This Statista bar chart has been suggesting for months that the all-cause death rate in Sweden for 2020, a year in which the country gave the finger to the deadliest virus within the memory of Humankind, will be lower than the death rate in 2010, an unremarkable year from a disease point of view.
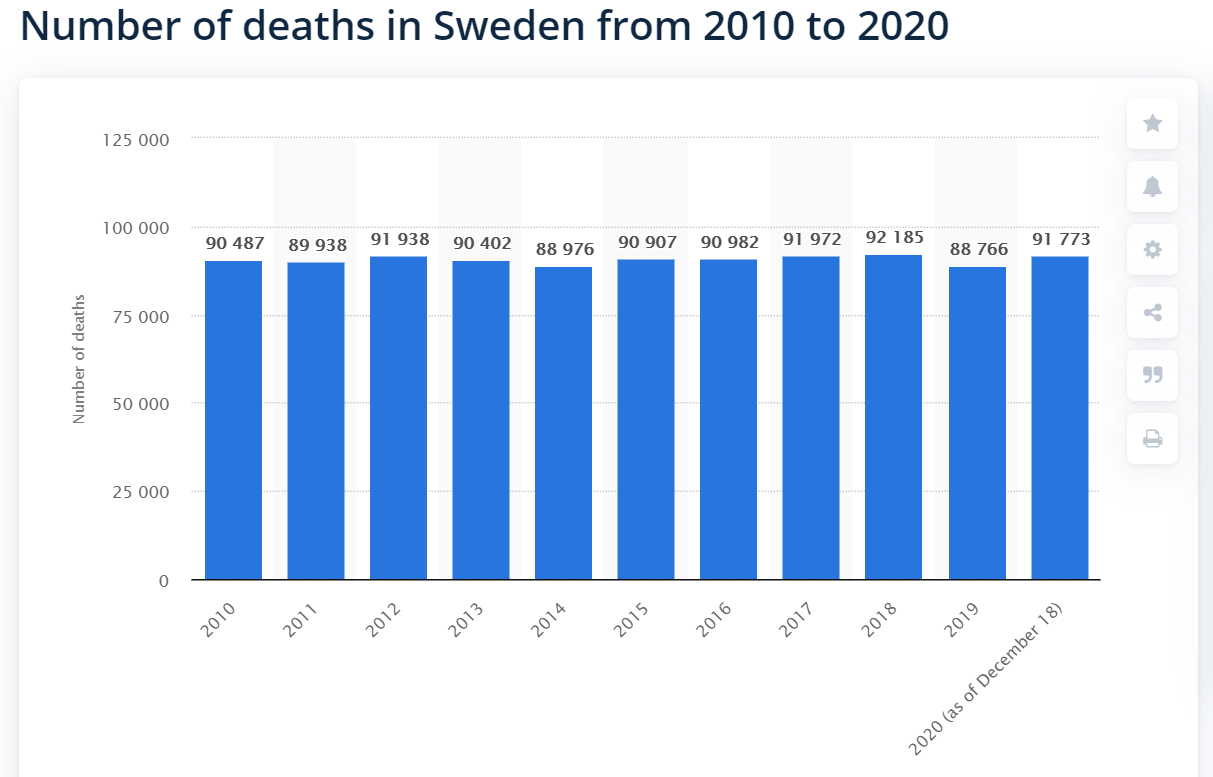
90,487 residents of Sweden died in 2010, when the population was 9.34 million (Google). The population today is 10.4 million (Statistics Sweden, a government agency).
The 2010 death rate applied to the 2020 population would be consistent with approximately 100,750 deaths.
The Statistics Sweden folks make fine-grained death data available for download. The latest iteration, released today, shows 95,022 deaths for all of 2020. However, it seems that the data are incomplete starting on December 21. If we normalize Dec 21-31 with averages from 2015-2019, we would expect Sweden to experience an additional 1,846 deaths in 2020, for a total of 96,868 (i.e., well below the 100,750 who would have died if the 2010 death rate occurred).
[Update: The January 18, 2021 version of the spreadsheet shows 97,941 deaths for all of 2020. More than the above guess, but still occurring at a lower rate than in 2010. It seems that the 2022 versions of the big official spreadsheet describe 98,124 deaths (sum Column G in Table 1), which is still a lower number than the 2010 death rate applied to the 2020 Swedish population size (as noted above, the result would have been 100,750.).]
It will be worth checking back in a couple of weeks for the near-final 2020 number. (The Swedes will publish their final number for 2020 on February 22, 2021, seven weeks after the end of 2020. Their U.S. counterparts at the CDC, published their final numbers for 2018 in January 2020, 13 months after the end of 2018.)
Summary: the Swedes sent their unmasked children to school, sent their unmasked selves to work, sent their unmasked selves to the gym and social events, and generally went right into November before losing their nerve (adopting masks on public transport and cutting “public events” (not private house parties) back to 8 people max). They’ve emerged from what in most countries was the Year of Coronapanic with their psyches, civil liberties (freedom to gather, freedom to travel), education, and work skills intact. They’ve suffered more deaths than in some previous years (but maybe partly this was due to having fewer-than-expected deaths in the most recent years), but have had a lower death rate than they had in 2010 and they’re not even on the first page of countries ranked by COVID-19-tagged death rate.
(What does a moderately northern place with a big city look like when the Church of Shutdown is worshipped and the Ritual of the Mask is observed? The Maskachusetts COVID-19 death rate per 100,000 people is 182 (CDC). Sweden’s rate is 86.)
Separately, for those who are interested in questions of government efficiency, particularly in a declared time of crisis/emergency .. I sent a question to the Statistics Sweden public email address using the World’s Greatest Language (i.e., not Swedish). It was the middle of the night there. I received an English-language answer at 9:47 am Swedish time the next day, also in the world’s greatest language. The answer, from Tova Holm, addressed the apparent discrepancy between the Statista numbers and the spreadsheet numbers (Statista’s chart was correct, but based on an earlier version of the spreadsheet), pointed me to specific sheets within the Excel file, etc.
Readers: If you emailed a U.S. government agency with a random question, how long would you expect to wait before receiving an answer? (Probably not worth asking what would happen if we turned the languages around and queried the U.S. government in Swedish!)
Related:
Phil, why do think more countries are not following the ‘Swedish Model’ (for lack of a better term) for the coronavirus? The only place I know of – and hopefully someone will enlighten me – that follows a similar model is South Dakota. Seems like most of Europe does shutdowns, a lot of Asia (other than maybe Japan, Vietnam) does them, as well as island nations when they have outbreaks. I am not familiar with what most of South America is doing. I am genuinely perplexed.
Paul: I think Florida at the state government level is actually fairly similar to Sweden (protect the elderly in bunkered nursing homes; open the schools for children), but then it turned out that local school districts and teachers’ unions could overrule the governor. The same dynamic played out in Brazil where Jair Bolsonaro told people they wouldn’t be able to escape the virus, but state/local governments tried shutdown anyway.
Island nations and efficient police states can be left out of the analysis since the U.S. has porous land borders and an inefficient government (whether we have a police state is a matter of debate).
I do think it is a matter of priorities and values. If your #1 value is educating children, you keep schools open. If your #2 value is avoiding death from COVID-19 (and you don’t care about deaths caused by shutting down), you shut everything down. A lot of Americans are sufficiently risk-averse at this point that they really should stay in a padded Internet-equipped room for the rest of their lives, so as to avoid infectious disease, transportation accidents, etc. They’re not smarter or dumber than Swedes. They just have different priorities.
A lot of my work-from-home Facebook friends who live in comfortable houses (kids all grown up, but the square footage remains) would, I think, choose 10 additional years of lockdown if it would cut their risk of death by 1%. From their point of view, lockdown has almost no cost and even a very slight benefit makes it rational to choose. (They also convince themselves that it is the interest of young Black Americans living with young kids in apartments. So they’re not only saving themselves, but saving others. It doesn’t strike them as unlikely that a policy designed and imposed by rich white people would be beneficial to low-income Black Americans.)
Presumably it all comes back to politics. A lockdown policy must generate more votes and support from a fearful population than a freedom-first/education-of-children-first policy. There are some regional variations, though. The Europeans are a lot more likely to keep schools open and close down things that adults value (e.g., restaurants). Americans close schools first and keep adult-oriented services open.
“Phil, why do think more countries are not following the ‘Swedish Model’ (for lack of a better term) for the coronavirus”
Because there are 197 countries in the world and the per capita death rate for covid in Sweden puts them at 25. That’s hardly a success story.
Rich: Based on your comment, I think it is safe to assume that protection from COVID-19 death is your #1 priority as a human. You can be a customer for our lifetime-in-a-padded-room concept!
To me, the death rate from all causes, including shutdown-caused death, is a more important statistic than the COVID-19 death rate by itself (and let’s not forget that many shutdown-caused deaths won’t happen for some years down the road, e.g., deaths due to shutdown-induced weight gain, shutdown-induced alcohol and drug dependence, shutdown-induced lack of education (less educated people have shorter lives), etc.).
But most heretically, I wouldn’t evaluate the success of a society by adult death rate! That would be one factor, but a society in which a bunch of people sit in their padded rooms connected to the Internet while the kids play Xbox wouldn’t be ideal under my personal value system.
“Porous borders” is not a valid excuse to eliminate island countries from comparison. Americans are simply incapable of banding together to make one concerted short term sacrifice to effect long term success. We are, after all, a country of contrarians. Naturally, you don’t want to consider New Zealand because they were perhaps the most successful in handling he pandemic. With good leadership and a willing, sane populous, they paid a high price in a very short term and will enjoy fantastic success in the long term. In 2019, we allowed in over a 1.2M persons per day while 2,354 were apprehended between borders. We can’t know how many people crossed our border illegally with success, but presumably those folks aren’t great spreaders of virus. They’re probably laying low and isolating to some extent. It would seem statistically insignificant. Also, almost 44% of all illegal aliens flew in legally and overstayed their visas, which has nothing to do with a porous border, as those folks would be subject to whatever quarantines were mandated to the general traveling population.
SenorP: It is not that undocumented migrants are especially infectious (though the ones ICE catches are 13X more likely to have COVID-19 than the U.S. general population, which itself may include nearly 30 million undocumented migrants; see https://www.americanbar.org/groups/public_interest/immigration/immigration-updates/impact-of-covid-19-on-the-immigration-system/ ). It is that if you successfully “pull a New Zealand” and eradicate the virus from the Lower 48, the virus would show up the next morning in the body of a migrant and the “global pandemic” would start up all over again. That’s where the genius of the New Zealanders in erecting the Southern Ocean border wall comes in. Once the virus is gone, it pretty much stays gone!
philg: Thanks for your reply. I had forgotten about Brazil, and Florida is another great example. Interesting insight on Europe. One possible explanation is government support (ie money) to places like restaurants so while they are closed, they are doing ok economically (like subsidies to our farmers when we put tariffs on items from other countries, they retaliate by not buying crops). Politics and values/priorities, well said.
Senorpablo: “presumably those folks aren’t great spreaders of virus. They’re probably laying low and isolating to some extent. ”
Well, they’re actually probably crammed into an apartment with 20 other people:
https://www.motherjones.com/food/2018/04/farmworkers-are-living-20-to-a-house-in-californias-bountiful-salinas-valley/
https://nymag.com/nymetro/news/features/1869/
From the 2nd article, “According to a recent City Planning Department study, two-thirds of all Mexicans in New York live in overcrowded conditions, the highest percentage of any immigrant group in the city.”
So this is not exactly an ideal situation for avoiding the spread of the plague.
One thing I’ve noticed about the statists: they (at least until this year) want to believe that the kinds of initiatives that work in Sweden would definitely work here, while ignoring the fact that our government is decisively staffed by non-Swedes.
The U.S. enthusiasts for Big Government don’t seem to share Sweden’s enthusiasm for 0% inheritance and 0% estate taxation. Nor for Sweden’s failure to tax offshore or worldwide income!
Philg – you’re cherry picking. Sweden is one of the highest taxed countries in the world. You want all the benefits of socialism without acknowledging the cost.
SenorP: I did indeed “cherry pick” Sweden from among a long list of countries that (a) gave the finger to the virus, and (b) publish timely reliable statistics. Which of the other countries on the list would you prefer to look at? (i.e., a country that did not shut down, that never wore masks except on crowded public transit for the last month of the year, and that offers credible stats right now for all deaths in 2020 as well as in 2010 (“the good old days”))
(Separately, if a society can become immortal via high tax rates, why do Californians sometimes die? And a quibble: Sweden is not a particularly high-tax society for high-achievers. Capital gains rates are lower than in California, for example. Inheritance and estate taxes were abolished in 2004. A high-income person can typically arrange to park income in a corporation domiciled in a no-corporate-tax jurisdiction, such as nearby Estonia, and thus defer taxes for many decades.)
philg – individual capital gains rate for Sweden is still a flat 30%. That 0% rate is for corporate capital gains. Every other rate is significantly higher and their top margins kick in at very modest incomes of 1.5x the national average. Up to 25% VAT. Property taxes are double typical US rates. Social security is about 30% for employers and 7% for employees. Are offshore tax havens practical in Sweden? Do they also have a fascist political party who like to play robin hood for corporations periodically, as with American republicans, which will allow corporations to repatriate foreign sheltered income at greatly reduced rates?
“Property taxes are double typical US rates”
That’s not true. Individual real estate tax there is the lower of SEK 7,812 ($952) and 0.75% of the property’s tax assessment value.
Senorpablo: As with the rest of Europe, the regressive VAT tax is the workhorse in Sweden. So even people of modest means are significant taxpayers and have a motivation to try to control government spending (or at least make sure that government programs benefit ordinary people rather than cronies).
If you check out https://en.wikipedia.org/wiki/International_taxation#Individuals you’ll see that the U.S. is one of only four countries with citizenship-based taxation. Sweden has a more conventional setup. So the concept of a “tax haven” is simply different. The successful Swede who sets up an enterprise based in corporate tax-free Estonia is not engaged in an exotic tax avoidance strategy.
Sweden is a great place to be a billionaire!
Ivan – thanks for the correction on personal property taxes. The rates I quoted were apparently for corporations, which are still quite high compared to the US. Also, there seems to be some additional taxes for real estate in Sweden for which we do not have equivalents in the US. Stamp duty tax applies to property transfers, at a corporate rate of 4.25% and 1.5% of value for personal. Also, a mortgage tax rate of .4-2%. Not trivial up front, but not indefinitely recurring as they are here.
> Readers: If you emailed a U.S. government agency with a random question, how long would you expect to wait before receiving an answer?
I’ll try to find an email contact for the Mass.gov vaccine schedule website and send an email with a nonrandom question tonight about the vaccination schedule. Not U.S. government, the much better MA government.
“The Baker-Polito Administration and the Department of Public Health developed a vaccine distribution timeline after extensive consultation with the Massachusetts Vaccine Advisory Group, made up of leaders from health care, the faith community, community organizations, local government, and others. ”
https://www.mass.gov/info-details/when-can-i-get-the-covid-19-vaccine
They have an email address listed in several places on the page.
Just sent it. I got back a robo-email within 10 seconds, which redirects me to the website and the CDC, including this:
“Thank you for your email.
For information on when and where you can get the vaccine, please visit https://www.mass.gov/info-details/When-can-I-get-the-Covid-19-vaccine for regular updates on the prioritization and distribution timeline. Each Phase and groups within each Phase will be updated weekly and is available on the webpage. Additional clarification and guidance are issued regularly. As we move through the prioritization phases, information on where, when and how to get the vaccine will be posted as it becomes available. Phase 1 is currently underway and Phase 2 is projected to start early March followed by Phase 3 in May. Groups are placed sequentially within each Phase. Please note that we do not maintain a registry to sign up for the vaccine.
For information on diseases or conditions that qualify as a comorbidity, please visit Certain Medical Conditions and Risk for Severe COVID-19 Illness | CDC .
For information on Long Term Care Facilities and the Federal Pharmacy Partnership Program, please visit Long Term Care Facility COVID-19 Vaccine Guidance.
You will also find helpful COVID-19 Vaccine guidance on our website https://www.mass.gov/CovidVaccine including Frequently Asked Questions and updates on the COVID-19 Vaccine Plan.
COVID-19 Vaccine providers will find information about COVID-19 vaccine guidance, prioritization, and trainings at https://www.mass.gov/info-details/covid-19-vaccine-information-for-providers. The webpage is frequently updated with new information.
This email box is being monitored continuously, however, you may not receive a direct response to your question or comment. It is strongly encouraged that you continue to check the website for updated information. For general information about COVID-19 please go to https://www.mass.gov/info-details/covid-19-updates-and-information.
Sincerely,
Immunization Division
Bureau of Infectious Disease and Laboratory Sciences
Massachusetts Department of Public Health
305 South Street, Jamaica Plain, MA 02130
This email box is being monitored continuously, however, you may not receive a direct response to your question or comment. It is strongly encouraged that you continue to check the website for updated information. For general information about COVID-19 please go to https://www.mass.gov/info-details/covid-19-updates-and-information.
I’ll wait and see if I get a direct response. I asked a very specific question and got a robot reply that directs me to the same pages I got the email address from.
I have another comment in moderation with the roboreply from the MA government, so I hope it emerges from moderation because that was fast! But it tells you nothing other than what the website does.
In the meantime, the MA Legislature has voted itself a 6%+ pay-and-perk raise, so let’s hope they’re all getting vaccinated or have a more direct email address.
https://patch.com/massachusetts/medford/s/hdewa/ma-lawmakers-cashing-in-on-pay-raises-to-open-new-year
Alex: OMG, their reply is classic (and hilarious!). Does it pass the Turing Test? 🙂
@Paul B: It sure does pass the Groucho Marx test: “Time flies like an arrow, fruit flies like a banana.”
https://en.wikipedia.org/wiki/Time_flies_like_an_arrow;_fruit_flies_like_a_banana
The saying is sometimes attributed to Groucho Marx, but the earliest attribution to him dates only to 1982,[11] and there is no reason to believe he actually said it.[12]
I think Turing would have found it disturbingly indistinguishable from a human response, because that it just repeats everything so blatantly and there’s really no new information there. I can only wonder what John von Neumann would have had to say. Lol.
@Alex: I wonder what John von Neumann would think of the customer ‘service’ chat bots today..
@Paul B: What’s I find particularly disturbing – and is increasingly prevalent – is that with only a little imagination, one can very easily read this in the voice of a cutscene from an FPS like Doom 2016, et. al. You walk up to a glowing workstation in the room strewn with blood and gore after vanquishing an army of demons, hit [E] and it says:
“Thank you for your interest in the Massachusetts Lazarus Labs vaccination timeline and procedures. Each Phase and groups within each Phase will be updated weekly and is available on the webpage. Additional clarification and guidance are issued regularly. As we move through the prioritization phases, information on where, when and how to get the vaccine will be posted as it becomes available. Phase 1 is currently underway and Phase 2 is projected to start early March followed by Phase 3 in May. Groups are placed sequentially within each Phase. Please note that we do not maintain a registry to sign up for the vaccine.”
Then instructions about how to shut down the portal to Hell by getting to the transport station…
https://www.youtube.com/watch?v=QjzUFlk0eR8
I’m one of those awful people who think von Neumann died far too young and wish he was still around to comment on what the world has made of some of his ideas, or at least have lived another 20 years.
I’m wondering how changes in the age distribution are weighing in. Taking into account that the group with the highest morality rate (the oldest) is significantly smaller in 2020 as in 2010 I’d expect that to have an impact. Plus, the data available is not precise enough to narrow that aspect further down.
Martin, the method the author uses for estimating the non-COVID deaths for 2020 is flawed. As the plots of the author show, the number of deaths in Sweden was almost constant from 1975 to 2019, hovering around 90000. There is no reason to believe that the number of deaths would have “jumped” to 100000 in 2020 without COVID.
The true number of excess deaths is around 7000-8000.
Update: No direct reply yet from the MA Immunization Dept. Going on 24 hours and crickets.
Update Update: I have a medical procedure scheduled with a specialist later this month, the same provider I’ve seen many times in the past six months. Today I called just to verify the appointment was still valid, and thought to ask:
“Also, in light of my [medical condition] and because I have another comorbidity for COVID-19, I’m wondering if you can help me learn more about getting scheduled for a vaccination.”
[Pause on the phone about 10 seconds]
“Um, we are a specialist provider and don’t have anything to do with vaccinations. I think the Massachusetts government has a very strict regimen for scheduling people in hospitals, but we don’t know what it is, so I can’t help you with that.”
“Do you have a recommendation for whom I should call to find out?”
[Long pause]
“I guess maybe your Primary Care doctor? That’s about all the information I have.”
So my specialist had nothing to offer. These are the folks performing surgeries on people with relatively serious medical conditions!
I called my primary care doctor, with whom I have an upcoming telemedicine appointment. Everything possible is being done via remote telemedicine now, and it took an hour on the phone to schedule the 20 minute appointment. After accomplishing that, I asked the scheduling person about my eligibility and timeline for the vaccine based on my health conditions (one of which is fairly severe). Here is what she said, verbatim, reading from the boilerplate prepared statement:
“Right now, we don’t have scheduling in place for the vaccine with patients with comorbidities. [Health Care Provider] is actively working on a COVID-19 vaccination plan and when it is approved we will be administering the vaccine in accordance with the guidelines set forth by the State and the CDC.”
Then they sent me to the provider website vaccine page, which tells you the same thing, and redirects you all the way back to the MA Government website discussed above. Turn Back to Channel One.
So, as of 1/5/2021, my neither my Primary Care Physician, my Specialist Surgeon, nor my larger Health Care Provider System have a plan or a schedule for their patients to receive the vaccine, even people with preexisting conditions and ongoing treatment. It’s all “in the planning stages and we will let you know on the website.”
I’m so glad you have done this analysis of the overall deaths in Sweden. I was in the process of doing the same with the UK.
It looks like the total deaths in the UK for 2020 will be about 580k with a population of 68 million. We had 604k deaths in 2001 with a population of 59 million. If you apply the same percentage to 2020 we would have had nearly 700k deaths.
Regards
Ric
There is a huge flaw in the logic of the author. The death rate of Sweden is around 90,000 yearly since 2000. An increase in population does not automatically lead to an increase in deaths. Hence, Sweden has an excess mortality of 8000 in year 2020.
No offense, but interpreting data should really be left to scholars and not “drive-by” scientists.
Cristian, I find what you said really belittle people ability hold accountable to so called experts lying to people.
Take the so called “excess death” that is being used around the world. It is pure garbage statistics, but we are bombarded with it non stop.
Let look at the US for example, using their official number and accounting for population growth (death/population). Since 2010 there has constant year after year of increase death. But if you used their excess deaths calculation, it would assume a trend reversal ( also ignoring any population change) for no other reason then there has been less death in previous years. Those are the experts that you would have us believe. Similar calculation is being done around the world.
If you think I am making it up, read the information below, collect the official data and do the calculation yourself.
https://www.americanthinker.com/articles/2020/10/covid_problems_cdcs_method_of_estimating_expected_deaths_and_excess_deaths_is_misleading.html
As for PCR testing,.. do you really believe the so call expert claiming that it only detect covid 19. It will surprise you to know that that information is also not totally true. Check out the WHO to see that it is a false claim in their “Diagnostic testing for SARS-CoV-2: Interim guidance 11 September 2020”. They have edit some information out after that date else it would be even more glaringly obvious.
“Since there is currently no known circulation of SARS-CoV-1 globally, a sarbecovirus-specific sequence is also a reasonable target.”
What does that mean? It target “sarbecovirus”. How your sample might contain sarbecovirus is a different topic. That isn’t including all the false positive associated with high cycle.
https://apps.who.int/iris/rest/bitstreams/1302661/retrieve
John, my intention was not to belittle people. However, the author has a major flaw in his method. Many readers didn’t bother checking, took it as face value and agreed with whatever conclusion the author proposed. This is not “holding experts accountable”. This is spreading falsehood. I think the author should update the article and correct the flaw immediately.
As for your other comments, they are off topic for the concern I raised. However, I am concerned that you try to discredit experts, instead of double checking the author’s method of estimating the expected number of excess death.
I understand the methodology that the author used. He was using it to show us how total death count in 2020 isn’t beyond what is consider a normal range by normalising the death and comparing to a year that is consider normal. Maybe you don’t realise the importance of normalisation to perform a more fair comparison.
The only possible flawed is not doing it for a range of years and just picking a year which doesn’t really do the process justice. What is done isn’t spreading falsehood like you think it is. It is the experts that expect general population to be ignorant of basic process of statistical analysis to present a exaggerated situation or present a false narrative.
I am not against expert if they are acting with good intentions for the people and not with an agenda. I am against expert telling blatant lies for whatever agenda. Since covid 19 came on stage, there has been outright lies, proven falsified medical journals, lethal medical studies design to kill people under there care, censorship of different view including hundreds of thousand medical doctors and researchers around the world.
Maybe you aren’t aware of how bad it is or have the impression that there is no way it could be done in such a grand scale. That experts and intellectuals won’t willingly go along with such agenda and exposed it. I been there. Only by reading several dozen medical journals, fact checking and learning history through different eyes did it finally make sense to me. It a personal journey and one not everyone will take, it will take people out of their comfort zone.
Cristian: We can both be correct. I present a 3rd grade division exercise in the original post. Take the number of deaths and divide by the population. That’s the death rate and it is lower than it was in 2010. You are saying that Sweden suffered more deaths in 2020 than it would have if coronavirus had not existed. That can also be true without making the earlier statement false.
From both of these (true) statements individuals still have to decide what to do. Cower in a bunker for a year or two (or 10 years if the virus can evolve its way around our masks and vaccines)? Go out and party? Both could be reasonable choices depending on an individual’s personal value system and preferences.
philg and John,
you propose the “death normalization” model, i.e., that the ratio between the number of deaths in a year and the population is approximately a constant, let’s call this constant alpha. The population in 2010 was 9 408 320 (according to SCB) and the number of deaths was 90 487. Hence, alpha is 9.6177 death per 1000 people. You then take the model and the previously computed constant alpha, to project that the “non-COVID” number of deaths in 2020 (with a population of 10 378 483) would have been 99 817. (Please ignore the small difference in input data, they are not relevant to my argument.) Did I get your model correctly?
If yes, let us apply the same model to 2016-2019 and compare the predicted number of deaths with the deaths in your data:
year | population | predicted | your data
2019 | 10 319 473 | 99 250 | 88 766
2018 | 10 215 309 | 98 248 | 92 185
2017 | 10 104 036 | 97 178 | 91 972
2016 | 9 967 637 | 95 866 | 90 982
As you can see, your postulate consistently predicts a lot more death (between 4 900 and 11 000) for year 2016-2019 than what was measured in reality. For comparison, the model “deaths in Sweden is constant 90 000” gives an error between 1 700 and 2 200. The data simply shows that the “normalized death” model is not accurate: The number of death may be correlated with many variables, but, at least in case of Sweden, for the years 1975-2019, it does not correlate with the population. Hence, deducing that “we should have seen approximately 100,750 deaths” is simply not supported by data.
Let me ask in another way: Why did you normalize deaths with population? Why should one not normalize with population over 60? Or population over 70? There is no a-priori reason to believe that normalization is necessary, and, as I hope I convinced you, the model “deaths need to be normalized with population” is simply inaccurate.
(P.S. Someone off-topic, I do like Sweden’s strategy. They decided to buy sustainable restrictions by sacrificing some elderly life. It is a tough moral and ethical position to take, which certainly benefits some part of the population. But let’s not pretend it was without casualties.)
I should also apologise if what say in any way sound offensive to you Cristian. That wasn’t my intention.
You might say I been trying to keep up with the news and was disheartening to see people not wanting to question experts that could result in harm to themselves.
John,
No need to apologize, I did not feel offended. I hope I managed to disagree with you as respectfully as you disagreed with me.
I do agree with you that we *must* constantly challenge experts. But I also think that we must give them some benefit of doubt before making our own predictions.
Please note that the conversation really has two parts: (a) challenging the experts on the number of excess death in Sweden, (b) challenging the experts on the lockdown measures taken worldwide. I was only meaning to correct (a), which I feel is a question that can be backed by statistics.
(b) is very much a political and ethical question, which has no scientific answer: Should we save as many elderly as possible? Should we let the young population live as normally as possible? Somewhere in between? I think all opinions are valid on (b), but I feel strongly that everyone needs to get (a) right first.
I think you have the wrong impression of the calculation and it purpose. The calculation is not used to predict death or excess death. It purely used to make the number more comparable when comparing different years.
We could normalise it with different age group if we take death in that age group only else we polluted with death in different age group.
So if we are concern with changes in death 60+, we look at death in that age group and then used the population in that age group to normalise the change in that age group.
The usual approach to normalise death between years is to used death per 1000 of the population. Divide death of that year by population of that year then multiply it by 1000. By calculating as such you can then see and compare any year with each other. Nothing about predicting death, but a comparison.
Now let talk about predicted death and expected death.
The general calculation for predicted death is to average out the several previous year death, that number is then the expected death for the year. Excess death is calculated by actual death minus predicted death.
Using the general calculation for excess death, there is no weight difference to any of the given years used. So what occur say 4 year ago and one that occur the previous year affect this year death equally. Which is to say there the calculation assume zero trend or a reversal of then if there is a trend to neutralise trend. Nor does it take in consideration of changes in population. So you see why I say it a flawed method of calculation.
Instead of flawed predicted death/excess. We should be using death rate per 1000’s and comparing it to other year, it can show us if covid 19 has impact (let say Sweden) beyond accepted level of non-pandemic year.
Hope that explain my view for part a.
Oh.. forgot to added, by normalising death to per 1000’s, if you look from year to year in the graph you can see if there is a trend or not. Allowing you to determine the degree of changes match what is to be expected without any expert translating it. Easy to see.
With the expected death/excess death generally used, such information is lost. Even if they plotted the expected death/excess death, it very hard to see anything out of it.
Found a site that illustrates the death per 1000’s for Sweden, they smooth out the curve. It will maybe help you see how the graph can used to easily see the trajectory and you don’t need any expert to explain it to you.
Just remember to change the year so it doesn’t pass 2019.
https://www.macrotrends.net/countries/SWE/sweden/death-rate
If it show you that we should be expecting more or less death for 2020, it will be you who come to that conclusion without me or other people telling you of it.
What you might find interesting if you want to compare how Sweden health policy prior to 2020 vs other countries is by selecting those countries and setting to same period in time. Whatever Sweden been doing, it show it has been for the benefit of the people unlike majority of other countries.
John,
I just checked the website you sent. The death per 1000 in Sweden was 11.185 in 1988. Since then, it decreased every year until it reached 9.165 death per 1000 in 2019. In contrast, philg assumes that the number of deaths per 1000 is constant and equal to around 9.688, which it is obviously not according to the website you sent me. This downward trend is completely ignored in philg calculation, which exaggerates the predicted (non-COVID) death for 2020.
Normalizing death to the population for comparing different countries makes sense. Normalizing death for comparing year-by-year trends within the same country does not always makes sense.
Let me give you a non-expert argumentation: The absolute number of death in Sweden was under 92 200 for all years 2010-2019. Why would one predict the number of non-COVID deaths to suddenly jump over 100 000?
Again, the calculation ignores the downward trend in deaths per population for Sweden (or alternatively, the lack of trend of non-normalized deaths). This is a major flaw, which leads to misleading predictions.
Oh, I should say I do not reside in Sweden. Hence why I dislike the experts, politicians and media which constantly lied to it people. Throughout the whole period 2020, they have called Sweden a failed experiment, that is killing it people and make it seem like it’s a death trap. While the reverse the more likely situation. Making false allegations and taking quotes out of context. With continual bombardment of such narrative most here never question it and believed it is all true. With border closed, lockdown, masked, social distancing & no freedom to assembly at one stage or another there is lack of unbiased information here. Hope that explains the type of experts I dislike so much.
I personally admired Anders Tegnell and what he has done in Sweden. It is not his expert I am complaining about. Unfortunately the more recent news I been hearing, it seem those experts I dislike so much has access to unwary ears over there.
As for the site please remember that I did say to goes as far as 2019 and not beyond. 2020+ is pure simulation and any time frame beyond that.
The graph does smooth out the curve, a lot more then I would like. It more to show you how easy it it to read such graph once you do the calculation.
Whoops, accidentally click on wrong reply.. I’ll just copy it here.
As for why you used the graph within one country is if you see the curve for example been going up, if you were to make an educated guess on the next point on the graph it would be up because you think the trend should continue.
But based on the flawed general expected death calculation used, it would be the reverse since it averaged out the lower count.
Heres a fictional death count to illustrate it with simple number we can do in our head.
2015 100 death
2016 200 death
2017 300 death
2018 400 death
2019 500 death
If you look at the table or graph you would naturally expect 2020 to be 600 death.. but base on the flawed expected death calculation it would expect death to be 300 for 2020 by average out the death between 2015-2019.
If actual death was say, 400 for 2020, you would say that lower then expectation. While using the flawed expected death it would claim there is 100 excess death.
Both the death per 1000’s and the flawed general expected death does not take in any real life change such as covid 19. While with the death per 1000’s you can more less say if the actual figure show if it has impacted death for 2020 visually.
Btw the flawed expected death is used by the CDC and many other countries including mine. Haven’t check with Sweden is that the one you are given or if you have more reliable people who will do further analysis to it prior to presenting you with such info.
John,
I get your method, but that is not what the data shows. The data is more like:
2015 900 death
2016 900 death
2017 900 death
2018 900 death
2019 900 death
For 2020, I would expect 900 and certainly not 1100. 🙂
Other than that, I do get your distrust in experts. I’m afraid, however, that it’s not entirely their fault. Experts are good at predicting things like “if this than that”. Like “if you lock down, the infection rate will go down” or “if you don’t lock down, the infection rate will continue to rise”. Unfortunately, experts were asked, under intense political pressure “what should we do?”. (See Sabine’s criticism on “Follow the Science? Bullshit I say”: https://www.youtube.com/watch?v=nGVIJSW0Y3k&ab_channel=SabineHossenfelder)
This question simply does not have a scientific answer, rather it boils down to ethics: Do you want to safe elderly or make life bearable for the younger generation?
I do live in Sweden and I think it’s awesome how Tegnell managed to keep his cool given the extreme pressure he was getting. I actually followed one of his press releases. You could tell that he first looked at data, then produced recommendations.
Nevertheless, even Sweden is divided: Personally, I switched from malls, gyms, pools and cinema to nature, super easy! My neighbor, a nurse, had to work during Christmas and New Years.
So the whole pandemic is not about what is good and what is bad, rather which group of people do we protect and which group of people do we ruin.
Oh… and once the finalise death for 2020 is reveal for Sweden, on the death per 1000, if you draw a horizontal line at that death rate, any year that fall below the line you have less comparable death then 2020. Any year above that line you have more.
If it on table form, just look for all the number above and below the 2020 death rate.
Once you grasp the concept of normalise value, you will notice many statistical analysis using it in different ways all the time. From medical, research, economic, engineering, financial, social studies and etc.
I think the initial issue was the assumption that normalising of data equate in correlation between population change and death. Instead it was the removal of the variable of population change to view things in more comparable light.
I’ll be sleeping and if you think or believe I am wrong. Don’t mind saying so, I for one know I am not perfect and see it as a growth if I learn something new.
Yes, the graph for Sweden does show it and I agree. If I disagree with it I would be a fool who ignore unbiased statistics. You can also see that total death exceeds some non-pandemic year (especially those recent years) and looking further back, it is below other years using comparable value. The further you look back, the less association it has on current year which is true.
I hope you can agree that the author action of normalising death will allow us to compare it to the past. There is more death in 2020 then recent years, most likely due to covid 19, but should the death make us live in fear if it comparable to some non-pandemic years? To make it evident base, calculation needed to be done to show such thing is the case. Why pick 2010, I can’t say for sure, it still show such evident. Hopefully you can see there was nothing glaringly wrong by normalising death.
I understand what you are saying about Sabine’s criticism. The interpretation of science and what should we do or does it really matter to us that much?Calling it bullshit is logical assuming the science is base of fact and not propaganda. I would really prefer that my concerns was similar.
Unfortunately what I am talking about it worse in my countries and many other. I am talking out intentionally distorting science facts to further an agenda.
You might consider this off-topic, but let me talk about the science that I have to deal with in my country and many other are in the same boat.
Like it is shown that HCQ, ivermectin (replace his with other similar drug) & zinc work against covid 19. To disprove HCQ effectiveness, they released fake medical articles with the conclusion that it increase death for those with covid 19. Then when they perform actual medical trials, they overdosing critically ill people with HCQ at potential lethal dose to prove that HCQ lead to death to those with covid 19. Naturally they never mentioned correct dose level and claim those they used were in line with modelling to ensure it efficacy. The efficacy amount was pure rubbish.
Luckily in Sweden the only time it was banned was when the fake medical articles was published, the banned was remove once it was known it was fake. Other part of the world, the banned never got lifted, instead they double down, claiming HCQ doesn’t not working at all and it irresponsible to say it does and we need to get over it.
Or how they wish to say mask is effective, creating scientific paper using antidotal situations and conclude mask might work, to test such postulation, we need to perform mask mandate at countries wide scale. From then on, only thing they say it is scientific facts that mask work and any who denied it is anti-science.
Anders Tegnell got it correct when he say the evidence of mask effectiveness is astoundingly weak, but where I am, they claim it an iron clad certainty. Pointing at Anders Tegnell and claiming him to be well… ignorance. Took 4 years to complete a one year course through distance learning, attacking his character.
But not everywhere there is a graph like Sweden for death rate. The graph in prior years, majority of other countries is nothing like Sweden. They are using the flawed excess death figure to further action that cause more suffering and amplified fear.
Experts like those are rampant, while censorship of proper experts was done.
This is the type of result of the science the majority of the world got to deal with.
https://buffalonews.com/news/local/after-judge-orders-hospital-to-use-experimental-covid-19-treatment-woman-recovers/article_a9eb315c-5694-11eb-aac5-53b541448755.html
Oh… and this is the type of experts, police and media we also have to deal with. Not old news.
https://healthimpactnews.com/2021/community-bands-together-to-rescue-elderly-woman-medically-kidnapped-the-life-of-a-senior-is-still-precious-to-some/
Once you allow those experts, they will gain the support of the majority of the population. They will drive them to unquestioned irrational fear and people will let them and support them, thinking by doing so we will get back a portion normality as the expert claim.
John,
The concens you raise are worrying. However, the answer to FUD (fear, uncertainty, disorder) should never be to counter with a flawed method “just to reassure”. I mean look at all the comments! Nobody bothered running the numbers and everyone just took “Sweden is doing great” as a fact. The author does not seem to care correcting the article either.
At least 7,500 people died in Sweden due to COVID. We can debate if the measures were sufficient or not, we can debate if other countries should follow the Swedish model, but we cannot debate basic facts about the excess deaths in Sweden in 2020.
I think you are seeing that the process wasn’t apply to all years or one that is closer to 2020. Thus the comparison wasn’t fair. If the author extend the graph from 2000 to 2020 and let people decide for themselves if they should enjoy life or remain fearful of covid you would be more accepting of this method?
No one is debating there was more death in 2020 in Sweden then what it was trending to. The numbers I used was just to show and compare method using fictional numbers to see how the usual way of calculation excess death can be misleading and how the process I mention can be used to get a better excess death estimation (that is, a usage fo death per 1000s when comparing it to numbers just from Sweden and no with other countries).
I don’t think Sweden approach is the best either, its been extremely good without knowing the future. But what I trying to say, is Sweden has in the past done what it think is right base on actual science it has at the time. What I am concerned about is that in the future it may not be so.
I am using what has occurred in other parts of the world to illustrate this. I don’t think France US, UK and etc would have expected the distorting of science would ever occur to them. I just want people everywhere to be wary and have a inquiring mind or accept other questioning and verified truth.
John: I used 2010 because that is as far back as the chart goes. So 2010 is “the good old days” from the perspective of someone looking at the chart. If the chart started at 2000, I would have started at 2000.
John,
Yes, the author very clearly debates whether Sweden had excess mortality or not in 2020. I’m quoting the relevant part here: “we would expect Sweden to experience an additional 1,846 deaths in 2020, for a total of 96,868 (i.e., well below the 100,750 who would have died if the 2010 death rate occurred).”
Compare that to the better informed way of estimating excess mortality (quote taken from the Swedish National Television): “Statistics Sweden (SCB) has concluded that 97,164 Swedes died last year. This should be compared with the years 2015–2019, when an average of 90,962 people died each year. In other words, 6,202 more Swedes died in 2020 compared with the average.” (https://www.svt.se/nyheter/inrikes/coronans-verkliga-dodstal-borjar-bli-synligt-1)
Everyone has the right to debate whether they want to live their life in fear or not. But debating how to estimate excess mortality should be reserved to those mastering statistics and trend analysis.
Thank for explain why you selected 2010. Maybe to keep it less bias, have a chart of death per 1000s from 2010-2020 in there too once the figure for 2020 is finalised.
I am one who like everyone to live their life however they wish. Covid 19 isn’t what scaring me. It what happening in the name of combating covid 19 and the experimental vaccine that scare me make me cry sometime. With very effective treatment and procedure designed already its painful to see death continue to rising and the push for the experimental vaccine.
Yes, since first published https://www.statista.com/statistics/525353/sweden-number-of-deaths/ was updated and shows 97,941 deaths of Sweden for all of 2021. Every death is a tragedy but extra over 6000 of deaths for 10,000,000 of population is much lower toll than deaths in masked and locked state of New Jersey that has over 20,000 coronavirus deaths with less than 9,000,000 of population, if statistics is to be believed. Did not find annual deaths statistics for NJ, maybe they too would show a significantly smaller bump then 20,000 would suggest.
“Low skilled immigrant” (funny name 😁), yes, that is the proper way to frame the issue!
Sorry to hear about NJ. I would assume that Sweden has the huge advantage that it is rather sparsely populated, so social distancing was potentially easier than in large metropolitan areas.
When coronaplague rates are low in a masked-and-shut place, we ascribe that to the masking and shutdown. When rates become high we say that it was unavoidable due to population density or other factors beyond human control. (See https://www.statista.com/statistics/1109011/coronavirus-covid19-death-rates-us-by-state/ for how the sparsely populated desert states of AZ and NM did not escape, though). Sweden’s middling numbers are plainly the result of human folly in giving the finger to the virus and continuing to send children to school.
If coronaplague truly is just about population divided by land area, that proves that Donald Trump was truly the wisest leader during this panic. He tried to purchase Greenland, which would have dramatically lowered Eastern U.S. population density.
True, 40% of Sweden’s population is concentrated in 3 metropolitan areas.
The world is full of narrative, with many contradictory one explaining why covid 19 spread and kill different in one place vs another. Look at japan with low death rate and they explain it because of face mask. How the flu was practically eradicated due to face mask, but people keep on spreading covid because we aren’t wearing face mask.
What does “we are all in it together” really mean?
Put simply, it mostly propaganda design so politicians and other people can pick which one suit make sense for their agenda.
Why are we trying to explain things base on what we got told without evidence but base on correlation because it common sense? Like in the link about medical kidnapping I posted, the narrative of the media explains thing in such logical reason but completely fabricated if the video footage is to be believed.
Was the proven falsified medical articles in the top medical journals just an isolated cases? Or is there a more fundamental issue with our medical industry that was design over many years? Where it not just the ease in which such task can be done, but systematic corruption of personnel in very high positions. Maybe there is some truth in “ghost managed medicine” (it a free ebook I found interesting).
As for why you used the graph within one country is if you see the curve for example been going up, if you were to make an educated guess on the next point on the graph it would be up because you think the trend should continue.
But based on the flawed general expected death calculation used, it would be the reverse since it averaged out the lower count.
Heres a fictional death count to illustrate it with simple number we can do in our head.
2015 100 death
2016 200 death
2017 300 death
2018 400 death
2019 500 death
If you look at the table or graph you would naturally expect 2020 to be 600 death.. but base on the flawed expected death calculation it would expect death to be 300 for 2020 by average out the death between 2015-2019.
If actual death was say, 400 for 2020, you would say that lower then expectation. While using the flawed expected death it would claim there is 100 excess death.
Both the death per 1000’s and the flawed general expected death does not take in any real life change such as covid 19. While with the death per 1000’s you can more less say if the actual figure show if it has impacted death for 2020 visually.