Raping by lying
“You Were Duped Into Saying Yes. Is That Still Consent?” (New York Times, March 5):
Imagine the following hypothetical situation: Frank and Ellen meet at a night course and end up getting drinks together after class several times. The drinks start to feel like dates, so Ellen asks Frank if he is married, making it clear that adultery is a deal-breaker for her. Frank is married, but he lies and says he is single. The two go to bed. Is Frank guilty of rape?
To many feminist legal scholars, the law’s failure to regard sexual fraud as a crime — when fraud elsewhere, such as fraud in business transactions, is taken to invalidate legal consent — shows that we are still beholden to an antiquated notion that rape is primarily a crime of force committed against a chaste, protesting victim, rather than primarily a violation of the right to control access to one’s body on one’s own terms.
The author, Roseanna Sommers, is a law professor and she essentially concludes that Frank did rape Ellen.
If the goal of “feminist legal scholars” is to help those who identify as “women”, I wonder if lying = rape will actually be helpful. Perhaps the theory is that this will be good for those who identify as “women” eager to file rape lawsuits because it is almost exclusively those who identify as “men” who lie to obtain consent. But the hypothetical example isn’t comprehensive. If Ellen is having sex in order to turn a profit via child support, for example, Frank being married actually improves her chances of getting consistently paid for 23 years (if Frank can’t pay, his beleaguered spouse will work and pay). What if Ellen were to say “It’s okay because I’m on the Pill”? She still has a good claim for $2 million in tax-free child support, but now Frank can file a civil lawsuit against her for rape and receive some of that money back (and then Ellen can file a child support modification lawsuit saying that Frank’s new wealth entitles her to higher monthly checks?).
Let’s tweak the story a little, to align it with a common lie…
Frank asks Ellen if she has previously slept with more than 100 sex partners, making it clear that being a Tinder super user is a deal-breaker for him. Ellen is Tinderlicious, but she lies and says she hasn’t had sex with anyone since the Obama years. The two go to bed. Is Ellen guilty of rape?
Would it be a positive, from a feminist perspective, for Ellen to face a lawsuit in which sexual history is a legitimate subject for cross-examination?
How about financial matters? “Do Americans marry for love or money?” (MarketWatch):
Some 56% of Americans say they want a partner who provides financial security more than “head over heels” love (44%), a recent survey released by Merrill Edge, an online discount brokerage and division of Bank of America Merrill Lynch BAC, +1.18%, found. This sentiment is held in almost equal measure by both men and women (54% and 57%).
Should someone who identifies as a “woman” be exposed to a rape lawsuit because she purportedly told someone at a club that she expected to be promoted to a lucrative executive position that, in fact, did not materialize and that a reasonable person should not have expected? After a year of sex without the promotion materializing, the “duped-at-the-club” person now has a rape claim?
What about people who have difficulty remembering what they said years ago? “New state law extends the statute of limitations for rape in New York” (CNN):
New York Gov. Andrew Cuomo signed legislation Wednesday that extends the statute of limitations for certain cases of rape and other sex crimes. He was joined at the signing by actresses… And under the law, victims now have 20 years in which to bring a civil suit for the offenses.
(and maybe Governor Cuomo was joined by some of those actresses after the signing as well?)
Suppose that a plaintiff sues Dianne Feinstein, alleging that the 87-year-old senator committed rape by lying in 2000, when she was 67 years old. That’s within the statute of limitations for rape, but are 20-year-old statements within the likely memory of an 87-year-old? Unless Feinstein is much sharper than the average 87-year-old and can testify convincingly, the $88 million that she acquired via marriage can be mined out by the plaintiff?
The good news is that the taxpayers of Michigan paid Professor Sommers to think about these issues! (or, if $billions for universities is buried somewhere in the latest $1.9 trillion spending package, perhaps taxpayers nationwide paid for this idea)
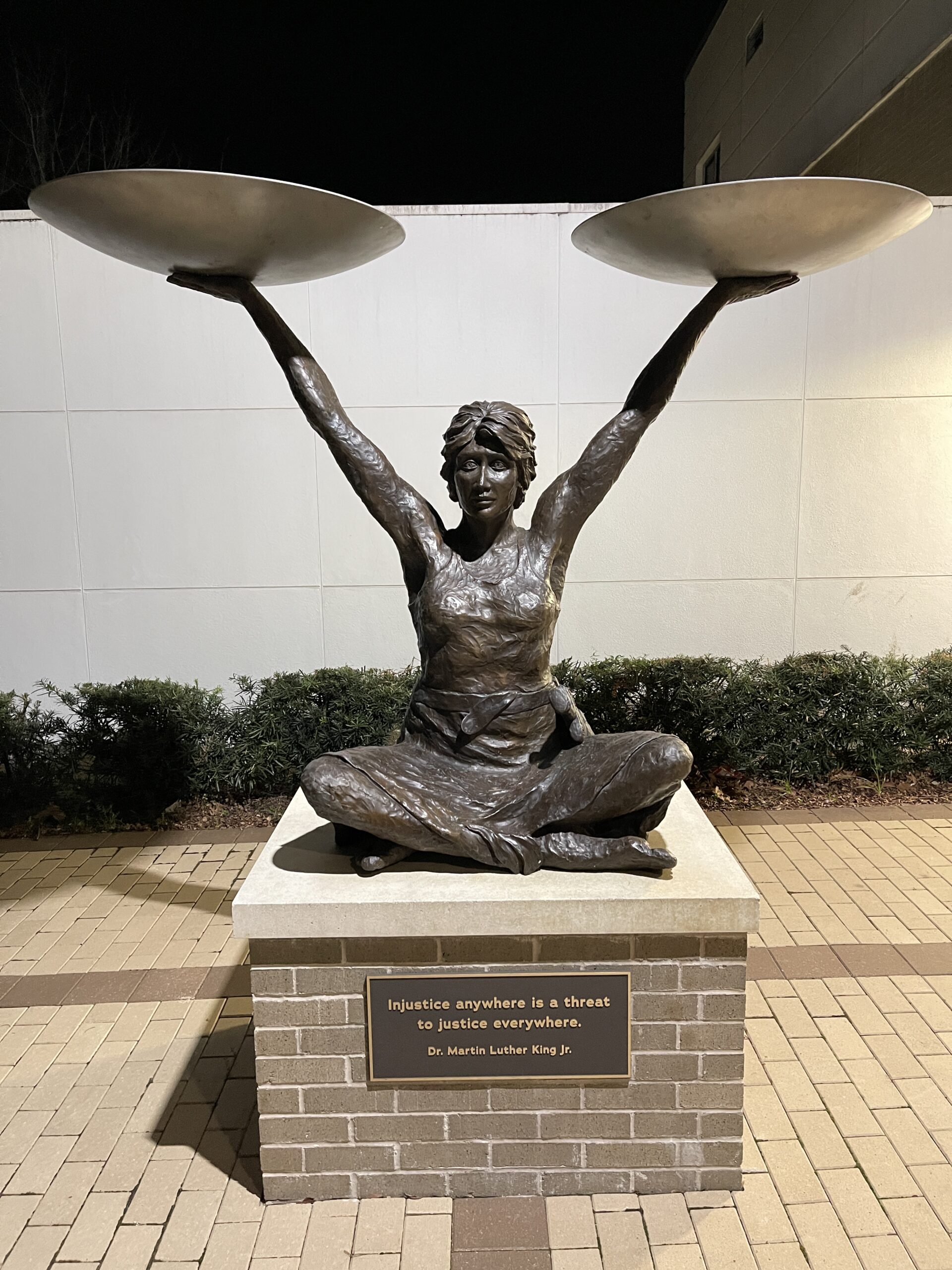
The scales of Justice, Gainesville, Florida, January 2021: