This is kind of fascinating… the New York Times, which was a principal cheerleader for lockdowns, now complains about American public schools having been shut for roughly one year… “The School Kids Are Not Alright” (NYT, August 22):
One of the most distressing aspects of the Covid pandemic has been seeing governors and state education officials abdicate responsibility for managing the worst disruption of public schooling in modern history and leaving the heavy lifting to the localities. Virtually every school in the nation closed in March 2020, replacing face-to-face schooling with thrown-together online education or programs that used a disruptive scheduling process to combine the two. Only a small portion of the student body returned to fully opened schools the following fall. The resulting learning setbacks range from grave for all groups of students to catastrophic for poor children.
From the start, elected officials seemed more concerned about reopening bars and restaurants than safely reopening schools that hold the futures of more than 50 million children in their hands.
Could this be the new definition of chutzpah? (replacing the former “that quality enshrined in a man who, having killed his mother and father, throws himself on the mercy of the court because he is an orphan.”)
The rest of the editorial is about new ways for President Biden to force every American schoolchild to wear masks for 7 hours per day. Having bravely confronted the Taliban, Uncle Joe will now turn his post-nap attention to K-12ers who are wearing chin diapers, under-nose masks, or running wild:
President Biden took the right approach on Wednesday when he announced that his Education Department would use its broad authority to deter the states from barring universal masking in classrooms.
How much difference will this make? See “The Science of Masking Kids at School Remains Uncertain” (New York, August 2021):
At the end of May, the Centers for Disease Control and Prevention published a notable, yet mostly ignored, large-scale study of COVID transmission in American schools. A few major news outlets covered its release by briefly reiterating the study’s summary: that masking then-unvaccinated teachers and improving ventilation with more fresh air were associated with a lower incidence of the virus in schools. Those are common-sense measures, and the fact that they seem to work is reassuring but not surprising. Other findings of equal importance in the study, however, were absent from the summary and not widely reported. These findings cast doubt on the impact of many of the most common mitigation measures in American schools. Distancing, hybrid models, classroom barriers, HEPA filters, and, most notably, requiring student masking were each found to not have a statistically significant benefit. In other words, these measures could not be said to be effective.
In the realm of science and public-health policy outside the U.S., the implications of these particular findings are not exactly controversial. Many of America’s peer nations around the world — including the U.K., Ireland, all of Scandinavia, France, the Netherlands, Switzerland, and Italy — have exempted kids, with varying age cutoffs, from wearing masks in classrooms.
(As with physics, e.g., Katherine Clerk Maxwell‘s equations, the predictions from coronascience will be different depending on the country in which the experiment is conducted.)
Another interesting media phenomenon is cheering for school districts that defy governors’ orders to reopen fully. See “How three school districts are defying state restrictions on mask mandates” (CNN) for example:
The debate over masks in schools has reared its head once again with the new academic year, and a handful of states have taken steps to restrict local officials’ ability to implement their own masking requirements, either through the governor’s office or state legislatures.
These restrictions — made despite guidance from the US Centers for Disease Control and Prevention recommending masks for everyone in schools regardless of vaccination status — have prompted showdowns between state officials and some local school districts, who say they’re trying to protect their communities, particularly students who are ineligible for vaccines.
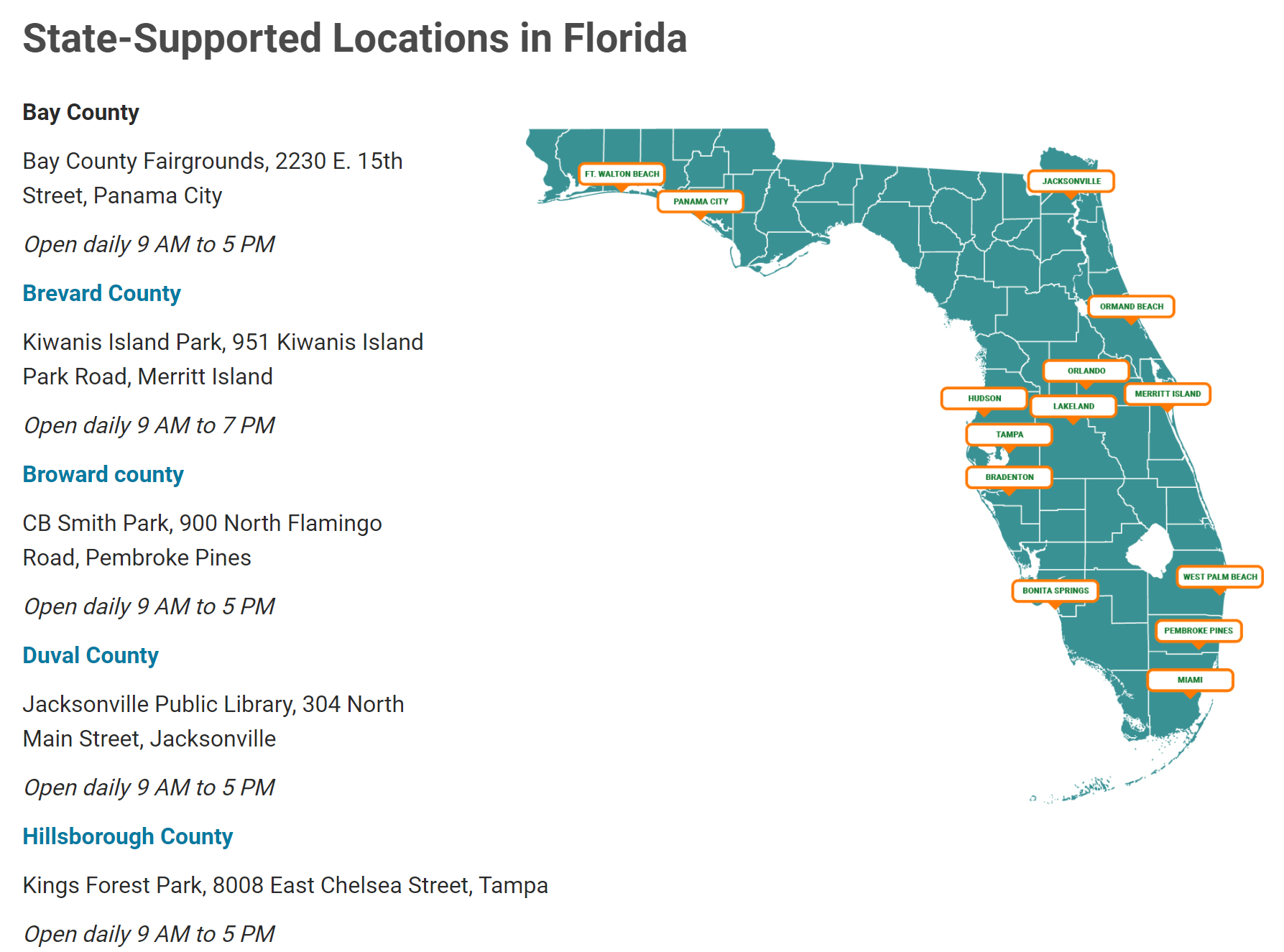
Perhaps most prominently, several Florida school districts have decided to impose mask mandates, defying an executive order by Gov. Ron DeSantis that forbids such requirements and threatens to take away school funding if school districts don’t allow students to opt-out.
But some school districts have taken more methodical approaches, carefully circumventing state restrictions on mask requirements through careful legal maneuvering or apparent loopholes.
The school bureaucrats’ motives are noble. They want to protect their communities and especially the children. The nobility of their motive is one reason that a governor’s order cannot apply to them.
What if, in April 2020, a school district in a rural area of a state had said “we’re reopening our school in defiance of the governor’s shutdown order because we are trying to protect our children’s future and ensure that they have enough education to thrive. We aren’t suffering from a plague the way folks in the big city who ride the subway to their Tinder dates are”? Would the same journalists have praised such defiance?
Full post, including comments