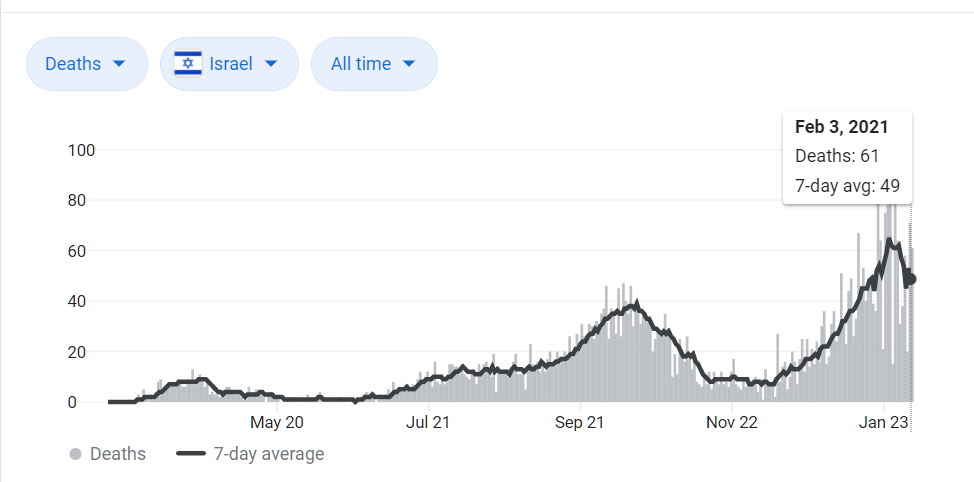
From yesterday’s post on Israel…
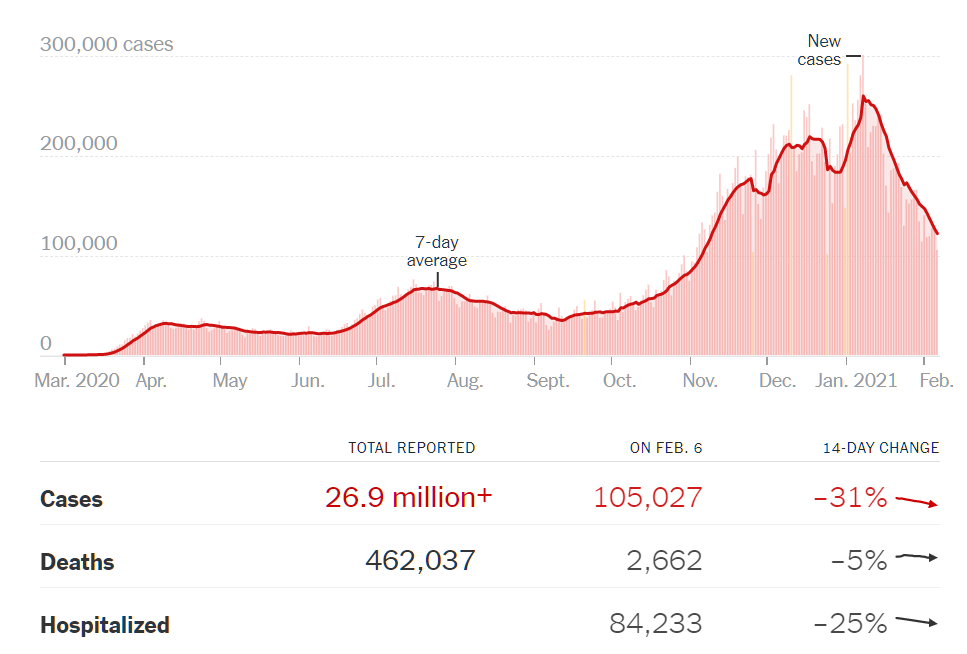
For comparison, how about the U.S. case count, plunging since January 1, 2021 despite no changes in policy or significant numbers of people vaccinated (from NYT):
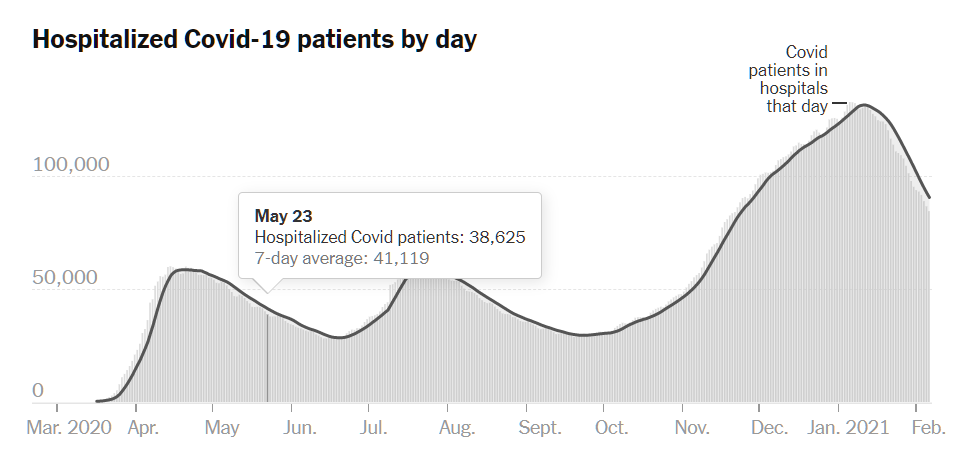
And the plunging hospitalizations, which presumably should lead to a plunge in deaths (since the only thing worse than death is death without Medicare being billed for a hospital stay):
Given that Americans did not change their behavior or policies during the time period covered, coronascience that is actually “scientific” should have been able to predict this peak and subsequent downward trend, right?
Let’s look at what our nation’s greatest scientist (at age 80), Dr. Fauci, said to state-sponsored media just a month before the peak. “Fauci Warns Of ‘Surge Upon A Surge’ As COVID-19 Hospitalizations Hit Yet Another High” (NPR, November 29):
“We may see a surge upon a surge,” Dr. Anthony Fauci, the nation’s top infectious disease expert, told ABC’s This Week on Sunday. “We don’t want to frighten people, but that’s just the reality. We said that these things would happen as we got into the cold weather and as we began traveling, and they’ve happened.”
With the December holidays just around the corner and more people traveling, “it’s going to happen again,” Fauci said. “We’re getting into colder weather and an even larger holiday season.”
The December holidays happened. More people actually did travel: “U.S. air travel reached post-March peak on day before Christmas Eve, TSA data shows” (NBC). Positive tests (“cases”) are half what they were when these superspreading travel events occurred.
From the Official Magazine of Trump Hatred (New Yorker, November 12, 2020)… “The Pandemic’s Winter Surge is Here,” by “Dhruv Khullar, a contributing writer at The New Yorker, is a practicing physician and an assistant professor at Weill Cornell Medical College”:
Unless we put mitigating measures in place, the coronavirus will spread, and sooner than we expect it will get out of control. The only way to avoid mass death is to move quickly and decisively, flattening the curve through masks, distance, testing, tracing, and lockdowns until a vaccine and therapies can avert the suffering caused by covid-19. Passivity is the enemy. The winter surge is here; we decide what happens next.
(Note that science-following humans are in charge of the virus: we decide what happens next.)
None of these things were done, except maybe in California and Maskachusetts, yet the surge that concerned the “scientist” dissipated, apparently due to factors unrelated to human actions.
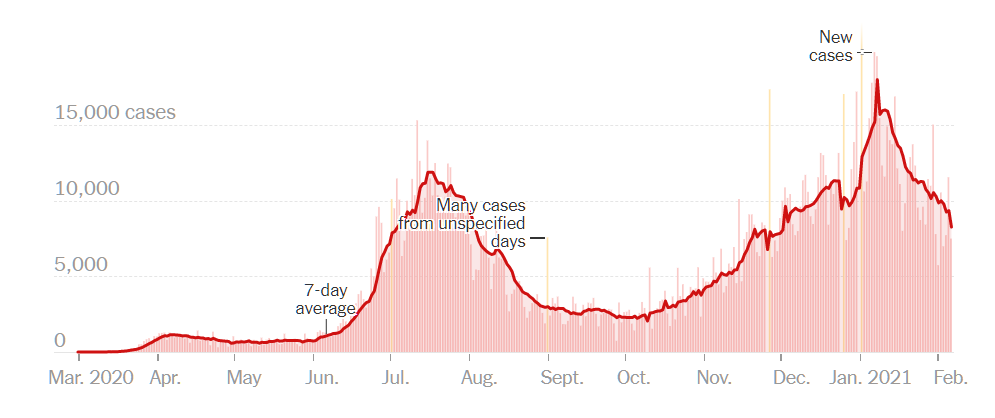
Here’s Florida “case” curve, with a decline starting just as the snowbirds arrived for Christmas:
Florida is a state with no mask law:
Florida recommends but does not require face coverings for the general public. Several cities and large counties, including Miami-Dade, Palm Beach and Hillsborough (which includes Tampa), have mask requirements, but local governments are barred from assessing fines and penalties for noncompliance under a Sept. 25 executive order by Gov. Ron DeSantis.
Floridians have rejected what the rest of us call science. Schools are open for in-person instruction (with some objections and lawsuits from science-following unionized teachers). Restaurants are open. Clubs are open. Offices are open. After-school sports for children are open and unmasked. People gather in large groups for social purposes. Even in supermarkets staffed by and catering to the elderly, workers and customers may be unmasked (CNBC). Here’s a January 2020 photograph from a club in Miami, in which people greeted each other with hugs and kisses:
If “scientists” failed yet again in their predictions, why are they still called “scientists”? What has distinguished astronomy from astrology, for example, is the superior predictive power of astronomy. Astronomy also gets better every year. Have we seen any improvement in the ability or people who claim to have scientific insight regarding coronavirus to predict epidemic statistics?
[My personal explanation for the plunge in U.S. “cases”: Back in October, Joe Biden promised that he would shut down the virus. What we’re seeing is simply President Biden delivering on his campaign promise a little earlier than expected (i.e., starting three weeks before taking power).]
Related:
- Did doom visit the Swedes yesterday as planned? (May 24: On May 3, in “Doom for the wicked Swedes is always three weeks away”, the IHME prophecy for Sweden was a peak in ICU usage on May 22 and a peak in deaths (494/day) on May 23. What actually happened? Yesterday’s WHO report showed 54 new deaths. The day before it was 40. In other words, the prophecy was off by a factor of 10. They were going to need nearly 4,400 ICU beds. The actual number in ICUs all around Sweden? About 340. In other words, the “scientists” were off by a factor of 13X.)
- How is coronaplague down in Brazil? (and the rest of the IHME predictions) (August 5; the June 10 prediction of the “scientists” was off by 10X).
Full post, including comments