“Man Who’d Served His Time in U.S. Is Deported to an African Prison” (New York Times, September 1, 2025):
Mr. Etoria came to the United States [from Jamaica] on a green card in 1976 at age 12. He joined his mother, who had been sponsored by a family she worked for as a nanny, said Ms. McKen, his aunt. He had tough times early in life, she said. He saw his mother flee from his abusive father. In the United States, he struggled to adjust and was bullied in school, she said.
Mr. Etoria has a history of drug abuse, which he has blamed in part on head injuries he suffered as a child. He was also diagnosed with schizophrenia. Doctors noted that he has exhibited violent outbursts, hallucinations and paranoia, according to court records.
He was arrested in 1981 on charges of attempted murder, robbery and kidnapping. During a psychiatric evaluation, he said he could not remember exactly what happened, according to court records. He pleaded guilty and served three years in prison.
More than a decade later, Mr. Etoria walked into a leather goods shop and shot the victim three times in the head, according to Brooklyn court records. The motive was never determined, and there was no indication that he knew the victim or that the crime was gang-related.
I’m trying to figure out what our rationale has been for wanting to keep an immigrant after he “served three years in prison” for “attempted murder, robbery and kidnapping.” Why didn’t we deport him back to Jamaica in the 1980s, before he had a chance to commit murder? The U.S. government had the right to deport him, I think, but a bureaucrat somewhere concluded that American citizens would somehow be better off keeping Mr. Etoria as a neighbor?
Here’s a good window into how the female humans of America are implementing Charles Darwin’s sexual selection:
Since leaving prison in 2021, Mr. Etoria, a father of three adult children, has spoken regularly with his aunt, she said.
I.e., the schizophrenic convicted criminal has enjoyed far greater reproductive success than the typical American male who works 50 hours per week, pays taxes, and has never been arrested. Maybe that actually was the rationale for keeping him around? American women want to breed with convicted criminals and there aren’t enough native-born criminals to meet the demand for genetic material?
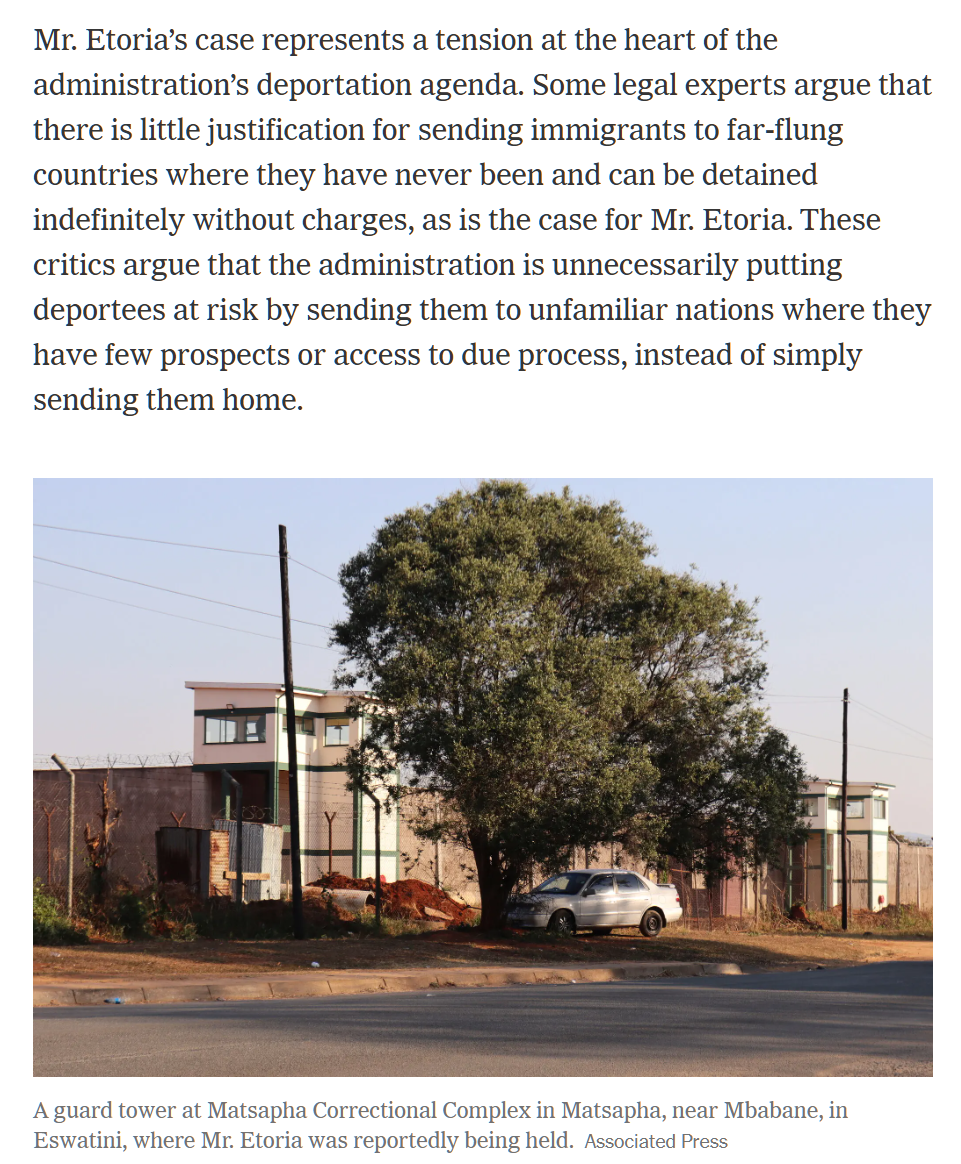
Note that the subject of the above-referenced article is not about what happened in the 1980s, but rather about the cruel Trump administration that has deported Orville Etoria to Eswatini, formerly Swaziland.
What amazes me almost as much as the idea that Americans in the 1980s couldn’t live without being enriched by a convicted criminal’s continued residence is the ability of the U.S. economy to survive Mr. Etoria and millions of similarly situated enrichers. Taxpayers have been funding shelter, food, security, etc. for Mr. Etoria almost every year since at least 1981 when he was first arrested. Taxpayers are continuing to fund shelter, food, and security for Mr. Etoria now that he lives in Eswatini. U.S. taxpayers are also funding migrant-to-migrant interactions, e.g., “Three victims of Florida 18-wheeler U-turn crash ID’d as Haitian immigrants” (New York Post):
The three victims of the Indian immigrant truck driver who made an illegal U-turn across a Florida highway earlier this month have been identified as Haitian immigrants, according to officials.
The driver Herby Dufresne, 30, and passengers Faniola Joseph, 27, and Rodrigue Dor, 53, all Haitian immigrants, were in their minivan when it plowed into the side of an 18-wheeler driven by Harjinder Singh, an immigrant from India, on Aug. 12, the Miami Herald reported.
(I’m not sure what the argument for keeping the enricher Harjinder Singh here in the U.S. was. India is home to 1.45 billion humans, a number that grows every year, and also India is too dangerous for any human to occupy?)
Full post, including comments