I’m not sure if it’s our inflation-free (TM) economy or that self-storage places underprice at move-in time and then raise the rent according to how difficult they think it will be for you to move your stuff, but the local self-storage place (Compass) just bumped our rent by 24 percent after six months (54 percent annual inflation rate), effective today.
Is this
a sign that inflation is alive and well?
an indication that South Florida continues to prosper?
a standard bait-and-switch tactic by self-storage places?
Rents for apartments and prices of houses are rising only gradually here right now, as far as I know, so I don’t think the “South Florida is booming” explanation is correct.
So why are we seeing an increase in people being labeled as depressed, or autistic, or ADHD?
Some of these labels have become high status. Nonbinary is high status among affluent teenagers. But I do not believe that the desire for status is the main driver.
I suspect that more children are being born with innate mutations, because their parents are older, reducing sperm and egg quality. These mutations result in unusual personality characteristics.
I suspect that children are spending less time with other children. Families are smaller. There are fewer neighborhoods with a lot of children. And there is a reluctance to let children go out on their own seeking children with whom to play. I suspect that having close adult supervision most of the time stunts children’s growth in social competence and confidence.
Children are skilled at manipulating their parents. When parents are easily manipulated, the child’s self-control is less likely to develop. When there are four children, no individual child has a good chance to manipulate parents. When there are one or two, manipulation is easier.
Children are skilled at manipulating their parents. When parents are easily manipulated, the child’s self-control is less likely to develop. When there are four children, no individual child has a good chance to manipulate parents. When there are one or two, manipulation is easier.
I wonder if it’s time for my standard line: “If you think teenage parenting is bad it’s only because you haven’t seen old people with kids.”
Any chance that the above trends will reverse? It doesn’t seem likely among native-born Americans who are college-educated. I talked to a senior at Brown the other day (considering how kids will do almost anything to get into an Queers for Palestine League school these days, she was surprisingly diffident about the overall experience there). She’s moderately religious/conservative and, therefore, might be expected to have more children than average for her cohort. She said that she didn’t want to have any children until she was at least 30 years old (“my 20s are for me”). Also, she didn’t want to have any kids until she’d been married for at least two years (“in case I want to divorce,” she noted, expressing zero commitment to marriage per se (i.e., she would stay married only if it seemed like the best option going forward)). So her life plan was to get married at some point between 26 and 28 and then have children at some point between 30 and 32. This is a recipe, I think, for having exactly the kind of family that Arnold Kling decries (older parents, 1-2 children, maybe just one parent if things don’t go perfectly).
Loosely related…
A $5000 baby bonus?
This country would be better off sterilizing anyone who would choose to have a baby for $5000.
The post that was scheduled for May 5, 2025 somehow didn’t get properly handled by WordPress. In order to deliver on my tagline of a posting every day, let me backfill it with a tale of going through a TSA checkpoint: They had a lot of signage about their new demand for REAL ID. I offered my driver’s license and explained “It’s real to me.” #MyTruth
Today we begin our celebration of Public Service Recognition Week, in which we “honor the people who serve our nation as federal, state, county, local and tribal government employees.”
In writing the post about my mom’s 25th high school reunion, I noticed that Zillow in 2025 displays our old family homestead, which was bulldozed in 2012…
Zillow still shows the crummy 1953 Cape Cod house in which we grew up (address above) and lists the mansion’s 1,603 square feet of space (we also used the basement, though, and a screen porch that was glassed in and maybe isn’t included). However, it was bulldozed within hours of being sold in 2012 and the Indian immigrants who purchased it built a McMansion in its place.
What I didn’t notice until more recently was that the Zillow page indicates that my parents’ old house wasn’t reassessed despite having been bulldozed and replaced by a vastly-more-valuable McMansion:
Montgomery County, Maryland is run by Democrats who would be the first to tell you how much smarter they are than Republicans. Ditto for the state government, which I think might be responsible for assessment. The house next door, 6409 Dahlonega, was bulldozed and its assessed value went up from $382,000 in 2006 to $1.7 million in 2007 (today at $2.2 million). My parents’ old house would have brought in more than double the current property tax over the past 13 years if it had been assessed at market rates.
(Incidentally, the people who built the magnificent edifice at 6409 Dahlonega are no longer paying property, income, or, when the time comes, estate taxes to Montgomery County/Maryland. They moved to Clearwater Beach, Florida towards the tail-end of coronapanic.)
These data shatter my preconceptions about government, which I thought was a well-oiled machine for collecting maximum taxes. Maybe there is some rule in Maryland or in Montgomery County that prevents a reassessment after a bulldozing, but I don’t know what it would be.
Anyway, let’s celebrate the property tax assessors of Maryland for their hard work, even if trees obscured their view of the old 1,600-square-foot cottage that was replaced by a hulking McMansion.
Very loosely related…
I wonder if there's a very common event that would cause women to become both single and homeowners at the exact same time? 🤔 pic.twitter.com/wOF0VjV8EN
With the hated dictator threatening to defund NPR (NBC), let’s have a quick survey regarding favorite NPR articles for the working class taxpayer to fund.
Here’s one that I received recently from a friend in San Francisco (he’s a closeted Deplorable because diversity is our biggest strength and also anyone who didn’t vote Democrat has to be fired):
The peasants had to pay the following elites, apparently, to obtain this valuable lesson:
“It’s Time To Up Your Mask Game” (NPR, August 2021): since every American who wants the proven-perfect COVID-19 vaccine has already had it… “Wear two masks”
There was no population-level ob/gyn exodus away from abortion-restrictive states post-Roe.
From the quarter right before the June 2022 Dobbs v. Jackson Women’s Health Organization decision through the end of the study in September 2024, 95.8% of ob/gyns remained in states that protect access to abortion, 94.8% remained in states threatening bans, and 94.2% remained in states with abortion bans, reported Becky Staiger, PhD, of the University of California Berkeley, and colleagues.
“The only statistically significant difference suggested that the share of physicians who are ob/gyns decreased less in threatened states than in protected ones, opposite to the expected finding if ob/gyns were leaving states where abortion is threatened,” the authors wrote.
(I apologize for the hateful language in which “abortion care” is presented without the “care”.)
The full article says “Numerous media reports have described physicians leaving states where abortion is banned in response to these concerns, including cases of retirement or migration”.
Where should an ob/gyn passionate about delivering abortion care have moved? Maskachusetts law allows abortion care at 37 weeks of pregnancy or even more if a single physician believes that the abortion care will preserve “the patient’s … mental health”:
If a pregnancy has existed for 24 weeks or more, no abortion may be performed except by a physician, and only if in the best medical judgement of the physician it is: (i) necessary to preserve the life of the patient; (ii) necessary to preserve the patient’s physical or mental health; (iii) warranted because of a lethal fetal anomaly or diagnosis; or (iv) warranted because of a grave fetal diagnosis that indicates that the fetus is incompatible with sustained life outside of the uterus without extraordinary medical interventions.
We have tremendous inequality among U.S. states. Household income in California was $95,500 in 2023 dollars (Wokipedia) while Texas households enjoyed only $75,800 in income and in Mississippi the median household income was only $54,000. Who works to redress this inequality? Not the federal government, which keeps spending taxpayer money in the richest states, either directly (grants to universities, student loan subsidies, tuition subsidies) or indirectly (pharma and health care purchases).
But let’s consider Elon Musk. He has moved at least four companies from richer-than-average California to poorer-than-average Texas: Tesla, X, SpaceX, and The Boring Company. Is there anyone else alive who can be said to have done as much to reduce inequality among the states? If not, we must anoint Elon Musk as America’s Greatest Social Justice Warrior.
The company is also getting an injection of $17.3m (£13.4m) from the Texas government to develop the site, a grant that officials say is expected to create more than 400 jobs and $280m in capital investment in Bastrop.
Although I can’t blame Elon for taking the state’s money, that last bit is upsetting to me as a 14th Amendment Equal Protection purist. Why is it acceptable for a government (state, in this case) to favor one business with tax breaks while hitting smaller and less-connected businesses with the full force of taxation. I would like to see all of these state programs eliminated so that 2-person company is on a more level playing field with a 2,000-person company.
I think that we can all agree that our democracy would be at an end if a president were to defy the Supreme Court. Has it ever happened? I asked ChatGPT. Here are some snippets:
In the early 1930s, FDR removed the U.S. from the gold standard and invalidated gold clauses in both public and private contracts. These clauses had allowed creditors to demand payment in gold, insulating them from inflation.
The Supreme Court heard several consolidated cases, the most famous being Perry v. United States, which challenged the government’s abrogation of gold clauses in government bonds.
There was press speculation that FDR might defy the Court if it ruled against him, especially since the stakes were so high for the administration’s economic agenda.
In a narrow 5-4 ruling, the Court upheld the government’s position, essentially avoiding a constitutional crisis.
Chief Justice Charles Evans Hughes wrote the majority opinion in Perry v. United States, holding that while the government’s action was technically unconstitutional, the plaintiff had not suffered a legally redressable loss.
Yes, Franklin D. Roosevelt did prepare a contingency speech in the event that the Supreme Court ruled against him in the 1935 gold clause cases, particularly Perry v. United States.
The speech was drafted in anticipation of the Supreme Court potentially striking down his policies on invalidating gold clauses.
In this prepared address, FDR was ready to assure the public that he would not allow the economic system to collapse, even if it meant ignoring the Court’s ruling. The draft included language that strongly implied he would defy the decision.
According to historical sources, including William Leuchtenburg’s writings and Henry Morgenthau’s diaries, the speech essentially framed any contrary Court ruling as a threat to national survival, and FDR positioned himself as the defender of the people’s economic security over rigid constitutional formalism.
Here’s a paraphrase of the key idea from that draft speech:
If the Supreme Court were to rule that the government must repay debts in gold, then the administration would have no choice but to protect the nation’s economy by refusing to comply—suggesting a potential constitutional crisis.
Henry Morgenthau Jr., FDR’s Treasury Secretary, kept detailed diaries. In entries from January 1935, he discusses FDR’s draft speech and concerns about the Supreme Court decision. These diaries are held at the Franklin D. Roosevelt Presidential Library and are available digitally. Look for entries in January–February 1935 regarding the gold clause litigation.
Secondary source: Franklin D. Roosevelt and the New Deal, 1932–1940 by William E. Leuchtenburg:
“[FDR] had even prepared a radio address for the evening of the day the Supreme Court ruled, asserting that the government would defy the Court if it invalidated the gold policy. But the Court, by a narrow margin, spared him the necessity.”
Today is the deadline for accepting college admissions offers. For parents and kids who are disappointed, let’s consider the strategic mistakes that they might have made.
Most obviously, a child who fails to identify as Elizabeth Warren’s cousin (i.e., “Native American”), is at a disadvantage. Same deal for Black, Latinx, 2SLGBTQQIA+, etc. These identifications are often matters of personal choice and colleges and universities have made their prejudice against cisgender heterosexual whites and Asians clear so a failure to identify in some kind of preferred category isn’t excusable.
Some more nuanced lessons from the NYU data leak, from a friend in suburban Boston who is numbers-oriented and fed everything into a database management system:
The real comparison is between “cohorts” – basically they lump people into clusters by zip code, background, interests. NYU admissions rate for our [somewhat rich suburban public] high school was effectively 3%. Way lower than their average admission rate.
Moving to a zip code from which few people apply to the schools of interest could help. Moving to a less elite neighborhood within the same metro area, for example, could actually save a huge amount of money as well as enhancing a child’s admissions chances. Evincing an interest in less-popular majors, e.g., classics, could help. (My friend: “It isn’t enough just to say classics – you need Latin courses, participation in known Latin competitions, etc.”)
(Maybe the ultimate hack would be moving into a zip code that is 99% occupied by The Villages or similar kids-forbidden development. It’s virtually guaranteed that zero other kids will apply from that zip code if kids under age 19 aren’t allowed to live in 99% of that zip code.)
From a different friend whose child attends an elite private school in Philadelphia:
One kid got into [Queers for Palestine League] penn last year for deferred admission because of crew and now [the child’s] class has twice as many kids doing rowing than previous class
Let’s check in with Harvard, where they say that they hate inequality and also that they want as much federal money as possible funded to richer-than-average schools in richer-than-average states. (i.e., don’t send the money to universities in poorer-than-average Michigan, Ohio, and Mississippi where the result would be increased equality among states) Layla L. Hijjawi, a Crimson editor:
Mahmoud Khalil, for example, is a green card holder — otherwise known as a lawful permanent resident — who has been detained, apparently for pro-Palestine organizing at Columbia University. The Trump administration has linked his actions, which ought to be defended by the First Amendment, to terrorism, claiming he poses a threat to American foreign policy.
One doesn’t even need to organize pro-Palestinian protests to become a target; simply attending one is enough to merit condemnation and threatened deportation, as the case of Yunseo Chung makes clear.
Most egregiously, merely publishing a pro-Palestine opinion piece — as many editors of this very paper have — can apparently result in being snatched off the streets and detained by Immigration and Customs Enforcement for supposedly supporting terrorism like Rumeysa Ozturk, another permanent resident of the U.S.
This is a clear escalation of its attack on pro-Palestine speech on campus. Harvard must not yield in the face of this right-wing pressure. The conciliatory approach of Harvard President Alan M. Garber’s email regarding funding review misses the mark by treating the review as being pursued in good faith, ignoring the obvious insidious and chilling intention of the campaign developing under the guise of preventing antisemitism.
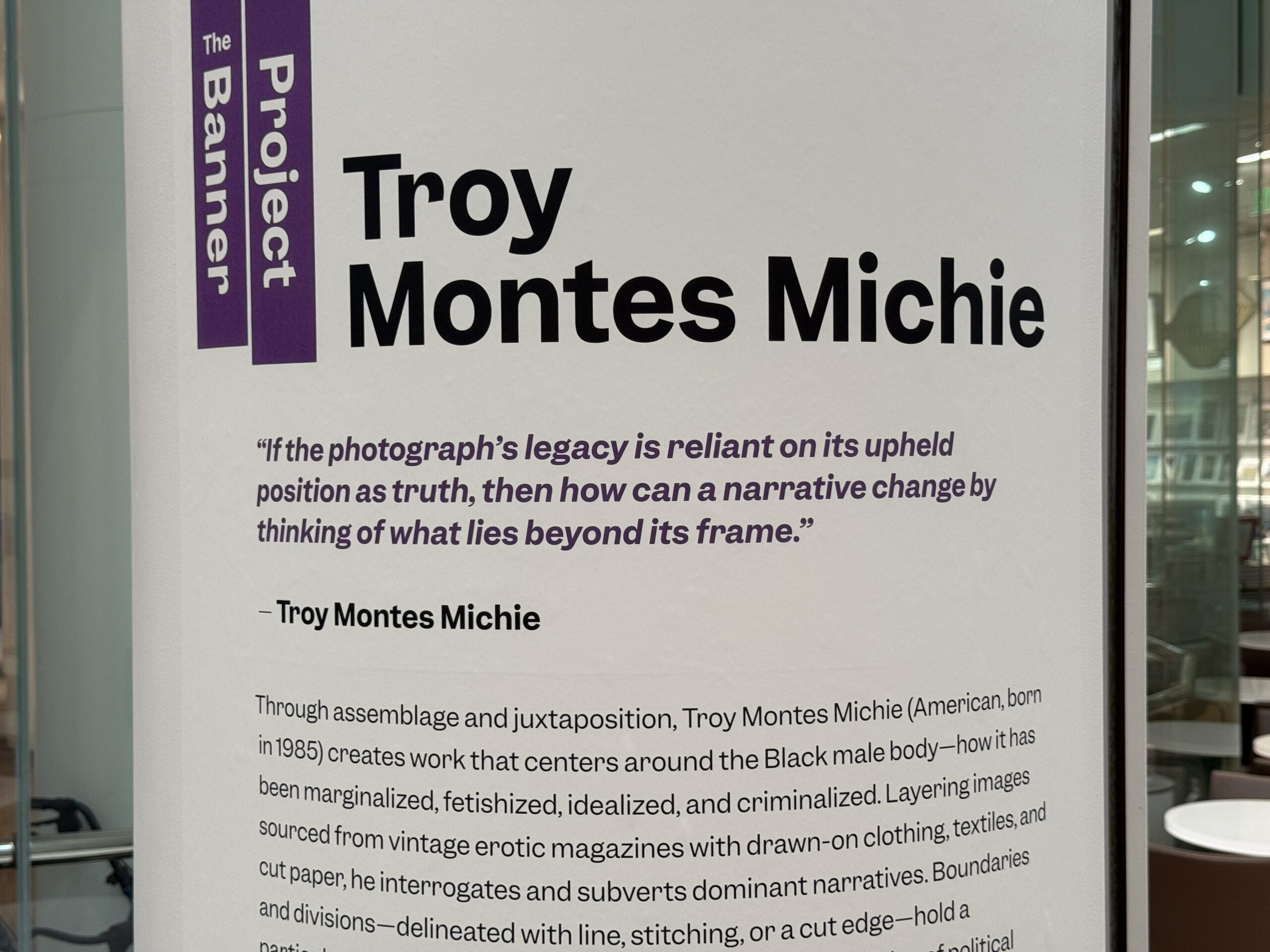
A friend and I visited the Boston Museum of Fine Arts on April 12, 2025. Our experience started in the coffee shop where we were urged to wash bananas before eating even though no sink was provided for visitors. We were also reminded that “the Black male body … has been … criminalized” (this will be Karmelo Anthony’s defense against his wrongful prosecution for murdering Austin Metcalf?):
How about this task for our future AI overlords: custom stained glass for every house? Here’s what rich people were able to get from Tiffany and John La Farge back in the Gilded Age:
Optimus isn’t ready yet to fabricate the glass, but we can check in with ChatGPT’s response to “Please design me a stained glass window that depicts a happy golden retriever chasing a squirrel with palm trees and orchids in the background”:
(People keep saying that AI will be deflationary, but that makes sense to me only if human wants are finite. If I can get AI to design and install a custom wrap for our car every 6-12 months at a reasonable cost then I would pay for that whereas right now it is mostly businesses with a commercial imperative that will pay for wraps.)
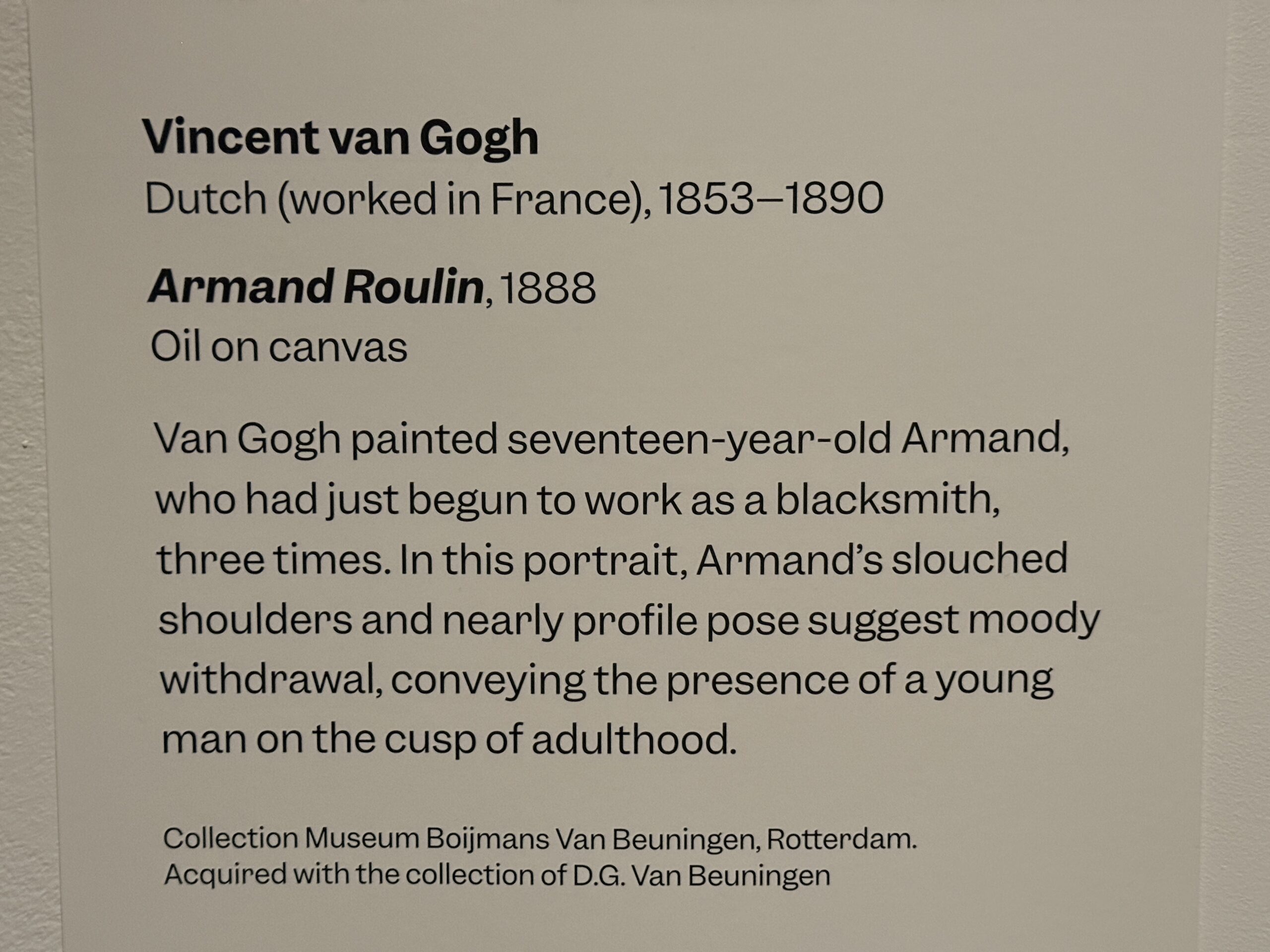
At a van Gogh exhibit, we learned about teenage rebellion in the bad old days: put on a suit and go to work.
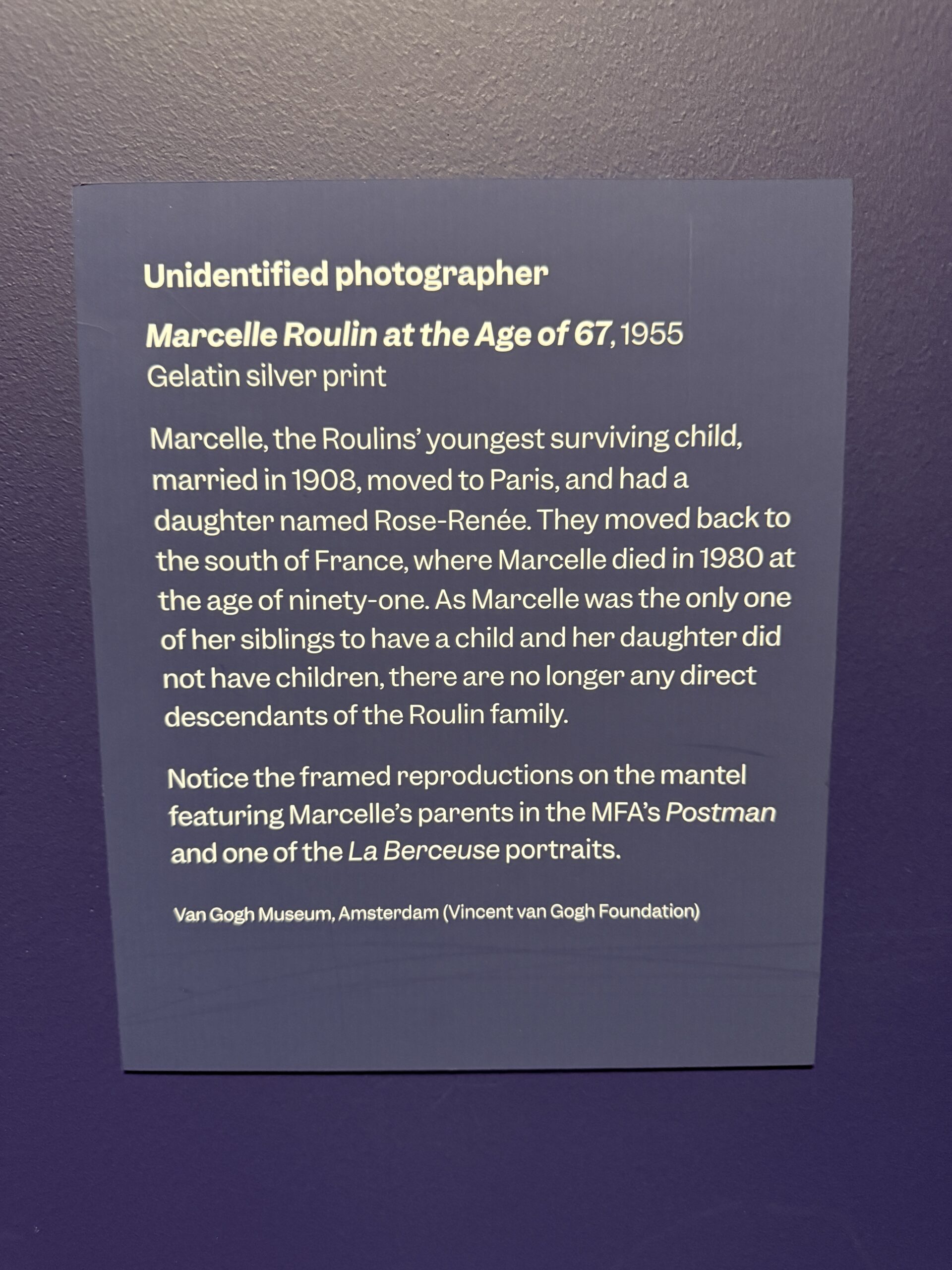
The French family that van Gogh painted literally went extinct (though only a conspiracy theorist would say that they’ve been replaced by migrants):
Visitors and staff had both voluntarily entered the crowded museum in reliance on inexpensive face masks as protection from aerosol viruses:
Children learn about art, and the importance of voluntarily entering crowded indoor environments while wearing a mask, from a docent:
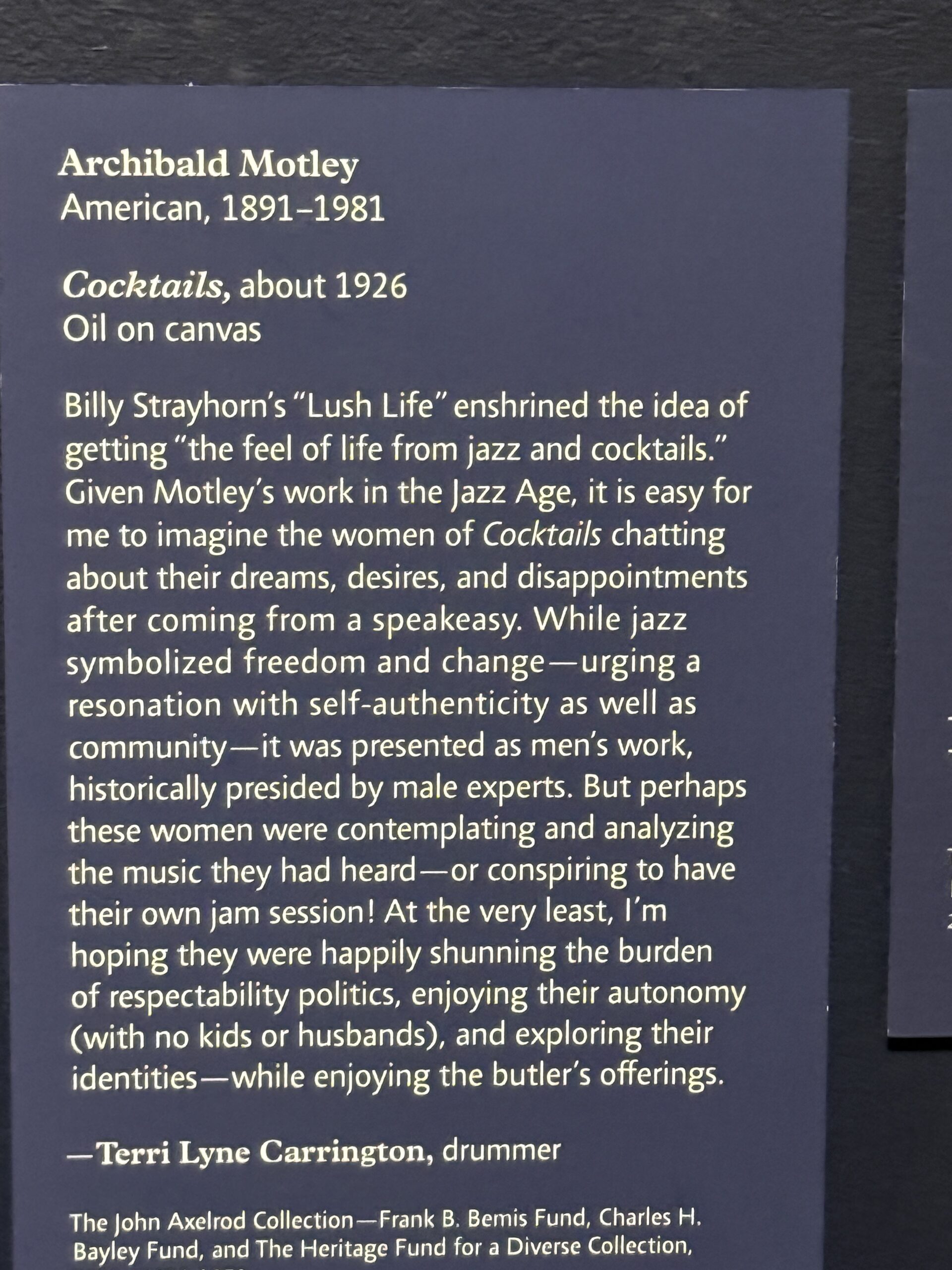
The museum posts the idea that the ideal life for a woman is to have “autonomy”, defined by “with no kids or husbands”, so that they can “explore their identities”:
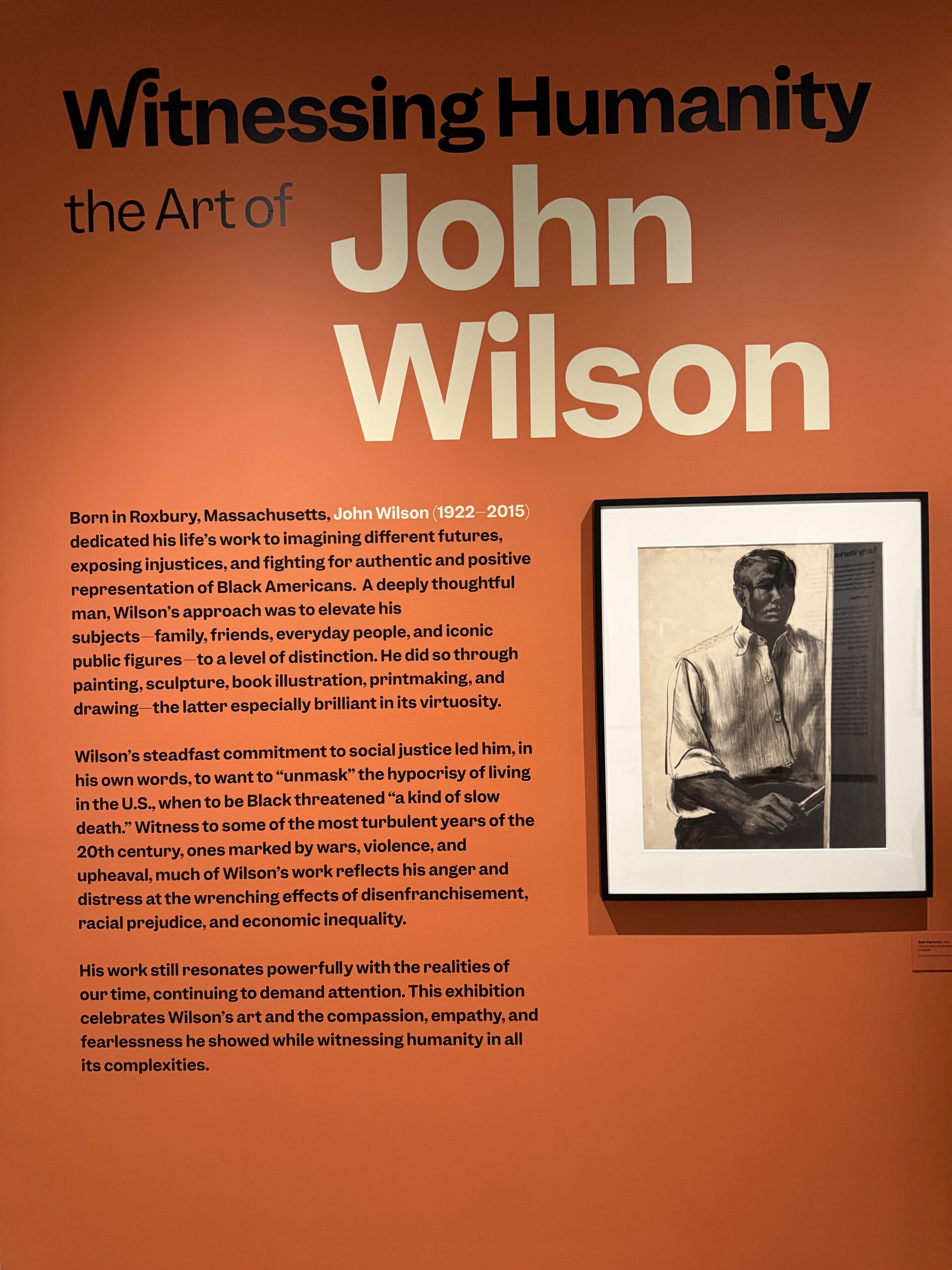
The museum had organized an exhibition by a Black artist who was an expert on Blackness and social justice. Wikipedia says that he married a white woman and then the two of them moved to Black-free Mexico. It would have been interesting to discuss this body of work with Black visitors to the Museum of Fine Arts, but I didn’t see any during my three hours there.
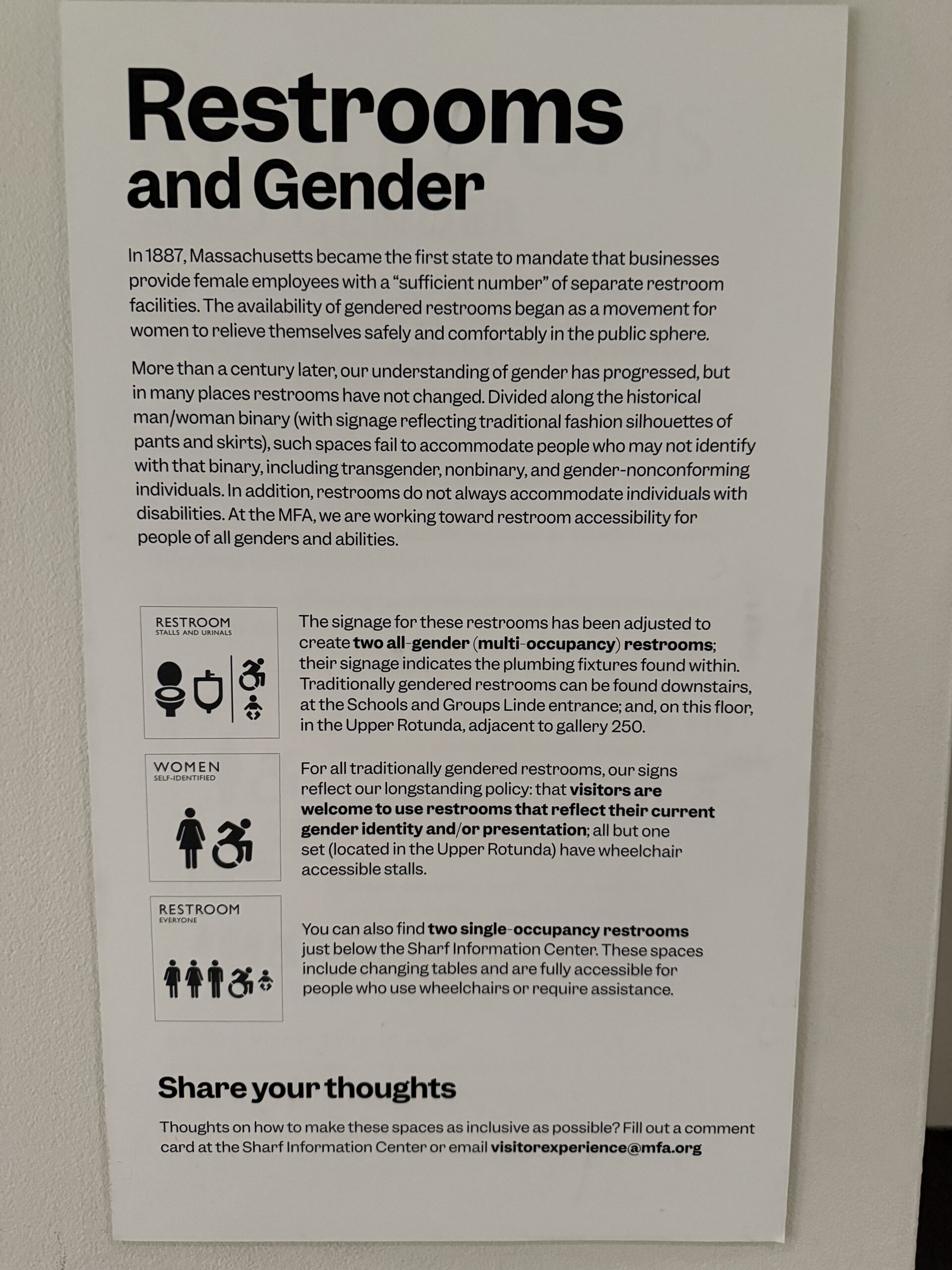
I posted the following on Facebook with a prefix of “Team of Harvard PhDs labels two bathrooms:”
(A loyal reader here and on Facebook pointed out that the discourse on restrooms and gender should properly be posted in multiple languages and also Braille. Given the recent influx of migrants to Maskachusetts, why not versions in Arabic, Haitian Creole, and Spanish?)
A Trump-hating, Musk-hating, Hamas-loving MIT PhD read the “Team of Harvard PhDs” prefix literally:
I don’t see any evidence of Harvard or Ph.D.’s being involved. Is it safe to assume that you are just making that up, or do you actually have information related to that? (For non-Bostonians, it’s worth noting that Phil is having his hissy fit at the MFA, which is not affiliated with Harvard… and is not even particularly close to Harvard)
A Manhattan-based immigration/asylum profiteer responded
Who cares.
to which I followed up with
who cares? How about the intellectual elites who wrote the epic-length sign depicted above? … like Jeffrey Epstein, that sign didn’t hang itself. And I don’t think it wrote itself either!
(The idea is that people who follow Joe Biden’s example and fly the trans-enhanced Rainbow Flag don’t actually care about Rainbow Flagism?)
Over lunch, my Boston-based friend (highly educated and paid) said that all of the young people in Gaza should be entitled to move to and live forever in the U.S. When I asked why those who attacked Israel get priority over poor, sick, disabled, and elderly folks in the poorest African countries, she said that they too should be able to move to the U.S. In fact, “I don’t think countries or borders should exist.”