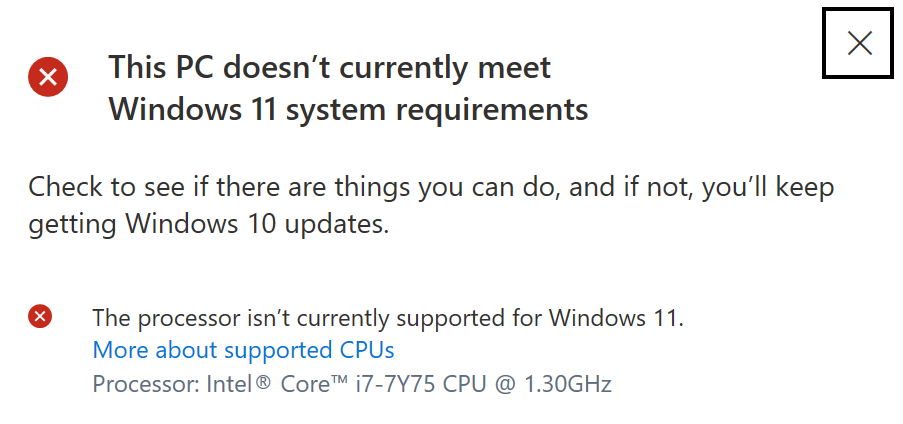
It is time to replace my 5-year-old Dell XPS 13. Despite multiple return trips to Dell for service, the computer has never worked properly, refusing to sleep when closed or even to sleep when “sleep” is selected from the power options at lower left (the only way to prevent the battery from being drained is “shutdown”). It lacks whatever mojo is required to run Windows 11:
I probably could have predicted this given that the machine runs out of CPU zorch on Zoom calls and warnings about compromised audio quality pop up. Also, having the camera at the bottom of the screen is an unbelievably bad idea for Zoom (others on the call will see your fingers as you type and, thinking that they’re on mute, will say “that guy has more chins than the Shanghai lockdown registry”).
The experience of being a Dell customer was traumatic, so I don’t want to repeat that. I’m not ready to abandon my love for all things Microsoft (the keyboard, the folding mouse, Windows itself) so I can’t join the young, hip, and stickered with MacOS. I haven’t enjoyed the 13″ screen, despite the high (3200×1800) resolution, but lugging a 17-inch laptop in the old days wasn’t fun.
[My 17-inch HP laptop died to support a worthy cause. A friend and I had it almost completely apart so that we could remove a failed component. Another friend walked in the door wearing a “women in STEM” T-shirt (“Maker Girl” or “Girls Code”?). She decided to assist us and, confused by a zero insertion force connection, rather than flick the male part out with a pinky, snapped the female portion off the main board (surface mount and therefore not field-repairable). (Are “male” and “female” terms for connectors obsolete in our 2SLBGTQQIA+ world? If so, what are the new names?)]
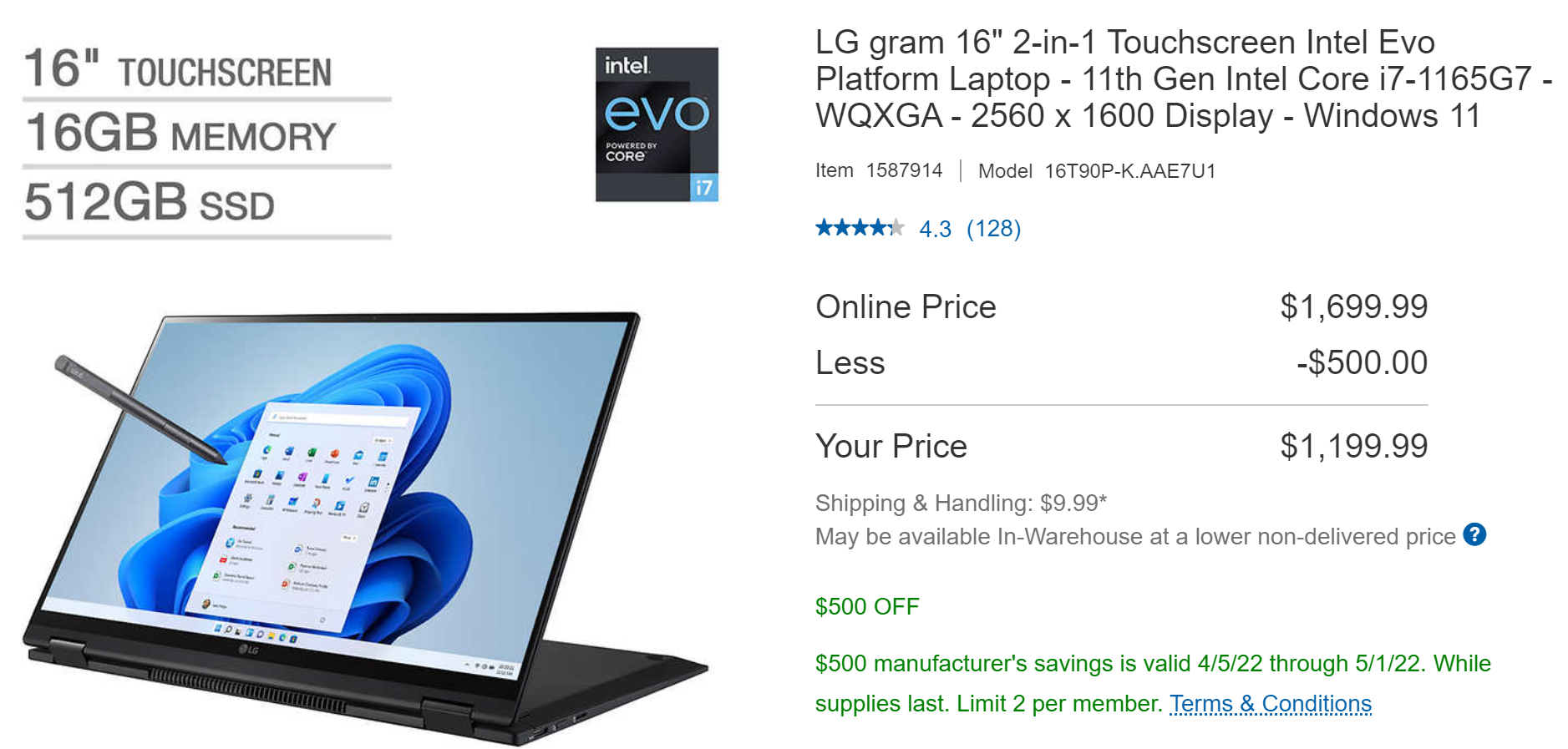
Back in 2019, I selected an LG Gram 17-inch laptop for Senior Management (see What laptop for Senior Management? and 17” laptop for seniors (note that Senior Management is not a senior!) and notice the lack of progress in specs; the LG Gram 17 had 16 GB of RAM, which is still the prevailing standard for higher-end laptops three years later). The machine is still functional, despite some abuse from the kids, and no tech support has been required either from LG or the Domestic IT Department (me). This machine will be used for travel and I like having a touchscreen, which LG still doesn’t make in a 17-inch version. So I am thinking about a 16-inch version. Last year’s model, which includes an 11th generation CPU, is marked down to $1200 at Costco (the newest 12th gen version isn’t quite available):
Given the feeble progress that I’ve noted in GPUs, for example, is there a practical difference between 12th and 11th gen Intel CPUs?
The Surface Laptop Studio direct from Microsoft is probably a great product, but the screen is only 14.4 inches in size. It is $1,550 with a 512 GB SSD (the minimum for me) and over $1,800 with the “i7” CPU. It also has the 11th gen CPU and a similar resolution (2400 x 1600).
What about gaming laptops for someone like me who mostly carries a machine into a conference room or a hotel room? Do they offer big advantages for sound quality, Zoom, etc.? I wouldn’t actually play games, though I would love to have (a) the time, and (b) the skill.
The old HP worked great until its encounter with Women in STEM and HP allows customers a certain amount of configuration flexibility. Maybe it is time to consider HP? Like LG, they won’t sell you a high-res 17-inch touchscreen, at least not on the Envy models. Maybe there is a conspiracy over in Asia to deny Americans 17-inch touchscreens? For $4,000+, HP will sell a laptop for “creators” with similar specs to the LG that I purchased in 2019: 16 GB of RAM and 256 GB SSD: HP ZBook Studio G8 Mobile Workstation. It has a 15.6″ screen.
I poked around on the Lenovo site and didn’t see anything comparable to the LG. They don’t seem to make 16-inch devices, for example, and their 17-inch laptop is low res (HD) and non-touch. Perhaps their specialties are 14-15-inch business laptops and gaming laptops?
Maybe this is why Apple is so beloved. Since they’re the monopoly hardware supplier, consumers don’t have to cope with a paralyzing array of choice.
Readers: Please help! I want to make sure that I have a good laptop in time for Hate Week in case I am traveling then! (prediction based on what I’m hearing right now here in Washington, D.C.: Ron DeSantis and Kathryn Kimball Mizelle will be featured)
(Separately, I tried using a supersized iPad and keyboard as a Windows substitute on one trip and was unsuccessful. I couldn’t figure out how to use Dropbox and Office 365 together effectively and found myself missing the Windows File System(!), despite having previously raged against the tyranny of a single hierarchy.)
Full post, including comments