[February 11 update: Only five days later, some more data… “It works: 0 deaths, only 4 severe cases among 523,000 fully vaccinated Israelis” (Times of Israel, but no information in the article regarding how old and/or sick this population of 523,000 folks was (maybe the kinds of folks who are typically killed by COVID-19 are not part of this HMO)).]
Israel is mostly vaccinated at this point, yet the coronaplague is subsiding at only roughly the rate we’d expect for a country in lockdown. (Israel went into its third lockdown in December and, of course, the country is fully masked as well.)
Here are some charts:

Shouldn’t we expect a discontinuity in hospitalizations if the vaccine is working as advertised?
How about deaths, the most reliable statistic?
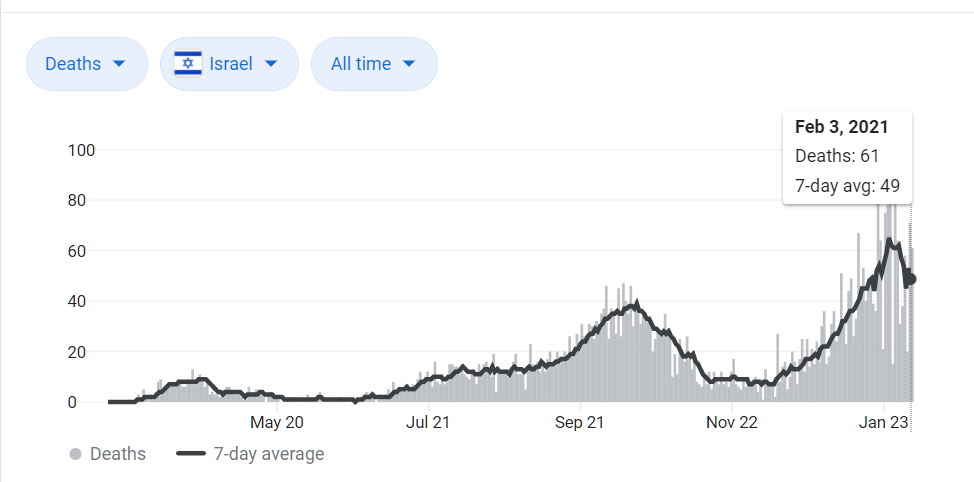
How do we explain these banal curves given the widespread use of the revolutionary plague-ending vaccine?
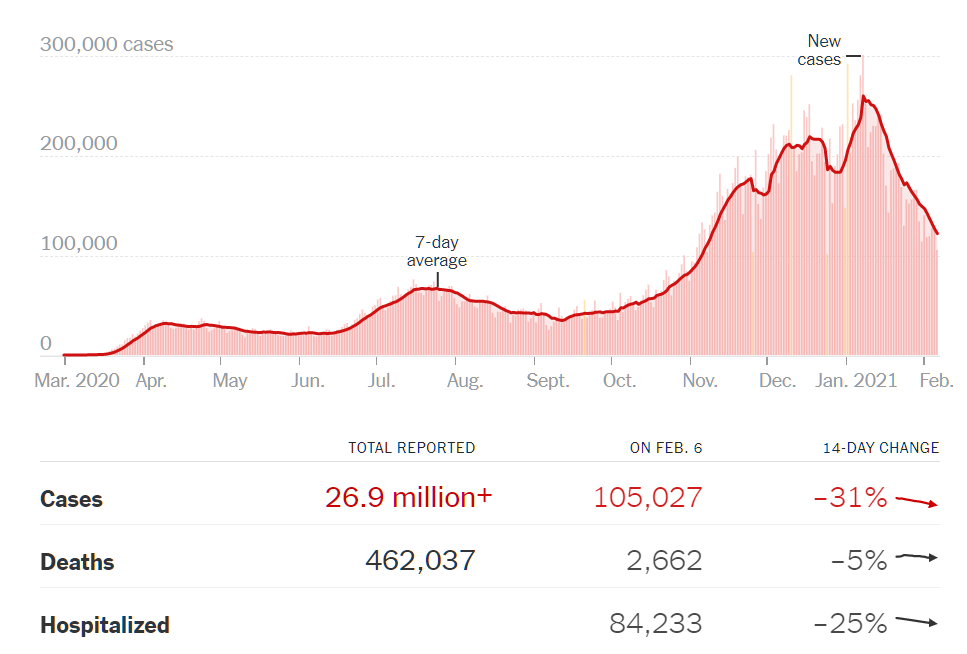
For comparison, how about the U.S. case count, plunging since January 1, 2021 despite no changes in policy or significant numbers of people vaccinated (from NYT):
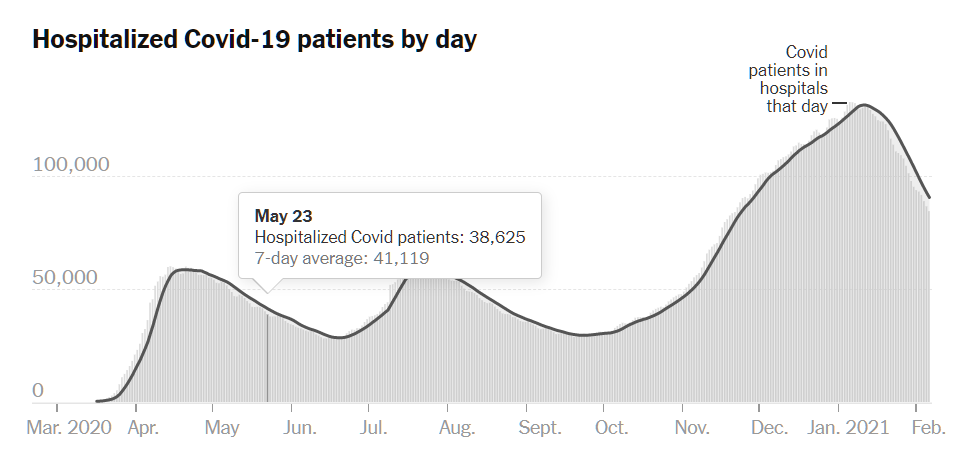
And the plunging hospitalizations, which presumably should lead to a plunge in deaths (since the only thing worse than death is death without Medicare being billed for a hospital stay):
Related:
- If COVID-19 vaccines weren’t tested on likely COVID-19 victims, how do we know that they will reduce COVID-19 deaths? (December 27, 2020)
- NYT regarding Israel: “The new Israeli research looked at national health statistics for people 60 years and older, who received the Pfizer-BioNTech vaccine first because of their high risk. Analyzing data from six weeks into the vaccination campaign, when the majority of people that age had been vaccinated, they found that the number of new Covid-19 cases dropped by 41 percent compared to three weeks earlier. That group also experienced a 31 percent drop in hospitalizations from the coronavirus, and a drop of 24 percent of those who became critically ill.” (i.e., despite a national lockdown, they had 76 percent as many “critically ill” among their newly vaccinated population compared to the no-lockdown no-vaccine situation).
- Don’t share this on Facebook… “Facebook says it plans to remove posts with false vaccine claims.” (NYT, February 8): “Building trust and confidence in these vaccines is critical, so we’re launching the largest worldwide campaign to help public health organizations share accurate information about Covid-19 vaccines and encourage people to get vaccinated as vaccines become available to them,” Kang-Xing Jin, head of health at Facebook, said in a company blog post.
Great questions. Assuming the coronaplague does not kill us first, we will soon have empirical answers to these issues, and we will be better for it. Just don’t die first!
While there does appear to be an inflection point between between the 50% 1st (still positive slope) and 50% 2nd shot (getting a little better), it sure looks like a big part of the answer is: “Um, we’ll have to circle back around to that later. New data is emerging all the time.”
It sure looks to me from this data that the vaccine is about half as effective – maybe less – than initially stated.
Philg – you may have to look at the data out of Israel in a little bit more detail. There seems to be information on how many people who have been vaccinated have tested positive vs. control groups who have not etc. etc. I think VOX just had some article on it but I’m too lazy to look it up and post the link.
If this vaccine stuff is so useless why did you get it?
I overcame my laziness:
https://apple.news/AF-Nqfg8ORB-R1AwMh66gzg
LP: Nobody said “this vaccine stuff is so useless”. You can be a righteous True Believer and still be interested to know how well the vaccines work. See https://www.mass.gov/info-details/covid-19-travel-order for example: “At this time, vaccinated individuals must continue to comply with the Governor’s Travel Order and related testing and quarantine requirements. While experts learn more about the protection that COVID-19 vaccines provide under real-life conditions, it will be important for everyone to continue using all the tools available to us to help stop this pandemic, including quarantining after a possible exposure, covering your mouth and nose with a mask, washing hands often, and staying at least 6 feet away from others.”
(i.e., the reporting, testing, and quarantine rules for those who’ve traveled outside of Maskachusetts are the same for the vaccinated and the unvaccinated, just as though the vaccine has zero value)
Separately, even a person who believed that the current vaccines are useless would still have good reasons to get one. The WHO said that masks for the general public were useless, but it is still useful for someone who follows the WHO’s scientific opinion to wear a mask because otherwise he/she/ze/they cannot go into a grocery store and get food. Presidents Biden and Harris, as well as governors in those states that currently require masks, will almost surely tell people “You’re free not to get the vaccine. It is just that you can’t leave your house or send your children to school unless you’ve been vaccinated.” So… unless you think that the vaccine is going to kill you, it makes sense to get vaccinated even if you don’t think that the vaccine will do anything to discourage the constantly evolving coronavirus.
https://pandemicpondering.com/2021/02/06/israels-vaccine-success-is-the-best-news-of-the-pandemic/
“Data presented in a series of tweets by Eran Segal from the Weizmann Institute and now presented in an unreviewed manuscript, show that vaccination has impressively reduced new infections and hospitalizations in Israelis over age 60.”
Note similar graphs but the ones in the link have a different vertical axis (percent vs total numbers).
Eran Segal is good on Twitter for this sort of thing:
“Nationwide, drop in the fraction of cases, hospitalizations, and critically ill in people 60 years old and above (who were prioritized first for vaccination) out of all age groups
These patterns were not seen in the 2nd lockdown (Oct.)”
https://twitter.com/segal_eran/status/1358154823590416387
Isn’t it too early to look at nationwide data?
A vaccinated individual has to prime enough antibody-producing cells to make enough antibody to produce an effect on viral growth before any survey can detect an effect. Surely it is too soon for the injected population in Israel to be exhibiting enough antibody to produce a population-wide effect detectable by virus-induced illness counting?.
Bernie: I hope you aren’t going to dispute #science and get deplatformed!
“The coronavirus vaccine made by Pfizer and BioNTech provides strong protection against Covid-19 within about 10 days of the first dose, according to documents published on Tuesday by the Food and Drug Administration before a meeting of its vaccine advisory group.”
https://www.nytimes.com/2020/12/08/health/covid-vaccine-pfizer.html
But maybe this is part of the upsell process.
If we shut down for 3 weeks that will flatten the curve and avoid overwhelming our health care system.
The shutdown should be 8 weeks or until there is a vaccine, which will end the pandemic.
Everyone should wear masks indoors and a lot of stuff, e.g., unionized public schools, should remain shut indefinitely.
Everyone should wear masks indoors and outdoors.
Everyone should be vaccinated because it will end the pandemic, but we should continue with shutdown and masks until everyone is vaccinated.
We can’t be sure how well the vaccines work, so we should continue with masks and shutdown even after everyone has been vaccinated.
The people receiving vaccines so far are largely elderly shut-ins.
The average person who gets infected with covid spreads the infection to perhaps 2.0 other people. But lots of people underestimate the heterogeneity in the spread rate. We are vaccinating people with below average spread rates.
Given the disparate health effects, it makes sense to prioritize vaccination for elderly who live in group settings or have caregiver dependency. Beyond that it would be smarter to use a military draft strategy. Every day, draw two birthdays out of a bowl and add people born those days to the vaccine eligibility.
If the goal is to get the virus to subcritical levels, it’s smarter to mix the “buffer solution” uniformly into the hot zones, than to apply a severely stratified strategy. The latter probably delays subcriticality into July instead of May.
It’s interesting. I think what we should have done is vaccinate the spreaders first, in large, densely-populated urban areas. The healthcare people who interact with the elderly, but not necessarily *all* the elderly themselves. If you want to slow the spread, you begin with the people who are spreading it.
The elderly in health care setting like nursing homes and assisted living facilities, in other words, should not have been the first priority, and especially not prisoners. Instead, we should have vaccinated all of the health care and prison *workers* first. People who live in nursing homes and assisted living facilities do not go out and wander around contracting the virus. They are already self-isolated. So the smarter strategy would have been to keep them isolated while making sure that 100% of the people who interact with them got their shots *first*. This has been a big problem because lots of people in those facilities have *refused* to be vaccinated. In the meantime, we can congratulate ourselves for having vaccinated X percentage of the elderly – but what good has it really done?
In the UK, the JCVI are in charge:
“Given the current epidemiological situation in the UK, the best option for preventing morbidity and mortality in the initial phase of the programme is to directly protect persons most at risk of morbidity and mortality.”
https://www.gov.uk/government/publications/priority-groups-for-coronavirus-covid-19-vaccination-advice-from-the-jcvi-30-december-2020/joint-committee-on-vaccination-and-immunisation-advice-on-priority-groups-for-covid-19-vaccination-30-december-2020
It’s probably clearer with a fuller quote:
“Direct protection vs transmission reduction
JCVI has considered a number of different vaccination strategies, including those targeting transmission and those targeted at providing direct protection to persons most at risk.
In order to interrupt transmission, mathematical modelling indicates that we would need to vaccinate a large proportion of the population with a vaccine which is highly effective at preventing infection (transmission). At the start of the vaccination programme, good evidence on the effects of vaccination on transmission will not be available, and vaccine availability will be more limited. The best use of available vaccine will also, in part, be dependent on the point in the pandemic the UK is at.
Given the current epidemiological situation in the UK, the best option for preventing morbidity and mortality in the initial phase of the programme is to directly protect persons most at risk of morbidity and mortality.”
In May, the UK will switch to the Phase 2 groups (those less at risk, probably emphasise those more likely to transmit).
@Alex: Note Indonesia is doing the young first.
https://www.aljazeera.com/news/2021/1/13/young-people-first-indonesias-covid-vaccine-strategy-questioned
But it appears mostly because of lack of clinical data for those over 60.
Israel is actually *not* mostly vaccinated, or even close: the headline figure of almost 60 doses per 100 people hides the fact that only 37% of the population has gotten even one shot, with only 22% having completed both shots. And it takes about two weeks after the shot for immunity to rise.
The link cited by Paul, above, says that, as of February 2, “88.9% and 77.7% of individuals older than 60 years old had received the first dose or both doses of the vaccine, respectively, or recovered from COVID-19.” We’re looking at only the data for those over 60 (folks under 60 are very seldom killed by COVID-19).
Alex, I disagree on the nursing homes because the vaccines aren’t 100% effective and all it takes is one infection to spread to dozens of other elderly, with high attendent hospital costs and death rates. Perhaps there was a third way, to spread them out more or improve ventilation systems, but it’s too late now.
For younger folks, it’s sort of an interesting math and behavior problem figuring out optimal vaccine strategy. The spreaders are going to be mostly single people in their 20s and 30s, but there’s also a moral hazard problem setting loose the most carefree with early vaccination when no one else is protected.
Vaccinating people essentially at random is probably close to optimal. Most spread happens at home, second most at work. If half of a household (or workplace) gets vaccinated, that cuts spread enormously. Vaccinating the second half of a household doesn’t add so much.
I doubt we see a big impact on cases until half of the 20-49 set is vaccinated. But at least the hospitalizations should plunge over the next two months with elderly prioritization.
@Steve: You might enjoy this article:
https://www.wired.com/story/covid-19-vaccine-super-spreaders/
Fascinating discourse (scroll down a bit) on finding the superspreader ‘nodes’.
So maybe the Covid is not the reason we are seeing our death rates go up, but something else is going on. Covid-19 is just a ubiquitous cold virus along for the ride and it is being set up as a patsy for a whole host of other intersecting health emergencies, like racism and climate change (heh). It turns out that the promise of ever-increasing long life was a lie. The years of a man are seventy, and after eighty he is done. The best things you can do for your health is to have good habits, better genes, and a spouse of indifferent quality.
Avoid doctors to cure the effects of age — there is no cure for the necessary natural process of senescence and death. Avoid doctors to treat the symptoms of your bad habit of gluttony, like diabetes and high blood pressure, Avoid doctors to give you pills because you are sad because you do not have the companionship of a wife. Avoid the advice of doctors that would prescribe the same course of treatment for you as they would for anybody and everybody else. Avoid doctors who demand your obedience to their authority. Avoid doctors who want to control the most intimate matters in your life. Avoid doctors who want to turn civil society into a prison state.
I’m okay with dying at 74 instead of 75 if it means I can get on with my life.
Another slightly skeptical take:
https://www.unz.com/isteve/is-this-what-good-news-looks-like/
Thanks, Don. You inspired me to update the original post with the U.S. curves, which have been plummeting since January 1 despite no new lockdown and no significant number of vaccinated people. If coronascience is, in fact, a science, why weren’t the scientists able to predict the dramatic collapse in U.S. cases? Ask a physicist where an orbiting object will be in two months and he/she/ze/they will be able to give you a great prediction.
Phil, yes, great questions. The virus seems to ‘behave’ somewhat chaotically, and it’s spread sometimes seems to be turbulent. I’ve also noted that when it ‘surges’ or when it collapses, lots of hindsight hand waving goes on to explain what happened, as if he/she/ze/they knew what happened.
Phil, if you looked at the midwest epidemic curve and shifted it two months to the right, you would have successfully predicted the national epidemic curve.
The beauty of the epidemic (thinking of the Wired article) is that it heavily favors “innoculating” the social butterfly nodes. The problem with the epidemic is that it generally favors only certain vectors, so the herd immunity is less robust than if acheived through vaccination.
What do I mean by “certain vectors?” The New York wave was largely a global travel wave, spreading through airports, business conferences, and ski chalets. It affected the wealthiest enclaves, like Milan, New York, Boston and San Francisco. But it also burned out quickly since global travelers are also zoomers and home owners.sdfsd
The sunbelt wave was an uncertain mix of air conditioning (poor ventilation) and Latin American migration. That too burned out, thanks to the shortness of a/c season and the insularity/youth of migrant farm work.
The fall wave was the first normal epidemic/pandemic wave. Covid was finally well-mixed into society and truly endemic. The epidemic followed the traditional arc of cold dry weather, short days, and vitamin D deficiency.
There’s still risk of another wave, but it would probably follow a new vector caused by relaxed distancing like colleges or concerts. Or hold off until next fall when seasonal respiratory viruses return.
Steve: On my recent Florida trip I found some clubs outside of which it would have made obvious sense to set up a vaccine injection desk! (on the other hand, maybe most of those club-goers have already been exposed and are immune)
Israel has a unique issue: the ultra-Orthodox Jews. In an interview I heard Michael Oren (Israeli politician/historian) say that the u-O mostly refuse the vaccination, believing everything is in the hand of God and the works of man are irrelevant. While making up 10% of the population, they are upwards of 60% of hospital cases.
Sounds like the same point of view as Phil’s.
Dubious that the Haredim “mostly refuse the vaccination.” First, the Haredim are not monolithic — though to you they may appear to be. Second, a quick google search will lead to lots of articles to the contrary with Haredi leaders urging their followers to get vacinated. Seems you have the Haredim confused with the Christian Scientists.
Randall: Are you sure that this isn’t just a local variation on the general principle that some other group is always to blame for a problem? Rich white Californians blame “Latinos” (see https://philip.greenspun.com/blog/2020/12/29/assumption-that-masks-are-effective-leads-to-conclusion-that-people-of-color-are-responsible-for-coronaplague/ ). Secular Israelis blame the observant.
(Nit: the Haredi are now 13 percent of the population; see https://www.timesofisrael.com/haredi-population-growing-twice-as-fast-as-total-israeli-population-report/ )
https://www.cnn.com/2021/01/29/middleeast/israel-ultra-orthodox-coronavirus-intl/index.html says that the ultra-Orthodox are poor and live in large crowded households. The poor in the U.S. also have a much higher rate of plague than the rich. That said, the stats aren’t so exciting: “The rate of Covid-related deaths in people over 65 among the ultra-Orthodox was estimated last December to be about 3.6% higher than the Israeli norm, according to the Ministry of Health.”
How bad is a 1.036X higher risk of death? https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-race-ethnicity.html says that Being Americans While Black carries a 2.8X higher risk of COVID-19 death (ditto for being Latinx).
Jack: I am not saying that an omnipotent god has chosen whom to kill via COVID-19. And I wouldn’t say that all of the “works of man are irrelevant” against a virus that is continuously evolving. Skepticism regarding using a bandana as PPE would not have been considered a religiously motivated belief a year ago.
Jack: It’s not my confusion! I’ll take Oren’s word for it on the numbers. He lives there and is heavily involved in their politics and journalism – an ex-member of Knesset and was in cabinet and was Deputy Prime Minister.
That’s a “name a group” game. Most common count for ultra-orthodox is at 17% of Israeli population, some cite other percentage. They are not a monolith group, most of leading rabbis of theirs issued orders to vaccinate to their followers and even some issued orders that those who do not vaccinate act against the Lord. They can not account for most of the hospitalizations as their population is heavily shifted towards officially non-vulnerable majority of non-vulnerable children, youths and young adults; the highest estimates I have read that Orthodox represents 1/4 of all tested positive coronavirus cases in Israel. Again, this label covers very distinct groups with different modes of interactions with society as a whole.
A vaccine does not protect against false positives in the ridiculously inaccurate RT-PCR tests.
Tomas Pueyo has a new article out which has a pretty good explanation of what might be going on in Israel and elsewhere.
https://tomaspueyo.substack.com/p/variants-v-vaccines?utm_campaign=post&utm_medium=email&utm_source=copy
Hmm, maybe the vaccine does work? Not nearly as inflammatory as “all the so-called experts suck” but interesting nonetheless.
https://www.wsj.com/articles/israeli-data-shows-94-drop-in-symptomatic-covid-19-cases-with-pfizer-vaccine-11613401510?st=ok2m96qllqz2u7y&reflink=article_copyURL_share