Bostonians blame Trump for their biotech slump
Nearly everyone in Boston expressed hatred for President Trump v1.0, despite the fact that 2017-2020 coincided with great economic times for the city and state (the final year of Trump’s first term wasn’t so great due to the self-inflicted wounds of lockdown and school closure). Now that the Massachusetts biotech industry is sagging, they’re blaming President Trump 2.0,
First, are the good times over? The Wall Street Journal says that they are:
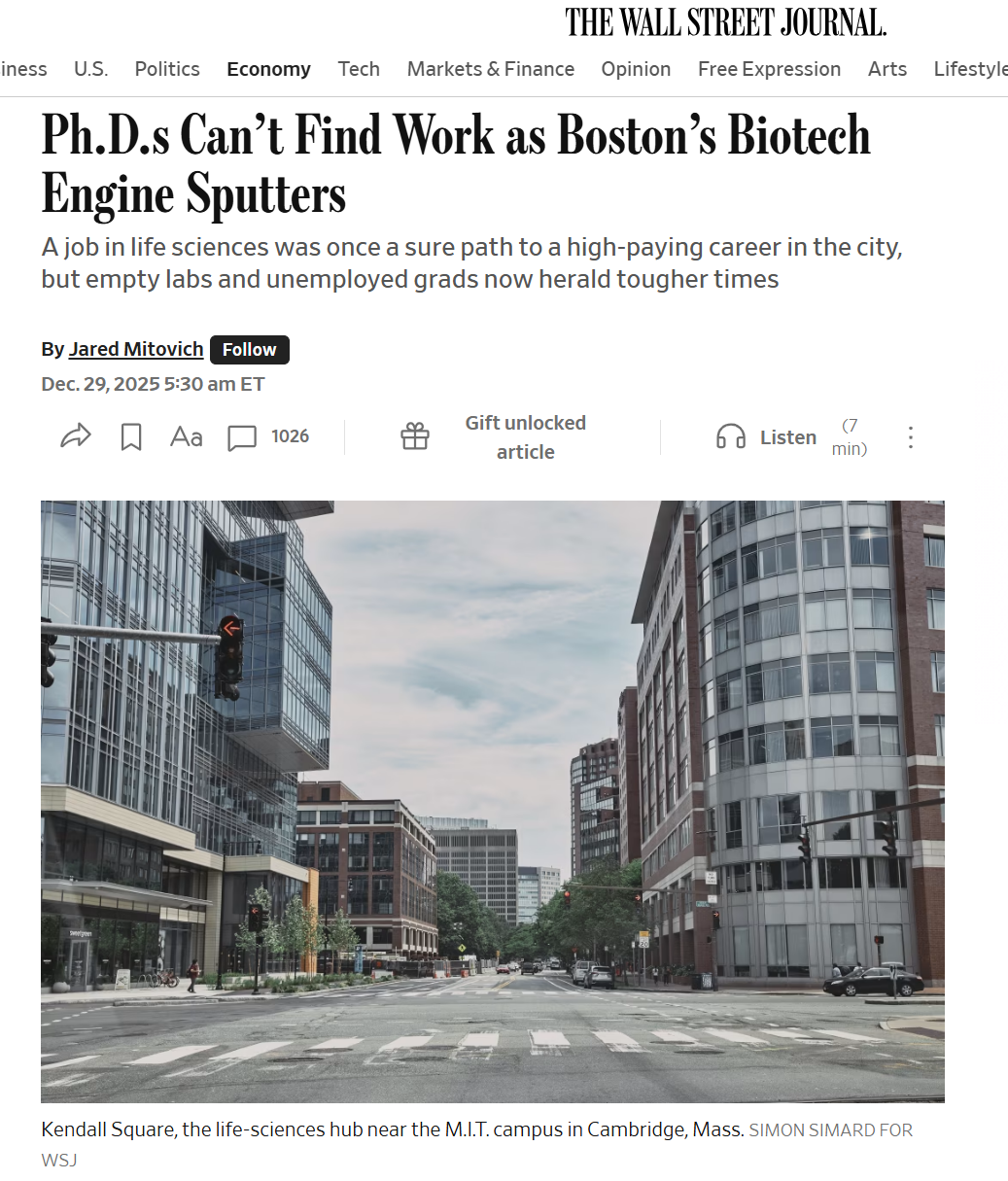
Massachusetts experienced a slight decline in its roughly 65,000 biotech research-and-development jobs in 2024 after years of mostly strong increases, including during the Covid-19 pandemic, according to federal data. The numbers indicate that job losses continued through at least June, while hiring remains sluggish.
By the end of September, nearly 28% of greater Boston’s laboratory space sat empty, according to the latest estimates from real-estate firm CBRE.
Folks in Massachusetts who decry inequality are especially upset that some federal money is being spent in places that aren’t as rich as Massachusetts:
“Every stage of the life cycle has been impacted by policy or regulatory uncertainty this year,” said Kendalle Burlin O’Connell, chief executive of MassBio, an industry trade group. The impact has hit startups especially hard, she said.
A continued downturn poses risks for a region where workers will put up with sky-high real-estate costs if they can land high-paying jobs. Massachusetts faces competition from other states and China, which are eager to peel away talent and investment.
“There are states and countries chasing us every single day,” Gov. Maura Healey said in an interview.
On the federal front, the Trump administration has terminated tens of millions of dollars in active grants in Massachusetts this year, according to Grant Witness, an independent group of researchers tracking grant terminations and reinstatements by government science agencies.
Also, while Massachusetts gets the most National Institutes of Health funding of any state on a per capita basis, changes are afoot. The NIH announced a strategy in November to promote “broad distribution and geographic balance” by spreading around future research funding.
(Does the governor have any experience in building or attracting businesses? It is unclear. “Massachusetts’ Attorney General Maura Healey becomes 1st lesbian elected governor in U.S.” (state-sponsored PBS) doesn’t explain the governor’s background other than “she is lesbian”.)
A friend who is a senior administrator at Harvard was spewing venom at Donald Trump in April for “cutting NSF funding” and thus destroying Maskachusetts. I refrained from pointing out that Congress sets NSF funding levels, not the president, no matter how much of a hater he/she/ze/they might be. Instead I asked her why she expected Boston biotech to stay on the gravy train given that Boston biotech hadn’t developed any drugs that are significant to the average human. She responded with “CRISPR”. I refrained from pointing out that most of the work on CRISPR was done at UC Berkeley and in Europe (the Nobel winners were Jennifer Doudna (Berkeley) and Emmanuelle Charpentier (variety of European institutions, including Max Planck, which has a single American outpost… in Jupiter, Florida), but did note that there isn’t any widely available treatment based on CRISPR. She said that there would be, but for Donald Trump’s interference.
I did ask why she expected Boston biotech to continue standing under the money shower if Boston hadn’t developed any of the recent blockbuster drugs. I said maybe investors, including NSF, would keep pouring money in if Boston-based companies had developed Ozempic. She corrected me: Ozempic was developed in Boston (ChatGPT says it was developed by Danes in Denmark working for Novo Nordisk; related drug Wegovy is also from Novo Nordisk; related drug Mounjaro was developed in Indianapolis by Eli Lilly). It occurred to me that today’s Boston Soviets have a mental attitude just like our charicature of 1970s Russian Soviets, i.e., any failures can be blamed on outsiders (the U.S. for 1970s Russians; Donald Trump for Bostonians in the 2020s) and any inventions worldwide can be attributed to heroic local Soviets.
Maybe Boston-based companies developed whatever class of drugs whose sales were comparable to GLP-1 ($75 billion/year)? The last time the pharma world had something of similar value was with the statin, discovered by Akira Endo at Sankyo in the Japan section of Boston and turned into an FDA-approved pill by scientists in the Rahway, New Jersey section of Boston at Merck. (I’ve always been a statin skeptic, incidentally; if a blood test shows high cholesterol because a human is fat and sedentary, a pill that changes the blood test result without changing the fat/sedentary problem doesn’t seem like it will lead to immortality.)
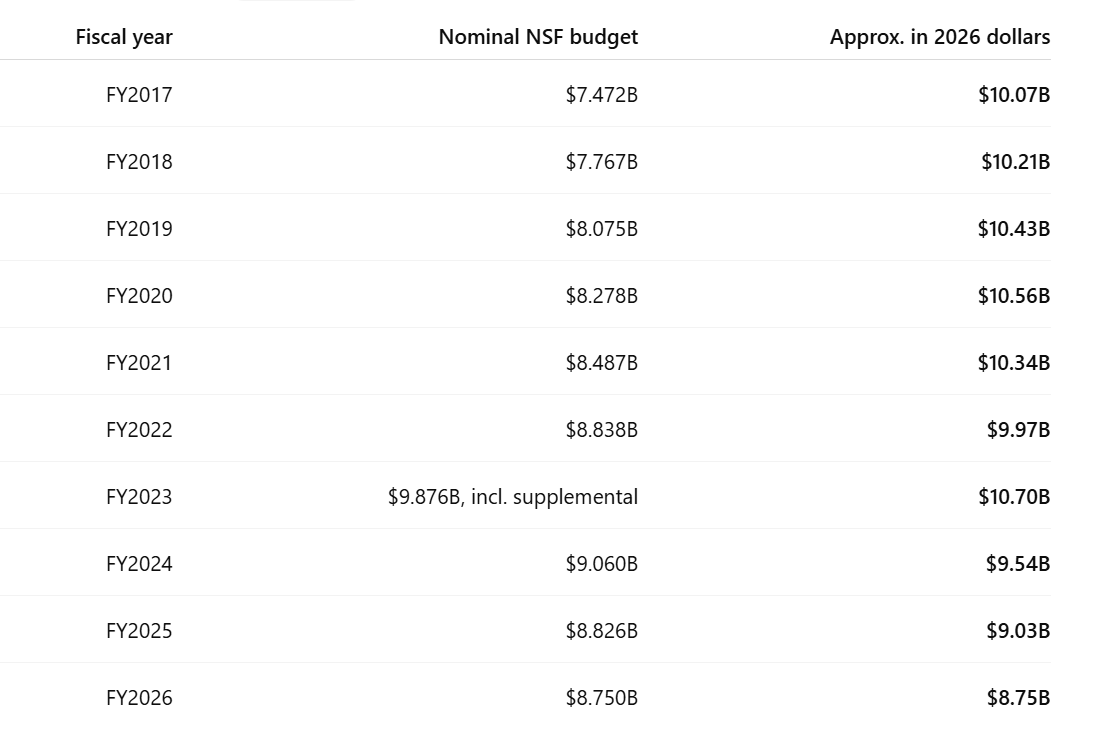
ChatGPT on inflation-adjusted NSF spending, showing modest growth during Trump v1.0, a bump during coronapanic, and a sag that began during the Biden-Harris administration (money was diverted to supporting migrants?):
The Harvard employee’s focus on NSF might be misplaced. Consistent with the WSJ’s reporting, it seems to be NIH that funds more biotech. NIH’s total research funding is about $27 billion, much larger than NSF’s entire budget. NIH will fund clinical trials and NSF won’t.
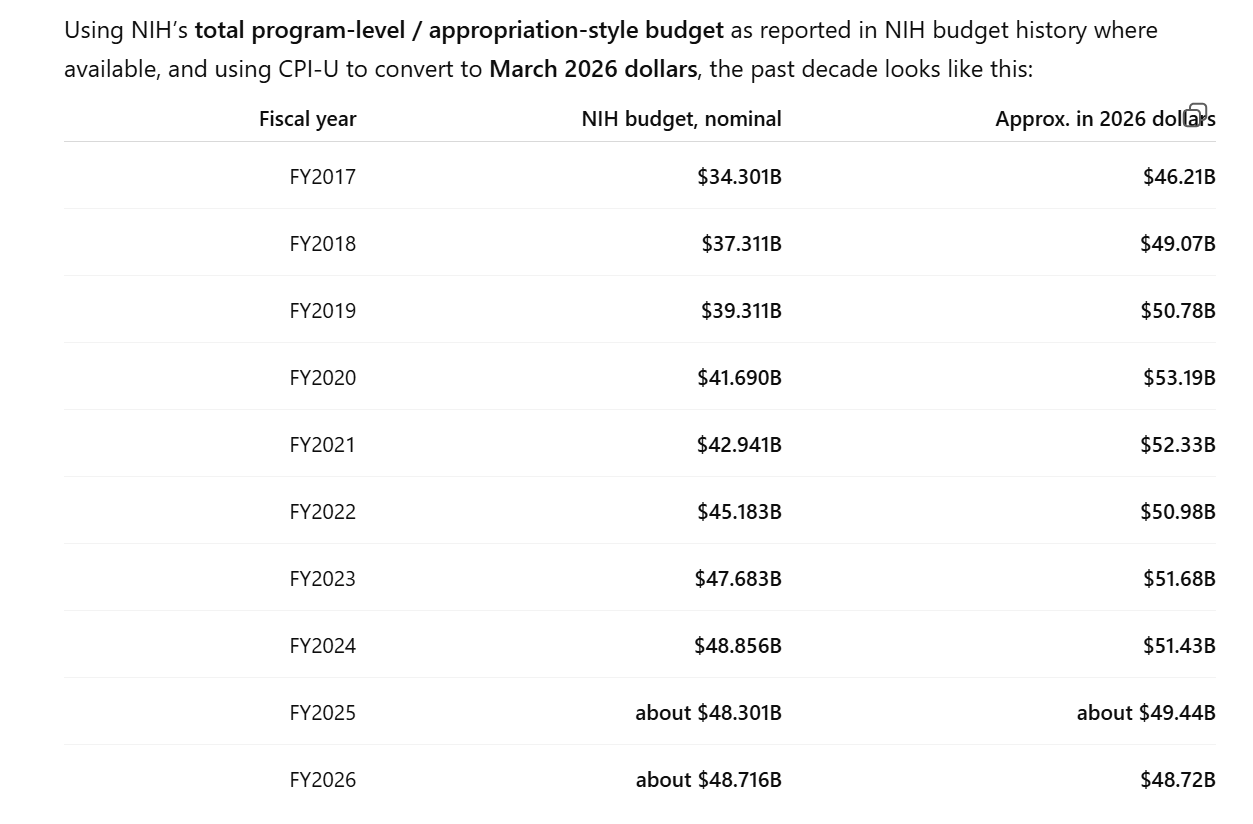
Given that Americans were so passionate about avoiding death from disease during coronapanic, while remaining indifferent to being killed in car accidents (imagine the lives safe with my 35 mph computer-enforced speed limit!), from lifestyle choices such as consuming alcohol and marijuana all day, etc., it surprises me that NIH funding hasn’t doubled, in real terms, since 2017. Maybe the explanation is that the entitlement/welfare/migrant-welcoming systems consume all of the growth in government spending.
Probably the real explanation for the Boston slump is that the boom was too good to last, as one WSJ source said:
“There was so much money that the sector got overbuilt,” said Alexis Borisy, founder of Boston-based Curie.Bio, a biotech venture firm that has raised more than $1 billion for early-stage biotechs. “If there was a good idea, there’d be 10 companies all built at the same time to go do it.”
It’s still interesting to me that Bostonians felt that it was their right to claim an ever-expanding share of federal tax dollars and of GDP, despite not having delivered any medications that improve the average American’s health or life. The Righteous of Maskachusetts are quick to criticize “white male entitlement”, but what is a more “entitled” attitude than expecting to stay on the gravy train after decades of underdelivering?
Full post, including comments