Is U.S. immigration policy a form of animal hoarding?
People in the U.S. who say that we have a critical shortage of affordable housing and that income and wealth inequality are a “crisis” simultaneously say that we must keep our borders open to low-skill migrants, elderly and disabled migrants, and others who will never be able to pay a median rent. The people who observe that the U.S. health care system is unusable due to lengthy waiting lists and capacity shortages also say that we should bring in child migrants with diseases that will entail months of hospital stays (at a cost of $millions and with a result of extending waiting lists for native-born Americans; see, by contrast, Australia).
Let’s compare this to animal hoarding, as explained by the Minnesota-based Animal Humane Society (I picked Minnesota because the noble citizens there are passionate about importing as many Somalis as possible, regardless of education level or propensity to work):
Animal hoarding is an accumulation of animals that has overwhelmed a person’s ability to provide minimum standards of care. … Rescue hoarders believe they’re the only people that can adequately care for their animals. Their hoarding begins with a strong desire to save animals. They also may have an extensive network of enablers, and are in complete denial about the dangerous or unhealthy conditions in which the animals are living.
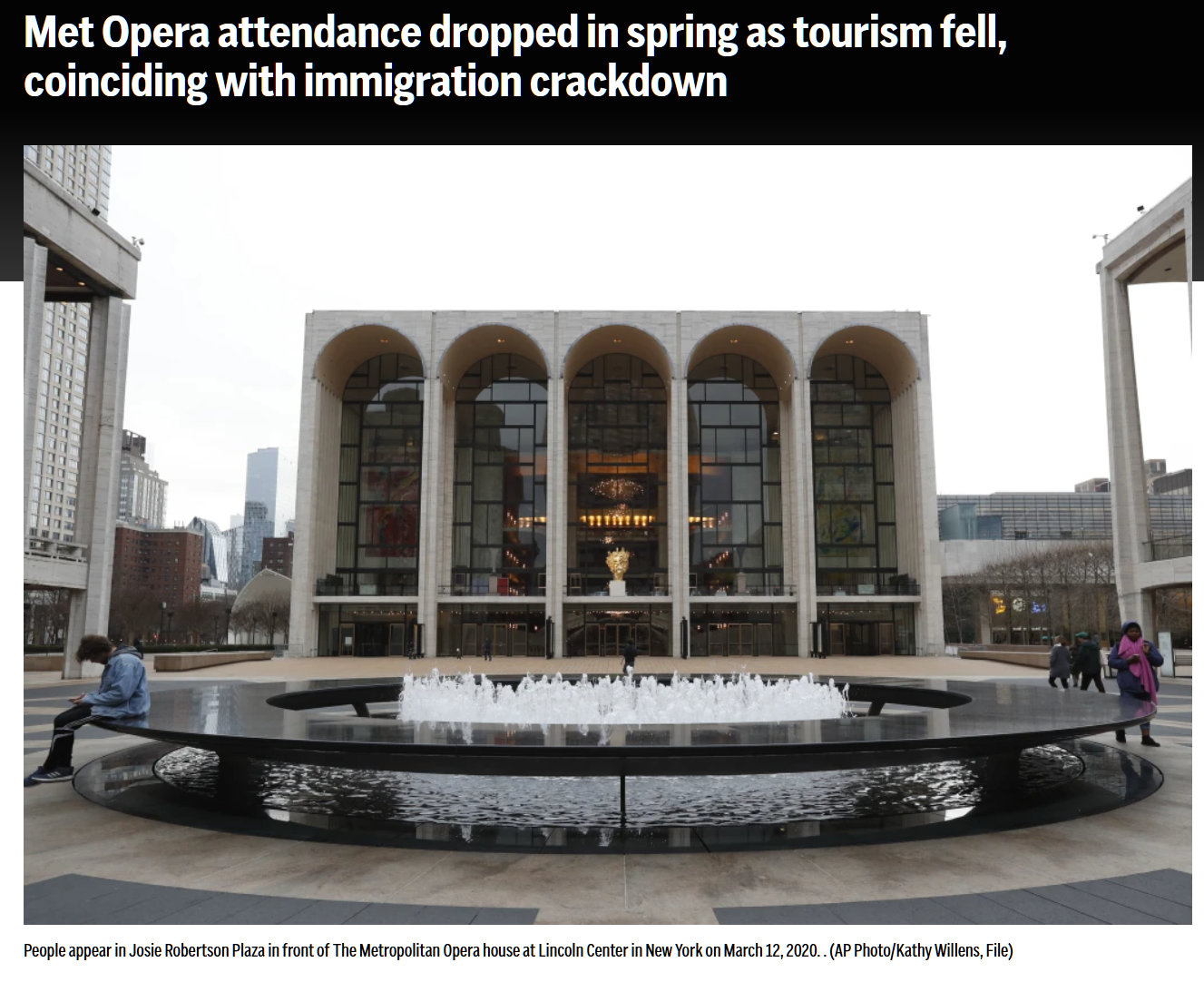
Does the analogy hold up? Below, from Politico, a situation that has changed exactly nobody’s mind in Maskachusetts regarding the merits of open borders.

Related:
- the UK is jammed with advocates for open borders despite a 2023 report by Human Rights Watch about “this system [of taxpayer-funded everything for migrants] has increasingly been plagued by serious deficiencies, in violation of people’s human rights to housing, food, education, health, and social security”
- national ASPCA page: Animal “hoarding” can be identified when a person is housing more animals than they can adequately and appropriately care for. … guardians believe they are helping their animals and deny this inability to provide minimum care.
- “‘You’re not welcome here’: Australia’s treatment of disabled migrants” (BBC): It is one of few countries that routinely rejects immigrants’ visas on the basis of their medical needs – specifically if the cost of care exceeds A$86,000 ($57,000; £45,000) over a maximum of 10 years. New Zealand has a similar policy but Australia’s is much stricter. … The government defends the law as necessary to curb government spending and protect citizens’ access to healthcare.