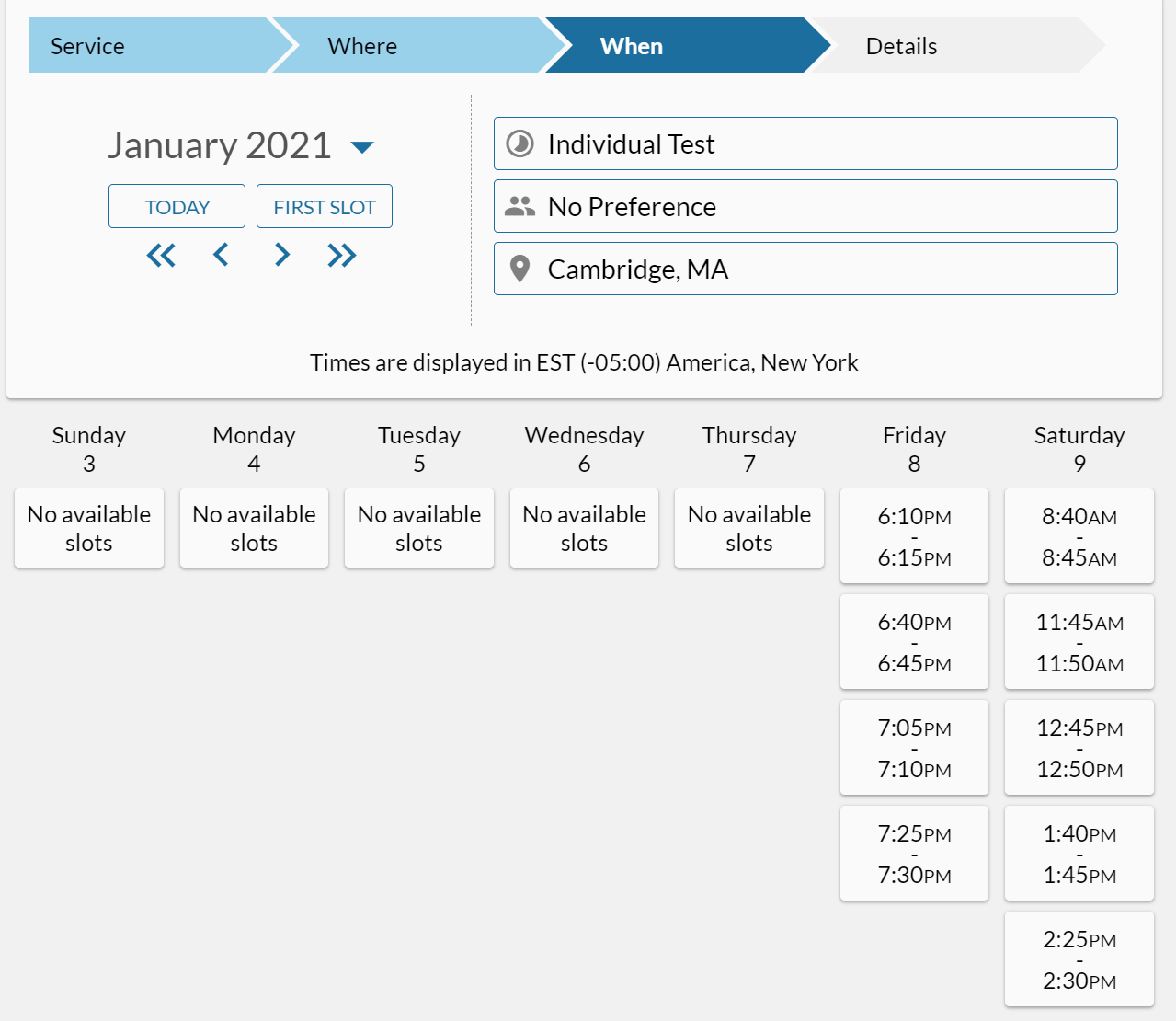
So the result would come back on Monday? That’s 8 days later and the governor’s travel order requires a 10-day quarantine. So the effort and $$ for the test shortens the quarantine period by only 1-2 days.
Separately, one thing that is great about Americans is that we won’t give up our passion for bureaucracy and paperwork even after we declare an “emergency”. For example, although a non-physician (the governor) orders subjects to get tested after travel, a subject can’t actually be tested without paying a physician in addition to paying the lab. From the CIC Health site, regarding pricing for organizations:
To cover the physician who provides the legally-required referral, the clinician to oversee the test, the software for ordering and reviewing results, and logistics support. This fee ranges considerably based on the components required, and range from $5-$35.
As there is no medical treatment for COVID-19 (remdesivir is approved by the FDA, but considered useless by the WHO) and the vast majority of folks who test positive for COVID-19 have no symptoms and the person getting the test probably isn’t sick to begin with, what is the point of paying a physician?
Finally, let me note that rich white people seem to be ignoring the travel order. Friends with vacation houses in other states go to and from freely. A friend recently met up with us for a dog walk in the woods. He talked about having just returned from a ski trip to another state. I asked “Unless you were skiing in Hawaii, didn’t you have to get a Covid test to comply with the governor’s travel orders?” He responded that he hadn’t bothered and wasn’t going to bother. What’s his day job? Physician.
Related:
- Turboprop coast to coast to coast with youngsters (we managed to get a test, but in Kentucky where they’re apparently better organized)
- beacontesting.com, a massive project; on January 3, the site showed “no upcoming times are currently available” at any of the Boston-area locations, but a 2.5-hour round-trip drive to New Bedford, MA would have enabled a test on January 4
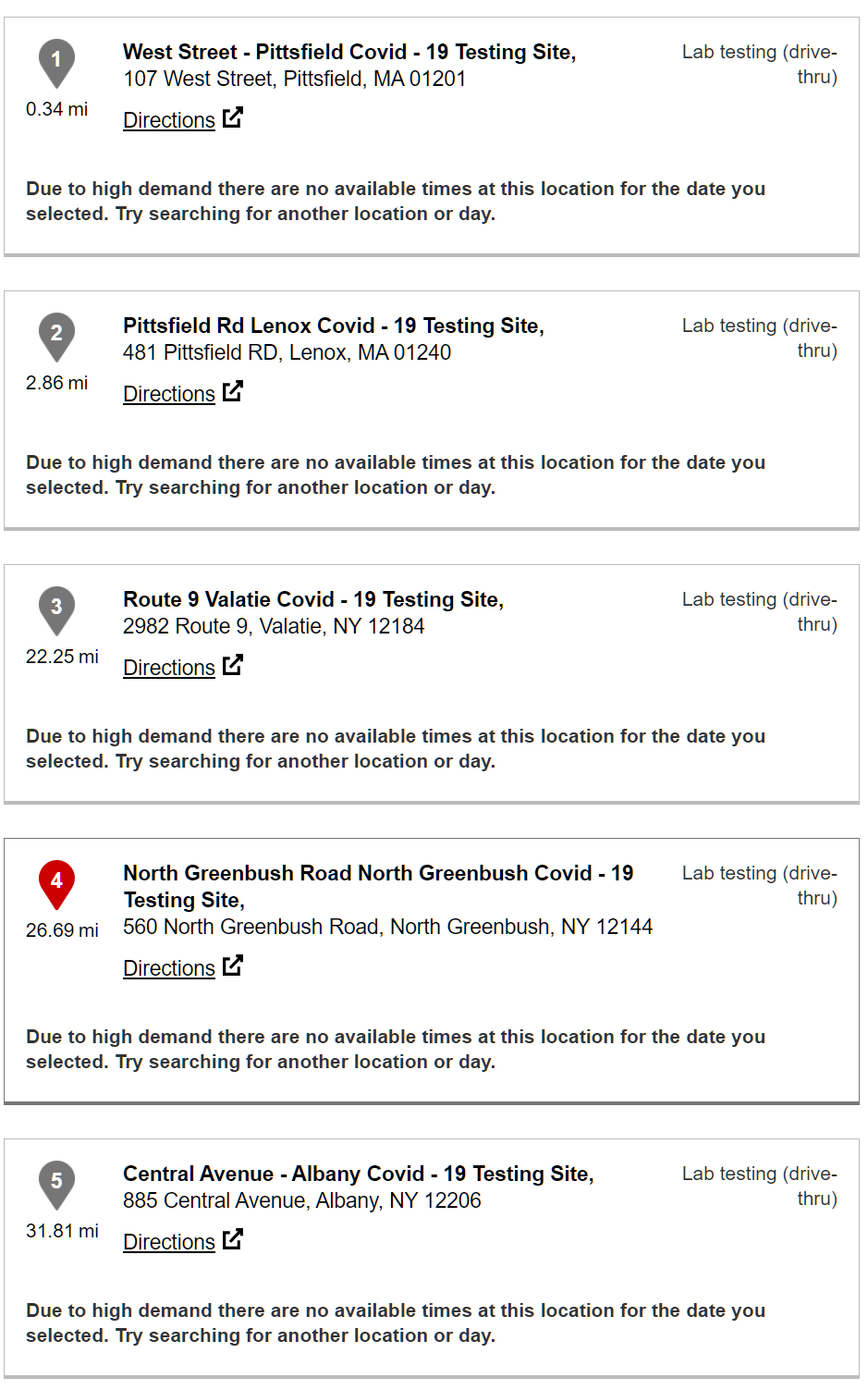
Update: Patrick, below, asked whether the situation was better in Western, Maskachusetts, e.g., Pittsfield. The answer seems to be “no”. As of January 3 at 2 pm:
Update from a friend who is considering a brief trip from his all-white COVID-free exurb of COVID-plagued Boston (he’s locked down in a 12,000 square foot house on 10 acres) to rural Maine:
I see. So if I leave MA, go to Maine, and come back – I must quarantine for 10 days. But if I go to Boston and back, I don’t need to. Got it.
We’re already in the Soviet Union, with the only caveat being that we’re doing even worse than they would have:
Bill de Blasio can’t get NYC vaccinated but claims he’s doing great and it’s the Governor’s fault:
https://nypost.com/2021/01/03/scott-stringer-slams-frustrating-nyc-covid-vaccine-rollout/
Half the health care workers don’t want the vaccine:
https://nypost.com/2021/01/01/alarming-number-of-us-health-care-workers-are-refusing-covid-19-vaccine/
Combined with the school closure article in the Washington Post and practically anything else you read, the United States has, on the whole, devolved into mindless incompetence and “protect my ass” buck-passing on every level. We are the apotheosis of technocratic paralysis and systemic rot.
Tangentially related to systemic failure: Yesterday’s trip to a large US Postal Service facility in a pretty big U.S. city, to try and conduct some Saturday New Year’s mailing. We’re working on a Saturday, but nothing else is:
First we cannot get the paperwork processed online through the USPS business web portal, because it’s been down for more than 48 hours with no ETA on return to service. Usually Saturday is a good day to visit this particular facility, so we drive there anyway in the hope that one of the supervisors we work with can process the mail on their in-house system. Nope. Dead as a doornail. The facility is a mob scene. They have a huge room full of pallets of holiday mail and packages backlogged as much as a week awaiting sorting and transit to the endpoints of the network. “It’s chaos here right now. We can’t take that mail. Hopefully by Tuesday or Wednesday of next week things will ease up” he says. We try to snag a couple hundred postal trays of various sizes, so that at least we can continue working on our jobs. Nothing is available. All of the mailing equipment like trays and tray covers are in use because of the backlog. He manages to scrounge together 50 trays for us, which will get us through perhaps one of our jobs. Why is the backlog so bad? “It’s system-wide, and we had a lot of absenteeism with people taking extra days off through the holidays, even though we urged them not to. We’ve also had some COVID attrition but that’s not the biggest reason.”
This is why you have not yet received that Christmas card your Aunt Matilda in Toledo sent on December 15th.
@philg Were you able to determine that testing was completely unavailable throughout the state of Massachusetts? How about Pittsfield? Or should people be expected to travel for vaccinations, but not for testing?
“But it is not such a severe emergency that anyone should be expected to travel beyond his/her/zir/their immediate neighborhood in order to be vaccinated …”
I would say that a 2.5-hour round-trip drive is a little farther than anyone here in Maskachusetts, regardless of residential neighborhood, would have to go to get to the nearest CVS MinuteClinic (if CVS, for example, had been one of the bidders under my proposed scheme). And I don’t think that you ever established that a government central planner would have been able to distribute vaccination clinics more widely than what CVS and Walgreen’s have.
However, because you asked, I checked in on the state’s web site and found that there are no COVID-19 testing appointments available within an hour’s drive of Pittsfield in the foreseeable future. I will update the original post.
(Separately, I actually would be happy to travel 2.5 hours round-trip, either in my own vehicle or in a righteous billionaire’s COVID Vaccination Bus for the Underprivileged in order to get a vaccine shot. But for tests that are required for a child to return to school after a sniffle, or for a family to escape quarantine after an overnight trip to see a relative in Maine, a 2.5-hour drive is too much. And the state government’s central planners have now had 10 months to figure this out.)
Quote above found at this link:
https://philip.greenspun.com/blog/2020/12/31/american-central-planners-tackle-vaccine-scarcity/
Also at that link:
“Patrick: It would be like everything else in American retail and services. There would be a huge concentration of potential buyers with money in, say, downtown Boston. Yet all of the suppliers would be a 2-hour drive away in Pittsfield, Maskachusetts. That is how the market works and why central planning yields far superior matching of buyers and sellers.”
Why should testing be different than anything else? Why do you seem surprised that testing is not available in a convenient location?
Also, sorry, you did mention testing was available in Cambridge. So the only problem is the length of time you have to wait for results, not the travel?
Testing that would have a practical medical, personal, or epidemiological value is not available anywhere in Maskachusetts that I could find, with the exception of that single New Bedford site. The opportunity to be tested in Cambridge on Friday evening (i.e., waiting through Sunday, Monday, Tuesday, Wednesday, Thursday, Friday, Saturday, Sunday, and most of Monday for a result) does not strike me as useful if the goal is getting a child back into school and the waiting period of the result is, as noted above, roughly the same length of time as the required quarantine period.
If you rig the bidding so that CVS and Walgreens and other major chains are certain to win, then fine. You seem to have omitted that from your original proposal:
“I wonder if something more like a market economy could have done this better. The bureaucrats can send free vaccine doses to hospitals, medical and dental offices, and nursing homes. Whatever is left over goes to whatever clinic or facility bids the highest.”
You think the bidding would have to be rigged for the biggest and richest enterprises, with the largest network of locations, to win the largest supply of vaccine?
@philg Why aren’t CVS, etc. currently providing testing at all their locations in Massachusetts? Are non-market forces preventing that?
Patrick: If your goal is to do something about an infection that has, according to the CDC, so far afflicted approximately 162 million people (20.34 lab-confirmed cases times 8), I think asking why CVS hasn’t ramped up its capacity to do doctor-ordered and state-licensed-technician-administered testing is the wrong question (though it has an obvious answer: there is a limit to how many state-licensed humans exist). You would need some sort of at-home test. And schools that are requiring testing for students to be educated would need an at-school test. https://www.nytimes.com/2020/12/03/us/coronavirus-saliva-testing-home.html notes that, even in early December before California reached max plague level, “Pharmacies in the Southern California suburbs are advising customers lucky enough to score appointments that it could be four days before they receive results. In Chelsea, Mass., a line of people who hoped for testing, pelted by rain and wind, strung along an entire block early this week. In Atlanta, people have idled in cars, sometimes for hours, to get swabbed at drive-throughs.”
(could we do a two-shot vaccination of all U.S. adults with the same level of bureaucracy and regulation that we apply to testing? Maybe. https://ourworldindata.org/grapher/full-list-total-tests-for-covid-19?time=2020-02-20..latest says that, after nearly a year, the U.S. has managed to do about 240 million COVID-19 tests)
Philg – two little items regarding CVS/Walgreens etc. First, it seems that a large portion of the planned 20 million vaccines that were supposed to be complete by the end of 2020 under warp speed and have not been completed were the CVS/Walgreens efforts in nursing/retirement homes. Seems like that side has been allocated a lot of money and not yet delivered… so not sure how that factors into your “market based” approach. Second, on the positive side I can get a test at CVS here in NC pretty much any time I want.
The point of how poor “central planning” is working has been made in some posts. This is all a question of interpretation. There is a school of thought indicating that the problem is that we have 50+ independent organizations trying to do this without enough “central planning.” I would also guess that the CVS and Walgreens would be doing quite a bit of “central planning” as they roll things out…
At least I get my vaccine this week!!
LP: I am not sure that it is fair to criticize the CVS/Walgreens folks. Remember that I have chronicled the Facebook chorus of vaccine injection pace scolders, not joined them. https://ourworldindata.org/grapher/covid-vaccination-doses-per-capita?tab=chart&stackMode=absolute&time=latest%C2%AEion=World shows that the U.S. is #4 in the world in percentage of the population that has been vaccinated. It would be nice to be #1 (out of nearly 200 countries), but I am not sure what entitles us to be the outlier. We stole a huge chunk of land from the Native Americans and that has made us richer-than-average, but is it obvious that, merely because we are richer-than-average we are also much smarter than average?
(For comparison, France vaccinated 352 people in all of December. https://www.france24.com/en/france/20210103-france-vows-to-boost-pace-of-vaccinations-after-slow-rollout-fiasco ; admittedly this was partly due to the vaccine not being approved by the EU until Monday, December 21: https://www.rfi.fr/en/france/20201221-european-union-regulator-approves-pfizer-biontech-coronavirus-vaccine )
I think this mirrors what we did with COVID-19 in general. We waited until a bunch of statistics were available. Then we seized on some outliers, e.g., Taiwan and New Zealand (surrounded by the world’s best border barrier: an ocean). Then we said “It is obvious that we should have been the outlier instead of these two that we picked.”
@philg How is testing currently being administered in Massachusetts? Are private companies free to provide testing to the public at market prices? Or is overregulation by government authorities the problem?
Patrick: I wouldn’t say that “overregulation” is a possibility because one can never have enough government regulation! We should remember Edward Tufte’s point: “Every single oxycodone pill was approved by the U.S. Food and Drug Administration, and was made by licensed drug companies, prescribed by licensed doctors, sold by licensed pharmacists. All 72,000,000,000 pills (500 pills/U.S. household) were tracked to the exact place/time/amount of sale by the Drug Enforcement Agency.”
COVID-19 testing in Maskachusetts was delayed for approximately 1.5 months by the CDC. See https://www.technologyreview.com/2020/03/05/905484/why-the-cdc-botched-its-coronavirus-testing/ (“The first testing kits from the Centers for Disease Control had a simple fault, and red tape prevented other labs from creating their own.”)
As noted in the original post, Maskachusetts makes it illegal to do a COVID-19 test without paying a physician to order the test. That will reduce capacity given that the U.S. has a small supply of physicians per capita compared to a lot of the EU nations.
I don’t think that there is anything about COVID-19 testing in Massachusetts that is recognizably part of an Econ 101 market.
@philg “As noted in the original post, Maskachusetts makes it illegal to do a COVID-19 test without paying a physician to order the test.”
https://www.umassmemorialhealthcare.org/marlborough-hospital/covid-19-dph-testing-site-marlborough-hospital
“Individuals do not require a physician’s order or to have symptoms to be tested.”
Is UMass Marlborough Hospital offering tests illegally?
If they do not employ any physicians who are capable of supervising their testing program, then yes, UMass Marlborough Hospital is offering tests illegally. (In my limited experience, however, an enterprise that calls itself a “hospital” usually employs at least one physician.)
Is this another illegal operation?
There’s a menu item “referral not required”.
https://memamaps.maps.arcgis.com/apps/webappviewer/index.html?id=eba3f0395451430b9f631cb095febf13
Not sure if it is reputable, but I reached it from the Mass General website.
https://www.massgeneral.org/news/coronavirus/massachusetts-covid-19-testing-sites
Lots of locations show up with referral not required, but maybe there’s no actual availability?
CVS also does not require a referral from a state-licensed physician or nurse-practitioner other than the ones whom they employ (and they also don’t have any available slots!).
My most recent test, at a CVS in Kentucky, was ordered by “PCP: Lori Williams, NP”, according to the paperwork. (I think it is quite likely that Lori Williams is a nice person, but I never spoke to her. There is a questionnaire that one must fill out prior to receiving a test at any of these locations. Maybe the state-licensed physicians and NPs are reviewing the question answers before people come in and, if they deem it sensible, diverting some of them to hospitals for immediate treatment?)
If McDonald’s wanted to buy a PCR machine and offer tests at its restaurants, that would be illegal unless they could also find a physician, NP, or similar state-licensed provider to supervise the testing program.
You originally said “Maskachusetts makes it illegal to do a COVID-19 test without paying a physician to order the test.”
But that just means
“employ any physicians who are capable of supervising their testing program” ?
I love your thinking Philip!
As noted in the original post, the lab that offers testing says on its web site (regarding mass testing for schools and companies): “To cover the physician who provides the legally-required referral, the clinician to oversee the test, the software for ordering and reviewing results, and logistics support. This fee ranges considerably based on the components required, and range from $5-$35.”
So if you pay the lab the $80/test fee for a consumer test, you’re presumably indirectly paying a physician. To say that you’re not is like saying that people who rent apartments don’t pay any property tax (since the landlord actually writes the property tax check).
But it seems as though you know the Maskachusetts law better than this lab does and they actually don’t need to keep paying a physician. So why not call them up and share your insights so that they can start making $5-35 extra profit per test?
@philg You earlier provided this quote “To cover the physician who provides the legally-required referral,” which you attributed to “CIC Health site” but you did not seem to provide a link? Is it this https://www.cic-health.com/. That seems to be a commercial provider, not a legal reference?
This website, linked by Mass General has an option “referral not required”.
https://memamaps.maps.arcgis.com/apps/webappviewer/index.html?id=eba3f0395451430b9f631cb095febf13
How do you reconcile those?
These is nothing inconsistent about what you’re citing. Depending on your insurance, for example, you might need a referral from your primary care doctor in order to have the insurance company pay a specialist doctor (like Dr. Jill Biden, MD!). The question about the referral is whether you need two doctors or just one. Similarly, although we are informed by our media that most U.S. physicians have quit their jobs due to COVID-19 stress, as long as the Mass General Hospital has at least one physician on staff they can do whatever testing they want to in accordance with M.G.L. c. 111D, section 8 (7). The apparent discrepancy that you’re citing occurs because “CIC Health” is a lab and doesn’t have an in-house staff of physicians whereas MGH is a hospital and physicians show up to work there every day.
@philg Given that the test site needs a clinician to contact every positive test result, the incremental burden of needing a clinician to sign off once on the entire test site seems rather minimal to me.
As you yourself pointed out, however, when the clinician signs off to allow testing to begin, the clinician is also agreeing to deal with requirements for handling the output of the tests, e.g., telephoning patients who have tested positive (or making sure that someone else who qualifies under Massachusetts law does the telephoning).
The web site cited in my original post: “To cover the physician who provides the legally-required referral, the clinician to oversee the test, the software for ordering and reviewing results, and logistics support. This fee ranges considerably based on the components required, and range from $5-$35.”
They’re not saying that they need the $5-35 for the blanket letter. They need it to deal with all of the regulatory requirements that are above and beyond the regulatory requirements for the lab test itself.
@philg How much would it cost to get all the positive cases on the phone with a clinician, the reporting requirements, etc? This site claims the positive test rate is 6%, but I’m not sure how authoritative it is.
https://covidactnow.org/us/massachusetts-ma?s=1484440
Could the cost and logistics of dealing with positive cases be a major bottleneck?
My most recent test, at a CVS in Kentucky, was ordered by “PCP: Lori Williams, NP”,
Did you actually consult, in person, with Lori Williams, NP before receiving the test?
If not, the required referrals don’t seem that burdensome.
Would this help?
https://covidinstanttest.net/
They ship overnight via fed-ex.
With rush shipping a five person kit will cost $525.
M: Thanks for that. The at-home antibody test would not help here in Maskachusetts because children are denied the opportunity to learn if they don’t get a PCR-based test (and adults cannot get out of quarantine without a PCR-based test). Given the huge percentage of false negatives (no virus on swab in infected, but not grossly symptomatic person) and false positives (amplified fragments of dead virus from months-old infection) that come out of PCR machines, it is unclear why we love PCR so much, but we do! (even if we would have to hate, shun, and cancel the inventor: https://en.wikipedia.org/wiki/Kary_Mullis )
Interesting – now it is a password protected page….
LOL, but you can click on the header “test info” and get in….
Sorry, I was imagining a different process. Recently I wanted to get a standard lab test. In order for the lab (a big national chain) to perform the test, they needed a letter from a physician. To extract the letter from a physician took some effort. I was imagining the “referral” you mentioned required personally contacting an actual physician and extracting a document from them beforehand. That is the normal scenario for health care “referrals” in my experience.
Patrick: It is definitely more streamlined than that, which is why it can be as cheap as $5/test when thousands or tens of thousands of tests are ordered (from the lab: “To cover the physician who provides the legally-required referral, the clinician to oversee the test, the software for ordering and reviewing results, and logistics support. This fee ranges considerably based on the components required, and range from $5-$35.”).
Note that the “instant” at-home test that Mememe references above requires “One telehealth professional consult”. By “professional” I’m going to assume it is someone with at least some sort of state license.
So.. I think they are still going through all of the motions and bureaucratic steps that occurred when you got your “standard lab test.” But the reviews are perfunctory and the paperwork is flying faster.
“Many sites may also require pre-screening, a referral and/or an appointment.”
https://www.mass.gov/info-details/about-covid-19-testing#where-can-i-get-a-test?-
Maybe that language from the commercial provider was just something they stuck in to rationalize their high prices?
Patrick: A plain reading of the law makes it illegal to do a test without a licensed professional’s order. See M.G.L. c. 111D, section 8 (7) ( https://malegislature.gov/Laws/GeneralLaws/PartI/TitleXVI/Chapter111D/Section8 )
A clinical laboratory shall not: … to examine any specimen derived from a human body except upon the written request of a licensed physician … report an examination of any specimen derived from a human body except to or as directed by the licensed physician
COVID-19 is an existential threat to humanity and constitutes an “emergency” that requires the suspension of the Constitution and the closure of schools (at least for Black children who live in the city). But the emergency is not so severe that we can relax M.G.L. c. 111D, section 8 (7)…
https://www.mass.gov/doc/covid-19-testing-ordering-and-resulting-guidance/download
RECOMMENDATIONS FOR COVID-19 TEST ORDERING:
The Department of Public Health recommends that, when possible, providers for testing sites available to the public use a single clinician to order all COVID-19 tests administered at a given testing site. This is
recommended for the purposes of easing administrative burden for the testing site provider, as well as allowing for more streamlined laboratory processing and resulting. Testing site providers are advised to
have one standing order for all patients who are tested for COVID-19 at their testing site(s)
Seems like a fairly minimal requirement?
Minimal requirement? Well, if you’ve ever tried to get an appointment for a checkup with a primary care doctor here in Maskachusetts (most primary care docs won’t even accept new patients and it also typically takes months to get a non-urgent appointment with one’s own), you will be able to answer your own question regarding why not every CVS is a testing site (since that “single clinician” is not going to be easy for CVS to find unless they want to start their own medical school).
@philg “since that “single clinician” is not going to be easy for CVS to find unless they want to start their own medical school).”
For some reason I would imagine that CVS or any other commercial lab would probably have ongoing relationships with outside clinicians, if they don’t employ any in-house? So if they need a letter to cover a new site, they don’t need to establish a new relationship with a new clinician each time? And if the lab is sizable at all, they might be throwing said clinicians a fair amount of regular business, even in the normal course of affairs, and perhaps receive a higher level of service than a private individual? Or maybe I’m wrong? Maybe a CVS employee is tasked with searching for a new clinician from scratch each time they want to initiate testing at a new location, they make appointments just like private individuals, etc.?
Patrick: If you can find licensed clinicians with a lot of extra time on their hands who are happy to work for minimal $$ to order 240 million tests (this is probably the easiest part since I think they can issue a “standing order”), supervise the operation, sign off on the results, explain unusual results to patients who ask, be liable in case anything goes wrong, etc., then you’re right that this is an insignificant barrier to expanding testing.
One issue is that U.S. clinicians don’t have a lot of extra time. We have 2.6 docs per 1,000 people, for example, while Germany and Switzerland have 4.2.
https://www.indexmundi.com/facts/indicators/SH.MED.PHYS.ZS/rankings
“RECOMMENDATIONS FOR COVID-19 TEST RESULTING:
COVID-19 testing providers should always follow their clinical judgement regarding the most appropriate way to contact and relay test results to their patients. Quickly communicating results of COVID-19
laboratory tests is a critical part of reducing the spread of the disease and is a required part of providing testing services. It is not appropriate to direct patients to contact the state or local health department for their results. The following recommendation outline best practices for communicating test results with patients.
Positive test results: All individuals whose COVID-19 test results are positive must be contacted by a clinician and provided with clear instructions to self-isolate. ”
https://www.mass.gov/doc/covid-19-testing-ordering-and-resulting-guidance/download
The document goes on to give more details for positive results finishing with:
“Patients should be directed to contact their primary care provider or medical home for additional medical advice and follow up.”
Dealing with positive results does seem like an expensive part of operating a testing site.
Patrick: Yes, that’s a good point. With more than 20 million lab-confirmed “cases” of COVID-19 so far in the U.S., and assuming Maskachusetts law is representative, that’s a lot of phone calls that can’t be offloaded to the kind folks in India who call me every day offering to lower my credit card interest rates!
@philg Does the Dept of Public Health Guidance look inconsistent with the law you cited? Is Mass DPH is abetting an illegal testing regime?
Is the Dept of Public Health telling labs that they need a (scarce) licensed clinician to order tests inconsistent with the law that says a lab needs a (scarce) licensed clinician to order tests?
If the Dept. of Public Health said that Dr. Jill Biden could be the clinician I might start to get concerned…
Not meaning to derail Patrick and Phil’s conversation here, but…
> let me note that rich white people seem to be ignoring the travel order
Here in a very well-off Bay Area city, this is completely true. In just the last week, here’s a selection of what I’ve heard wealthy white people say:
– I’m heading to Colorado to see my son.
– We’re heading to see family in Los Angeles.
– We’ve decided to live full time in our ski house in North Lake Tahoe until the vaccine has been fully distributed or the snow melts.
– We’re going to Santa Cruz for a New Year’s Eve party.
These are people who will wear a mask 100% of the time they are outside including driving their car alone or running alone on a fire trail in a park.
There is definitely a feeling out here that masks are the magic protective element, social distancing is much less important, and limiting travel to places with fun or family or friends is not important at all.