Continuing to explore a topic raised in February (Did vaccines or any other intervention slow down COVID?)…
Cochrane has shown that the correlation between forced masking and coronaplague is minimal (i.e., general public masking does not reduce the spread of a respiratory virus, just as Science, including the WHO, said for 100 years prior to June 2020). We’ve had a good natural experiment on COVID-19 vaccines in that countries vary dramatically in their vaccination rate. Where is the study that shows, from these data, that population-wide COVID-19 vaccination, as aggressively promoted by the CDC (down to age 6 months!), reduces COVID-tagged death rate?
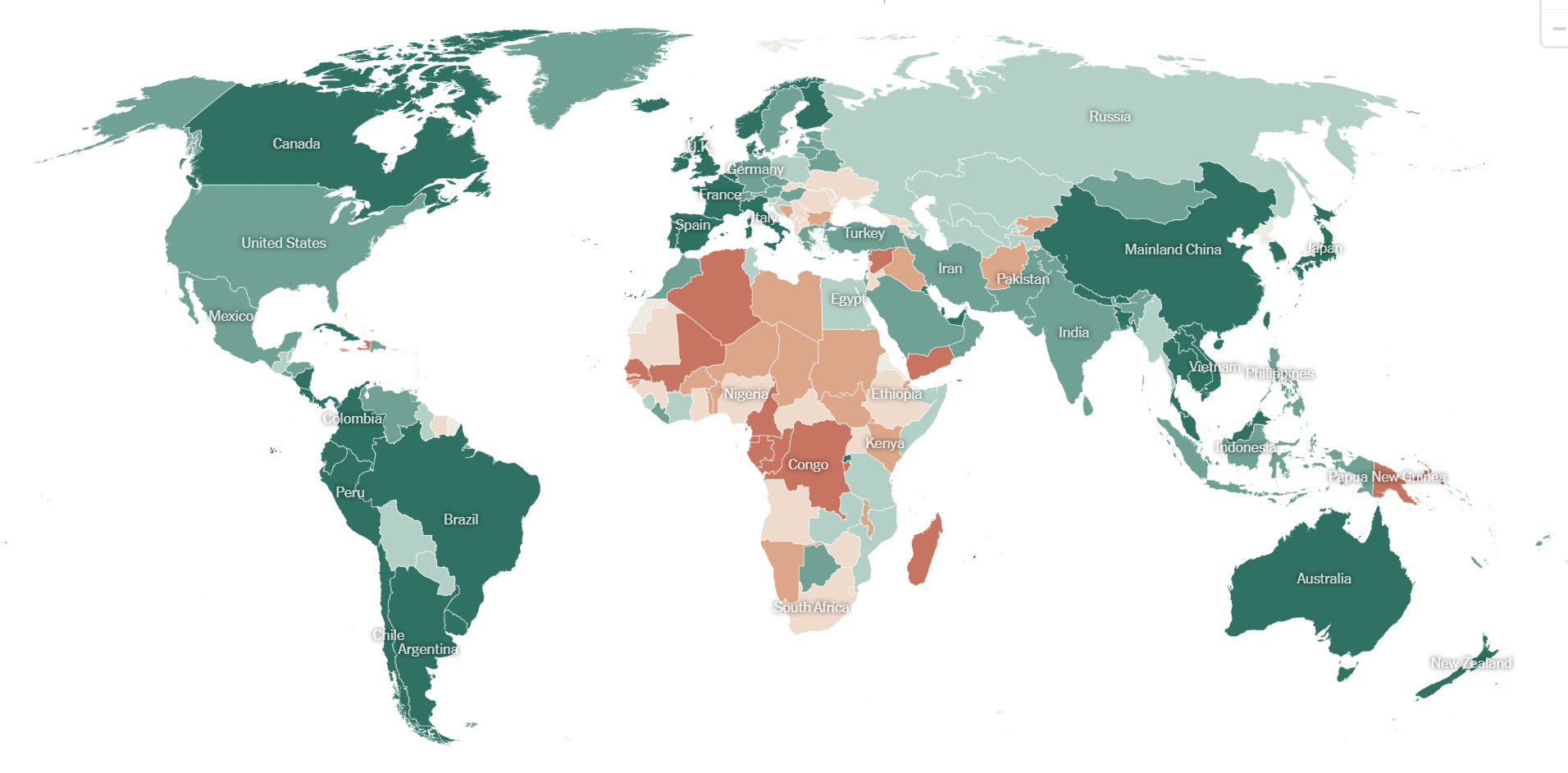
The New York Times offers a map and table of countries and their “fully vaccinated” rate. We can see that Chile is 93% fully vaccinated and Spain is virtuously at 87%. Compare to just 34% in Ukraine and 30% in Nigeria.
The correct approach to an analysis would almost certainly include adjusting by share of population over whatever we can agree is the COVID-vulnerable age (CDC says 6 months; European public health officials say 50 (age of vaccine eligibility); previous attempts have used 65; median age of a COVID death is about 80). But what if we do a rough cut by looking at the raw (not age-adjusted) COVID-tagged death rates?
| Country | Vaccination Rate | Covid-tagged deaths/million |
| Chile | 93% | 3,080 |
| Spain | 87% | 2,301 |
| Switzerland | 70% | 1,603 |
| Turkey | 64% | 1,175 |
| Ukraine | 34% | 2,565 |
| Nigeria | 30% | 15(!) |
Is it obvious from the above that #VaccinesSave?
(We could also look at excess deaths by country during three years of coronapanic. Vaccinated Chile is at 18%; Spain at 11%; packed-with-filthy-unvaccinated-disgusting-people Switzerland at 8% (no data for Turkey, Ukraine, and Nigeria).)
Why does this matter? Let’s look at a post-Cochrane tweet from a person who might be described as a moderate believer in public health interventions. With her MD and MPH, certainly, she cannot just throw in the towel on the idea that humans, at least with sufficient credentials, can be masters of their own destiny. In light of the Cochrane review, she says that we will master our destiny with vaccines and Paxlovid:
But if the Followers of Science fooled themselves for 3 years on masks, why can’t the Followers of Science also be wrong about the effectiveness of vaccines and Paxlovid? Is it worth looking at age-adjusted country-to-country comparisons to make sure that we aren’t wasting a lot of time, energy, and money that could be better spent on, e.g., fighting obesity (first step under Philip’s dictatorship: no more Buy 2 Get 3 candy sales at CVS!)?
Fighting COVID with ineffective tools is not cost-free because humans have limited time, energy, and money. Closing schools, for example, will ultimately cost more lives than SARS-CoV-2 infection because people with less education live statistically shorter lives. Dollars printed to pay people to sit at home for 2 years are dollars that can’t be used to pay people to lose weight (imagine what you could do for public health if you gave Americans $600/week on condition that they lose 1 lb. per week! (maybe people would game the system by bulking up in the week prior to the first weigh-in?)).
(Speaking of Paxlovid, my friends in California seem to be Pfizer’s best customers. They said that they would never get COVID because (a) they had 4 or 5 Pfizer shots, (b) they mostly stayed home for 2+ years, and (c) they wore their N95 masks on the rare occasions when they left home. Then they got COVID (once or twice) and, despite being reasonably young (60ish) and not obese or chronically sick, they would guzzle Paxlovid within hours of an at-home test yielding the sacred magenta line. (How did they get it so fast when the rest of us have to wait 2 months to see a primary care doc? Telehealth!))
What do you make of this data/graph?
https://twitter.com/PaulMainwood/status/1629229862685753347?s=20
I think it is better to look country to country because then all types of people are included in the stats. The problem with comparing vaccinated versus unvaccinated populations within a country is that these populations have a lot of other differences. It is not a randomized controlled trial. A work-from-home laptop class member is more likely than average to be vaccinated, for example.
When comparing countries the main adjustment required is for age distribution (unless you believe the CDC and American universities regarding the high vulnerability of slender 18-year-olds to death-by-Covid).
Also, don’t forget the biases of the academics reporting on the filthy unvaccinated Deplorables within the US.
See https://www.nas.org/blogs/article/partisan-registration-and-contributions-of-faculty-in-flagship-colleges for the political diversity at institutions that say diversity is their #1 goal.
The data without understanding underlying methodology is meaningless. In this case methodology (is there mention of C19 on official death report?) is total and utter junk. It is vulnerable to both administrative shenanigans and to honest diagnostic bias by physicians (this geriatric patient died from some respiratory infection, he has been vaccinated… no, that cannot be COVID).
Well indeed these statistics are not completely satisfactory, but neither are those broad cross country comparisons due to possible selection bias. But with ratios as strong as 10 to 1 regarding the deathrate, what would a guess in the spirit of Occam’s Razor look like here? If it is not the positive effect of the vaccination, it would also have to explain why the death rates of these groups suddenly converges again after the emergence of milder variants… So it cant be the generally poor health of those deplorables.. Or is the official British data just wrong..?
Uncle M: The death rate for any virus goes down after a season or two because a human vulnerable to a virus cannot be killed twice. Once most of those susceptible to death from SARS-CoV-2 have died, the death rate will fall even if there are no changes to the virus, no effective vaccines, and no improvements in therapy.
Actually it’s not only because of deaths of susceptible. People who had infections but survived develop natural immunity (which, due to diversity of learning by immune system is strictrly better than targeted learning induced by non live-virus vaccines) which either prevents or reduces severity of sibsequent infections.
@philg: So your take on the death statistics is not that the vaccines are effective, but the selection bias is so strong that on average the people declining the vaccine had somehow 10 times the risk of dying compared to the vaccinated population during the delta wave? And supposedly the reason for there demise is indeed corona, because after that wave has passed the death rate declined again?
Uncle M: That’s a good question. The US does not have a national medical record system so it impossible to do high quality research on this subject here (there is, for example, no way to know for certain what shots a particular human has received). The UK has some good data, but I haven’t looked at the latest report (see https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/deathsinvolvingcovid19byvaccinationstatusengland/deathsoccurringbetween1april2021and31december2022 ). They push out a huge spreadsheet and leave it to the reader to look at the relative risks.
But overall I am not offering an explanation for why a country’s vaccination rate and vaccination schedule (very early for Israel, for example, and moderately early for the U.S.) seems not to be correlated with the COVID-tagged death rate. I am mostly noting the lack of correlation.
Try this: https://www.economist.com/graphic-detail/coronavirus-excess-deaths-estimates. Anything other than excess deaths will have reporting bias depending on the country’s definition of a death from covid
excess deaths (or in the case of Japan) the opposite seems to be the best measure of the effect of Covid even if one removes things like (perhaps) fewer traffic deaths, more suicides etc.
https://ourworldindata.org/grapher/cumulative-excess-mortality-p-scores-projected-baseline is my preferred source for excess deaths (and it isn’t paywalled, as the Economist’s map is).
Gary: I tweaked the original post. Using Our World in Data as a source. One challenge with using excess deaths is that stats aren’t available for as many countries.
No one will study the topic until the The Party approves. The Party has now approved the lab leak theory (!), because suddenly China is bad, very bad:
https://www.wsj.com/articles/covid-origin-china-lab-leak-807b7b0a
In 2020 this was a “conspiracy theory”.
MiniTrue should update all previous articles to explain that SARS-CoV-2 leaked from the Wuhan Institute of Virology’s balloon fleet.
If a country doesn’t have good excess death numbers, I wouldn’t trust any numbers coming out of them.
The problem with looking at excess deaths is you don’t know if the deaths are from COVID or from the government reactions to COVID.
That’s true. All of the extra opioid overdoses, etc. Most of the lockdown deaths are in the future, though. People who gained weight, drank more, or went to school less during 2-3 years of restrictions will live shorter lives, but they might not actually die until 40 or 50 years from now. An 82-year-old whose life was shortened by two weeks by SARS-CoV-2 is marked down as a “COVID death” so a 10-year-old who lose a year of school in Boston or Chicago should also be considered a “COVID death” when he/she/ze/they dies a few weeks earlier than if his/her/zir/their school hadn’t been closed.
I don’t think the raw COVID death rates are all that inaccurate. Maybe they could be off by a factor of 2 in either direction? Sweden had one of the most comprehensive and automated systems. Test positive within 30 days prior to death and you were a COVID death by default in their nationwide computer system.
The C19 tests are total and utter junk. Does anyone know the actual false positive rate of these tests?
…that’s the point. Nobody actually knows. Because it is not published and likely has never been measured for any of the common brands. The validation required by FDA only demonstrates that FP is within 0%-11% (95% confidence interval).
The COVID epidemic could actually be mostly flu plus faulty testing. Notice that diagnosis of influenza virtually disappeared in late 2020?
To make things even funnier it hasn’t been established that SARS2 virus actually causes COVID. Not to the normal standards of proof (Koch postulates, or their modern variants).
The whole mess is piss-poor (if not outright junk) science and cojecture masquerading as actual sciemce. The outputs of it: “safe and effective” vaccines and treatments which already likely killed more people than saved and ridiculously, orders of magnitude, wrong epidemiological forecasts are quite telling. Quackery at its finest.
Just face it: biomed research in the West is a fucking joke. (Per Prof. Ioannides famous study, up to 80% of published biomed papers are junk science, non-reproducible, or of such low quality so as to be meaningless).
For age adjustment you have to allow for x10 or so increased vulnerability per decade of old age, which is such a large factor that conclusive and convincing results could be difficult to come by unless the analysis focuses on lower age cohorts where the exponential is flatter.
Cochrane in conclusion says the studies are too weak to draw strong conclusions. Lack of evidence is not evidence of lack.
Gill: Let’s apply your reasoning to snow in Palm Beach County. It hasn’t snowed in the past few years, which I attribute to the fact that at least one person out of the 1.5 million residents is wearing an “Ask Me About My Pronouns” T-shirt on any given day. https://amzn.to/3EJvO6y God controls the weather and God is trans, according to a rabbi selected by the New York Times (see https://www.nytimes.com/2016/08/13/opinion/is-god-transgender.html ). Therefore, God is happy when He/She/Ze/They sees the shirt and blesses us with warm sunny weather.
I have held this belief since March 2020.
Cochrane cannot find any correlation between this T-shirt being worn and God smiling on Palm Beach County and refraining from smiting us with snow. However, that doesn’t mean that the “Ask me about my pronouns” T -shirt isn’t effective at preventing snow.
Philip — It doesn’t make sense to compare deaths vs vaccine rates in these countries because most deaths happened before the vaccines!
Look at Chile, for example:
Daily deaths were high until around July 1, 2021, at which point they started dropping rapidly:
https://www.worldometers.info/coronavirus/country/chile/
When did Chile hit 50% vaccinated with 2 shots?
https://www.statista.com/statistics/1257346/population-vaccinated-against-covid-19-chile/
June 22, 2021!
It’s almost as if these two things are related.
That’s a great theory to explain one country’s data. Now let’s use your same site to look at the US. The slope of the death curve flattens in March 2022. What did intelligent humans in the U.S. do in March 2022 to defeat the stupid virus? https://www.worldometers.info/coronavirus/country/us/
Philip — The Jan 2022 flattening is easy to explain, although there are 2 factors are play
– Omicron was far more contagious, and most of the country caught it within the course of a month. After that, there were simply not many people to infect.
See: https://biobot.io/data/
You can likely recall a short 2-week period in Florida around Jan of 2022 where everyone had it.
– All variants from Omicron on have been less lethal.
So once Omicron passed through, you had: fewer new infections, fresh natural immunity, and a lower chance of death from each infection.
“natural immunity”? Science says that natural immunity is of insignificant value compared to the Sacrament of Fauci. https://www.nytimes.com/2022/02/03/well/live/booster-after-covid.html (February 2022): “Most experts agree that vaccines can offer a more reliable and effective immune boost than a natural infection can.”
Saying vaccines are better than natural immunity isn’t saying natural immunity doesn’t help a lot. But all this is old news and turns out to be probably wrong for two shots (but not for a third bivalent shot)
Why? because ,the new lancet paper is pretty definitive, natural immunity is at least as good as two shots. Although the data is less clear for a third bivalent booster or a bivalent booster for someone with natural immunity, the evidence is actually pretty good for this being far superior for high risk people. So the current best evidence which all people at high risk should follow is:
Natural immunity >= two shots
Bivalent + two shots > natural immunity.
If you are at low risk, there isn’t enough evidence to draw a good conclusion but having a good evidence based conclusion isn’t as important for these people..
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(22)02465-5/fulltext
Gary: If “experts agree”, as the NYT says, that’s a “scientific consensus” and it is therefore incontrovertible (unlike the mass of the hydrogen atom, about which research can still be done). So I’m not going to commit the heresy of doing my own research and I will accept the Science that natural immunity is near-worthless compared to the total protection of the Pfizer shots.
In that NYTimes article, pay attention to this part in the next paragraph:
“One of the best ways scientists know how to measure that response is to look at how many antibodies you’ve produced. In general, people who’ve been infected with the coronavirus tend to have lower levels of antibodies than those who’ve been vaccinated, said Aubree Gordon, an epidemiologist at the University of Michigan.”
This is a straight-forward experiment — look at the antibody count of someone post-covid and compare them to someone post-vaccine.
And what they say it true.
But it took a while to find out that antibody count wasn’t the full measure of protection, and that natural immunity provided a benefit through another mechanism.
But to give Fauci his fair credit, he was talking about the combined benefit of natural immunity + vaccines back in 2021:
https://www.cnbc.com/2021/05/05/fauci-says-studies-show-people-whove-had-covid-and-get-vaccinated-may-have-more-protection-against-variants.html
@Gary, I get it that there are those with health issue and will need vaccines and other drugs to live, more or less normal live or prolong their lives. However, have you seen TV or printed ads lately? One out of every 4 ads is about a drug from a pharma company promising a better life “take X once a day and you are in heaven”. Of course, those ads are followed with a 2 second fast talk and fine prints of how “X” may kill you too with all the side effects.
We have no clue about Fauci’s Sacrament side effect and instead of the expert saying get out and exercise, eat healthier food, don’t over eat, over consume alcohol or use drugs, they are offering a quick fix, the Sacrament.
Americans are hooked on illegal drugs that where they put their trust to buy drugs from a total stranger. Americans are now also hooked on so called “approved” FDA drugs for a quick fix instead of making a life style change.
But since we do have amazingly good evidence for how good the vaccines are for high risk individuals, calling it the fauci sacrament for these people is just dumb and I think borderline evil because the evidence for older people and younger people who are diabetics or with other co morbidities like sickle cell or on cancer drugs or even just having plain old fashioned hypertension is as good as evidence gets in medicine. Medicine isn’t physics, what constitutes overwhelming evidence in medicine is different then in particle physics!
And, since the evidence for getting
three shots for these people is beyond overwhelming and so any person in this group who isn’t fully vaccinated with the bivalent booster is just being plain old-fashioned stupid and all fair minded people should be advising these people to be fully boasted and using dumb terms like the fauci sacrement rather than separating out the correct recommendation for these people is just plain wrong.
I’m not disputing that there are those who need the Sacrament, like you pointed out. However, do you remember when Dr. Fauci was saying “80% of the population needs to be vaccinated to reach herd immunity” [1] in order for humanity to be saved? And what about most recently recommendation that infant as young as 6 months [2] need to be vaccinated? Sorry, but this is not science.
[1] https://www.cnbc.com/video/2020/12/16/80percent-of-the-population-needs-to-be-vaccinated-to-reach-herd-immunity-fauci.html
[2] https://www.mass.gov/info-details/covid-19-vaccinations-for-children-ages-6-months-to-4-years-old
Sheesh the levels needed for herd immunity change depending on r0. In a simple but actually not bad model it is
1 – (1/r0)
So what fauci said was correct for the time he was saying it. For omicron r0 is so high, the level eeded to obtain herd immunity is probably not possible.
@Gary, please go ahead and listen to what Dr. Fauci said in that video: “75% to 80-85% of the population” need to be vaccinated. He does not include herd immunity.
I get it, this was vert early on during COVID. I get it, Dr. Fauci and the FDA had good intention for the public. And I get it, the government was faced with an unknown and invisible thread. However, none of this rises to the level of COVIDFear and the non-sense mandates that was placed on the public. What’s even worse, the COVIDFear narrative continues to this day by telling the public a 6 month old should get injected!
Do you want to save the public from another epidemic? Start a new EpidemicFear campaign so that 70% to 80-85% of the population eat healthy, start exercising, stop over consuming alcohol or treating marijuana as essential need.
A clarification: it was 80% or so then for a combination of vaccinated and natural immunity. Early on it was not clear that natural immunity was as helpful as it actually was. In fact the evidence at the time seemed to indicate it wasn’t but over time science accumulates more evidence and changes the consensus or to quote a famous economist not a scientist “when the evidence changes I change my opinion what do you do sir?
Actually all of the recent “revelations” about C19 were obvious educated guesses to anyone who knew some medicine and virology and read some old coronavirus research back in early 2020.
I remember quite well my girlfriend (a molecular biologist) expressing rather strong disbelief about the whole panic thing (I was telling her about that new horrible CV from China in the news) and telling me to read some papers and the textbook. Took me few days to convince myself that this is mostly nothingburger and not actually more dangerous than a flu. As a result we never wore masks (willingly), traveled as much as we could, and never vaccinated. Both had a couple bouts of some respiratory viral infection, each very mild. It is very sad to see our friends who spent years hiding in fear, and now are visibly less healthy… not something specific, but way too many aggravated and new illnesses than one would expect from aging alone.
So, here we sit in March 2023, and there’s some credible evidence that:
1. Masking was ineffective at reducing transmission. (Stop the spread?)
2. The vaccine didn’t really affect transmission that much (stop the spread II?)
3. The virus may have escaped a Chinese viral lab. (Cover up/conspiracy?)
So, a bunch of “journalism” and moral posturing turned out to be information-age-scale gaslighting, which contributed to political divisiveness, alienated friendships, and even family strife. Trillions of dollars were spent in an effort to “do something” and it all looks like it may have been for nought. Think any lessons will be learned? Will our betters be held accountable? Will people understand that they should un-shun the nonconformists, or will pointing this out just alienate us further?
This “didn’t stop transmission” issue should be put to bed because people took it the wrong way.
I saw the outrage bounce around right-wing media, with people misinterpreting and overstating its meaning.
Basically, if you want to know if a vaccine reduces the spread, you would ideally want to know two things:
1) Is a vaccinated person less likely to catch the virus?
2) If a vaccinated person is infected, are they less likely to infect someone else?
#1 is easy to test. You vaccination a person and then follow them to see if they caught the virus.
But #2 is difficult. How do you know who they infected? If you find someone else who is infected, who do you know where it came from?
For #1, the proof is strong that it reduces infection. For covid v1, reduction was around 90%. For later variants, it was lower, but still useful.
But they didn’t know anything about #2, as the CEO said.
But of course, if you stop people from getting infected, you’ve reduced the disease from spreading!
And this is true even if a vaccinated person can spread it just as easily.
But right-wing media jumped on this and spread the idea that the vaccines do nothing to stop the virus from spreading, and that the vaccine makers never tested anything related to spread.
Not sure if this misinformation was caused by ignorance or malice, but it’s a wild lie that’s spreading among those of a specific political persuasion.