Karen visits a Florida theme park
This is a quote from a friend’s Facebook post, but I am not going to use the WordPress Quote style because it will be easier to read if not in italics. The names have been changed. The author is a professor who lives in a Biden- and Fauci-supporting town. Any similarities to Confessions are purely coincidental… (and let me just state for the record that the author is a far smarter and nicer person that I have ever been!)
I’ve made what might have been the single worst error of judgment in my 40 years of life. If any good will come of it, it’s only in the confession and warning that I now feel morally compelled to give my friends.
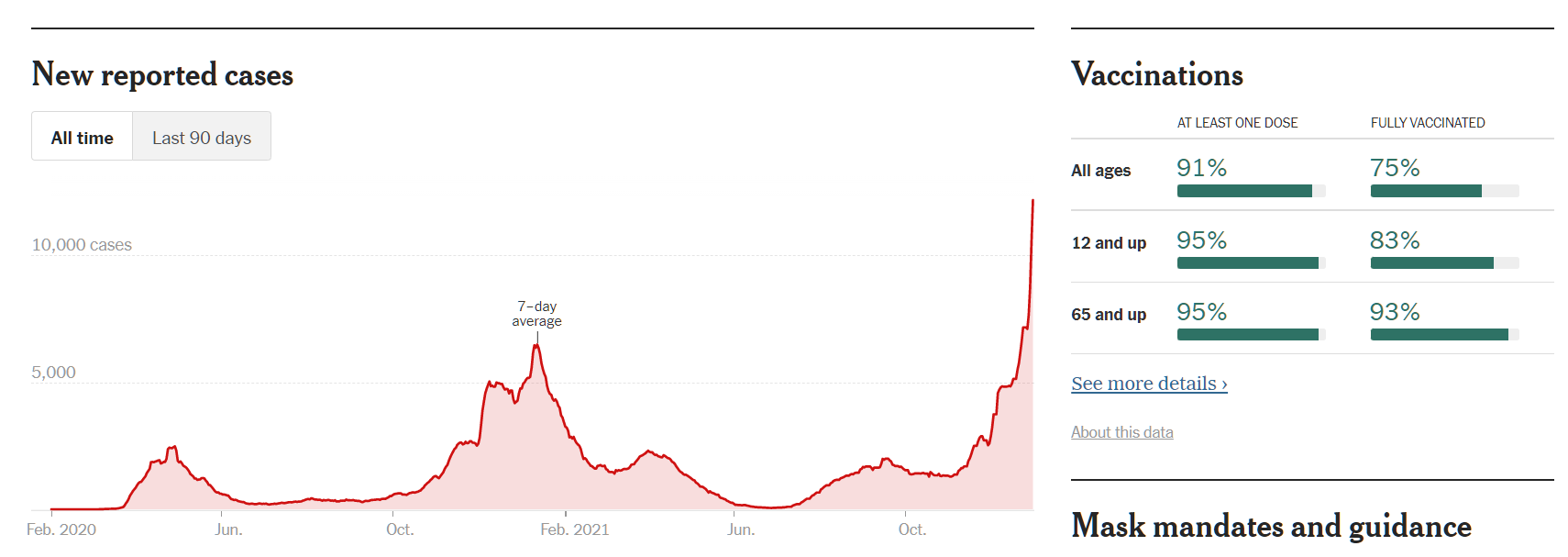
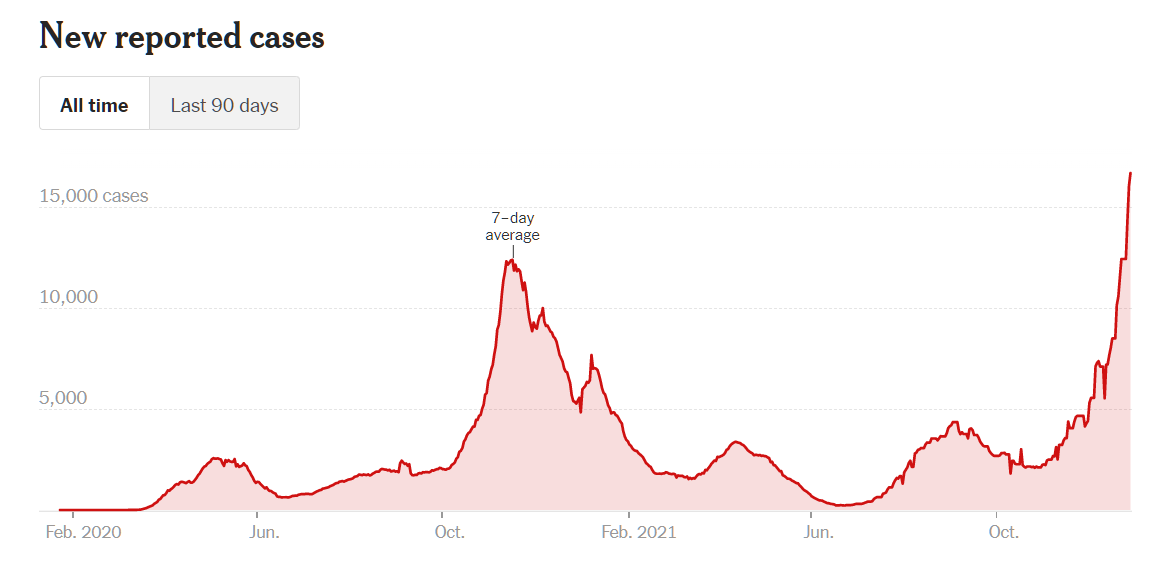
One month ago, my 8-year-old daughter [Alice], who just finished the Harry Potter series, begged to go to Universal Studios in Orlando over Christmas break to see their Harry Potter park. It seemed like a good time: Alice (and her 4-year-old brother [Robert]) hadn’t enjoyed any trip of this kind since before the pandemic, Alice at last would finally be vaccinated, [wife] and I had just gotten our booster shots, Delta was in retreat, and covid numbers were actually extremely low in Florida. Plus we figured it would be mainly outdoors, and we’d mask, and [wife] found a website claiming it wouldn’t be very crowded on the dates we wanted to visit.
So I plunked down a few grand for (non-refundable) tickets. And then, literally the next day, we learned about the Omicron variant from South Africa. And to my eternal shame, I didn’t cancel the trip, despite my understanding of exponential growth. I couldn’t bear to face my daughter and tell her she wasn’t going after all, nor could I bear to face my family and tell them the planning and money were all wasted.
So now we’re here. And the reality is: it’s crowded as hell — one of the most unpleasant, sardine-packed places I’ve ever experienced in my life, before or during covid. The majority of guests (and even many employees) are unmasked. It’s mostly indoors. For every single ride, you stand for more than an hour in cramped, enclosed waiting areas while hordes of unmasked people breathe on you. It’s obviously an Omicron superspreader site. Indeed, the chances that one or more of us caught it today are EXCEEDINGLY high. Plus … it’s not even fun, like Disney World is. It sucks. Just endless lines, crowds, ripoffs, and uninspired rides.
Many of the rides play jokey recorded audio messages about how the ride is so terrifying, how much danger you’re in, phew you survived it, etc. etc. All those messages now take on new, unapproved meanings.
From the minute we arrived, I started saying “we have to leave this place, we have to leave, WE HAVE TO LEAVE NOW” — and yet, I’m ashamed to say, it took us 5+ hours to do so. I kept deferring to the … err … majority vote among my family, that we shouldn’t make a TOTAL loss of this trip, and surely we can find something here that’s relatively covid-safe?
Our mistake did, at least, give me perhaps my first opportunity of this entire pandemic to stare directly into the heart of the half of the country for which the virus might as well not be real — and I found the view absolutely terrifying, and it’s given me a new, visceral understanding for how we managed to lose 800,000+ Americans, and that understanding will stay with me as long as I live.
I’m sorry to everyone for whom I was a bad example. I’m sorry to everyone who my family might have endangered. Please learn from our mistake.
In the meantime, do any of my friends have suggestions for what to do for the rest of this trip? (Where one possibility is, “take the next flight back to [cozy Deplorable-free university town] and never look back”?)
ADDED: [wife] wanted me to emphasize how Universal Studios is endangering lives for greed, by packing people way, WAY more densely than can possibly be safe.
Alice [the 8-year-old], alone among us, actually enjoyed the park (!) and wants to return to it tomorrow.
Thus endeth the Confessions of Karen. The Confessions of Greenspun begins here…
I’ve made what might have been the single worst error of judgment in what feels like nearly 100 years of life. If any good will come of it, it’s only in the confession and warning that I now feel morally compelled to give my friends. I purchased an annual pass to Legoland Florida (Winter Haven, just south of Orlando) and we decided to visit during the beginning of the two-week Florida Christmas school vacation.
The park is nowhere near as crowded as Disney (think suburban shopping mall on a Saturday versus Times Square on a Friday night), but we didn’t know what to expect so I paid up for the $90/day skip-the-lines band ($60/day during non-peak periods). Unlike Professor Karen’s experience at Universal, above, we found that we almost never needed to be indoors to enjoy Legoland. Most of the lines, which we skipped in any case, were outdoors. The park recommends masks when indoors, but the core customer base seems to be Floridians and therefore hardly any of the visitors were masked, indoors or out.
Our 6-year-old loved the water ski show so much that Senior Management needed to sit through two repeats.

If you thought that COVID-19 was bad, it is only because you haven’t been on Mia’s Riding Adventure. “Many of the rides play jokey recorded audio messages about how the ride is so terrifying, how much danger you’re in, phew you survived it, etc.,” said Professor Karen (above). If I could take over as dictator of the U.S. and thus were able to force Legoland to install such a message, it would start with “How much would you enjoy it if your first horse ride were as a jockey in the Kentucky Derby at 37 mph?” and then note that the ride was best suited for those who booked all of their coast-to-coast flights on the Vomit Comet. (Recommendation: Try the Dragon rollercoaster, which is not too violent and which starts with a flat slow tour through some fun LEGO scenery.)
The San Francisco miniature is not consistent with Reading list: San Fransicko. There wasn’t a single homeless encampment on any of the LEGO sidewalks. There was no open-air drug market.

Miami Beach without a traffic jam of Lamborghinis, Rolls-Royces, and Ferraris?

If you split your time between 12th Street and Haulover beaches, this might be the souvenir to bring home:

(One of my worst days since moving to Florida was at clothing-optional Haulover beach. Everything was awesome until some wag called Marine Mammal Rescue and they showed up at my blanket with a whale sling.)
Not every visitor was Deplorable. Here is a fully masked family:

They’re walking by a bust of a notorious racist (also known for popularizing Mileva Marić‘s explanations of the photoelectric effect, Brownian motion, and conversion of matter into energy) made out of 500,000 Duplo bricks.
Short summary of my friend’s theme park experience and our own family’s: I’m not surprised that Floridians, who never entered the Covid Olympics and therefore don’t care which medal they win, show up to parks. But I am surprised that anyone who supported school closures, mask orders, and other Covid-related restrictions will show up (this is about half of Americans, so the parks should be at least half empty!). And I am truly shocked that the federal government allows the parks to remain open (also, the Super Bowl; why?). From Disney World during Code Orange coronapanic (September 2021):
(According to #Science, COVID-19 is a sufficiently serious public health issue that schools have been closed (for 1.5 years in our big cities) and/or children are made to wear masks 7 hours per day while also forgoing normal interaction (American kindergarten is now set up more like high school detention; kids must sit at their individual desks and not get close to other kids… while also wearing masks). If we are losing life years, contrary to Social Security and life insurance financials, the only sensible #Science-informed policy would be a presidential order shutting down all American theme parks. Pulling together 200,000+ people per day at Disney World (all four parks combined) means pulling together people in airliners (most of the folks we met had flown there), in restaurants, in hotels, etc. Even if they don’t get infected while on a roller coaster, they’re a lot more likely to get infected than if they’d stayed home, which remains the best demonstrated method of cutting one’s infection/transmission risk (our best vaccines can cut infection/transmission in half right now?). As a society we’ve determined that it makes sense to deny an education to millions of children if just one life can be saved. Shouldn’t the same logic apply to theme parks? If child can wait 1.5 years to learn, why can’t adults and children wait until the pandemic is over to ride a roller coaster?)
Related:
- Covid Karen (why it is not a gender-specific term)
- If at least 50 percent of us are Covid-righteous, how did hotels and flights fill up with leisure travelers?
- After telling others to wear masks, the Democrats’ thought-leader Alexandria Ocasio-Cortez enjoys a mask-free vacation in Florida (Daily Mail)