A comment on “Power of the Media to Shape Coronaplague Beliefs” (June 29):
Brett Arron, MD
It is amazing that people are willing to dismiss the NYT reports while ignoring data evaluations by the experts in infectious diseases and epidemiology. New cases are a leading indicator of what is coming. Average onset of symptoms from exposure is 5.2 days ranging up to 10-14 days. It is another 10 days before hospitalization becomes necessary for about 20% of the population, It may be another few days before intubation and mechanical ventilation become necessary in about 2.5% of the infected population. Around 1.8% of the CoV19 patients progress from respiratory failure and develop failure of multiple organ systems and succumb to the infection 1-3 weeks after intubation.
Rather than trying to reason your way with an incomplete set of data and facts to an answer you would like, you would be best following expert advice. Wear mask, socially distance, minimize your exposure to crowds and encourage others to exercise exemplary citizenship and do the same.
BTW in some recent strains of the SARS2 CoV-19 virus spike S1 and S2 proteins have stable and more effective at transmitting the infection to cells.
Annual mortality in the US from the annual influenza seasons averages about 0.2%. US CoV-19 mortality rates are 10 times higher about 2%. With the recent trends to younger patients hopefully the mortality rate will start to fall.
Publishing half truths confuses the issues and distracts from our best responses. Sweden’s mortality rates are much higher than their neighbors. New Zealand clamped down hard initially and is now CoV-19 disease free.
Free speech has limits. It is illegal to scream fire in a movie theater. In this analogy, there is a fire in the theater and you and people like you are telling people it is okay to stay in your seats, just ignore the smoke and fire alarms, no one had died.
Herd immunity
My implicit prediction was that the downward/flat trend in deaths in the U.S. was likely to continue, despite the rising trend, starting in mid-June, of positive infection tests. This prediction was based on decades of experience… as a computer programmer. Dr. Brett Arron’s was based on actually knowing something.
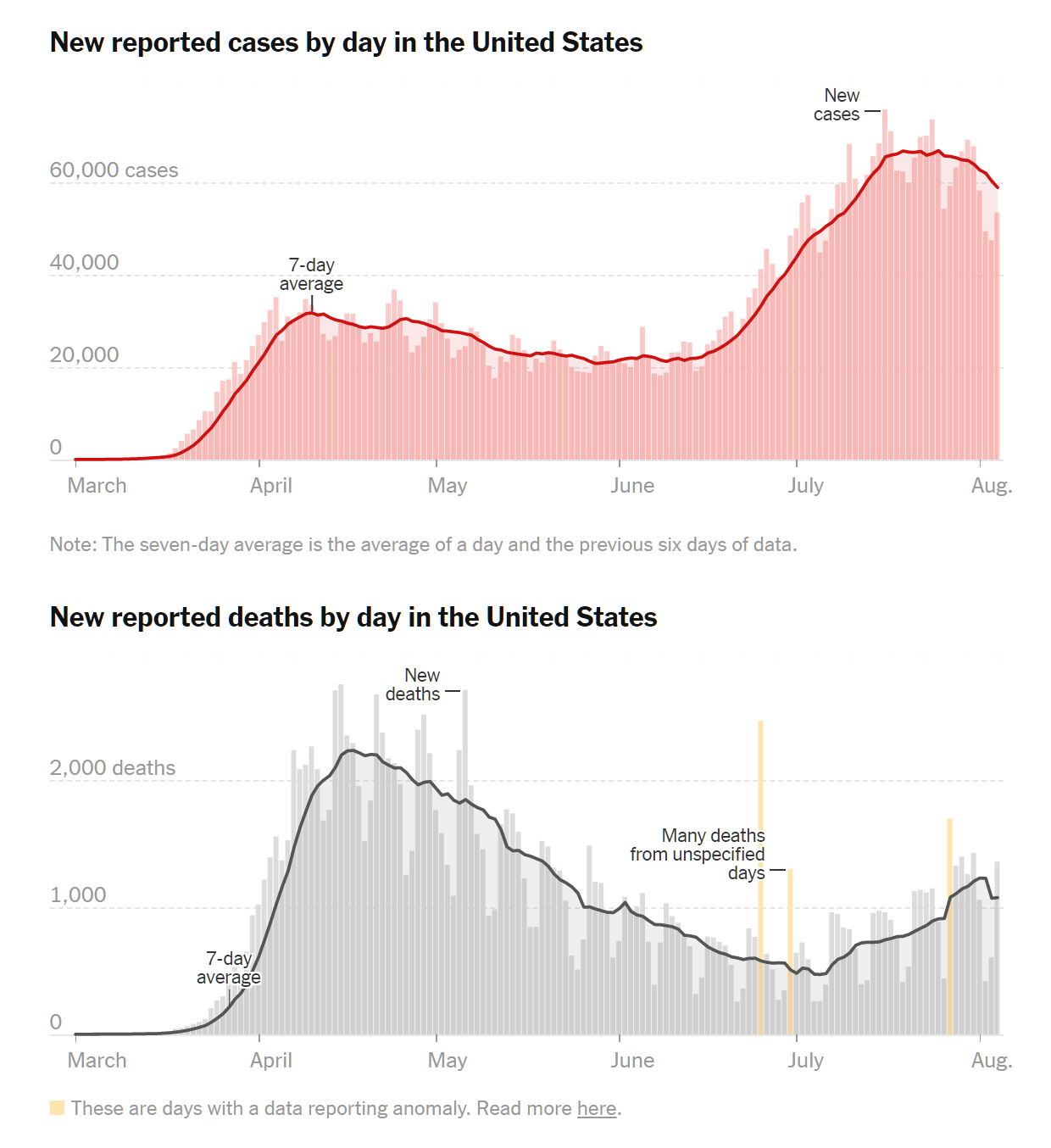
It has now been roughly 8 weeks since the “new reported cases in the U.S.” started trending up. What are we seeing in the trend of “new reported deaths”?
———— everything above this line was written on June 29 ————-
Well… it looks like I owe Dr. Arron dinner! From NYT:
I surely wish that I had been right, partly because I love to be right but mostly because it is sad when a virus is able to kill people.
On June 29 there were roughly 40,000 cases (positive tests). Using Dr. Arron’s numbers, today would be roughly when we would expect those who tested positive on June 29 to die. The death rate is about 1,000 people per day. Dr. Arron said it would be 1.8 percent of those who tested positive, which works out to 720.
Other than admitting to being stupid, what is my explanation for being wrong? I have consistently underestimated the power of shutdown. Knowing that Americans, despite a “shutdown”, were continuing to meet in grocery stores, marijuana stores, liquor stores, on Tinder (record usage), etc., and having seen Americans wearing filthy bandanas underneath their noses as PPE, I did not believe that we were having an effect on viral transmission.
About two weeks after the post that kicked off this follow-up, I began to doubt my assumptions: “Coronaplague test data show that Florida successfully flattened the curve?” At least in Florida, everything worked the way that it was supposed to, according to the Church of Shutdown dogma, March edition. By sacrificing their children’s education, sacrificing their long-term mental and physical health, sacrificing development of work skills, and eliminating their social lives, Floridians actually did push their plague back by a couple of months. If Floridians did it, maybe people in a lot of other states “succeeded” as well. This is a Pyrrhic victory, of course, since the reward is simply prolonging the shutdown and the “war” that we’ve declared on the virus that we are almost certainly destined to lose. It is also not a “success” as defined by minimizing deaths, since the deaths from shutdown will far exceed any lives saved from slowing down Covid-19.
Could we have done anything differently if we had known that the decline in deaths was simply to a local minimum?
Wear masks more diligently? “The land with no face masks: Holland’s top scientists say there’s no solid evidence coverings work and warn they could even damage the fight against Covid-19” (Daily Mail, August 4)
Social distance more distantly? Well, people don’t bother once they’re masked. But, even if they did, what would be the point? Shift Covid-19 infections and deaths into October?
Minimize exposure to crowds, as Dr. Arron suggests? Young people have already given up on this, right? And old/vulnerable people are still in their bunkers.
What is the value of all of these data, aside from proving that Dr. Arron was right and I was wrong?
Related:
- Our reward for all of the shutdowns and sacrifices: “One death every 80 seconds: The grim new toll of COVID-19 in America” (NBC) Over the last seven days, a grim new COVID-19 calculus has emerged: one person died every 80 seconds from the coronavirus in America. … The Chicago Public School system became the latest to ditch plans to reopen classrooms to in-person education come September. Instead, the nation’s third-largest school system will do what many other school districts are doing and reopen remotely on Sept. 8 and revisit that strategy on Nov. 9. [instead of three months of European-style terrible news from around the whole country, followed by a European-style resumption of normal life, we will perhaps have years to beat ourselves up about this]
1) We would only need to get the reproductive rate below 1 for the virus to dissipate and die out. Many states have done this for a period of time:
https://rt.live/
This mirrors almost exactly your (correct) prediction about the AIDS would not become an epidemic in the heterosexual community because an average of 6 lifetime sex partners is mathematically very different than the average 1160 partners of the average AIDS victim[1].
2) I was personally skeptical about vaccines, but progress seems very promising.
3) Your cost-benefit analysis is focusing only on mortality and ignoring significant, and unknown, morbidity. Is a lifetime of chronic fatigue, neurological complications, lung damage (75%), heart damage, or missing fingers really worth a few months of wages or public school BLM/LGTBQ+ indoctrination?
[1] http://www.2blowhards.com/archives/2007/02/aids_and_immune.html
sorry; the heart damage is 75%, but “ground glass opacities” on lung CT scans are also common.
Also, regarding R_t, about 40% of states are < 1.0 right now, and many others are only slightly above 1. As Andy Slavitt says, "We can virtually eliminate the virus any time we decide to." New Zeeland successfully knocked it out and reopened, COVID-free, in June.
Your expectation of flat mortality rate given an increase in infection rate was too optimistic. It assumed that only young people would be infected after distancing enforcement is over. As I wrote at about the same time: “An increase in new cases was expected due to relaxing containment measures: the infected people did not just vanish. […]
To what degree the surge in the number of newly discovered cases will translate in the number of deaths remains to be seen in a couple of weeks”
Anecdotal evidence (that may or may not be representative of the actual situation) I am getting from LA and Miami is that new cases apparently predominantly originate among hard-partying young people. Unfortunately, a lot of those young people are in contact with older more vulnerable folks, especially in Hispanic communities where families are much closer than elsewhere, probably similar to Italy and France but opposite to the Nordic countries. Hence, a higher increase in fatalities than one would expect.
https://www.palmbeachpost.com/news/20200731/florida-couple-jailed-for-refusing-to-quarantine-after-positive-covid-19-test-police-say
On the other hand, the 2% *average* IFR the good doctor claimed is not corroborated by data from various sources and is far too pessimistic: it is closer to 0.6-0.7% (Iceland/Sweden). Probably, the 1.5-2% ratio of deaths per number of tested(TFR/test fatality rate ?) is closer to the CFR assuming that the overwhelming majority of people who do get tested end up in the hospital. But that’s just an assumption.
As to what realistically could have been done in this country ? Probably, people older than 50 self-isolating from younger folks with the latter cooperating, and convincing the older ones to practice safe distancing, that’s about it. I do not see any draconian measures, similar to what some countries did, really possible in much of this country — you play with cards/people you were dealt.
Ivan: The elderly/vulnerable (me!) isolating themselves makes sense, but of what value is data for implementing that strategy? We know that coronaplague is potentially deadly, especially for unhealthy 82-year-olds (the typical victim here in Maskachusetts). Couldn’t we have implemented some isolation, e.g., government rents out hotel rooms for older people who otherwise would have been stuck in small apartments with young family members going out and being exposed, without knowing precisely how many positive tests were coming back?
“It is illegal to scream fire in a movie theater”
That’s a fallacy – for this, maybe the doctor should spring for the wine at your dinner?
Steve: Are you sure it is legal? (assuming no fire) https://en.wikipedia.org/wiki/Shouting_fire_in_a_crowded_theater suggests that it may still be illegal if you expect people to riot or trample each other. Of course, if you shout “Black Lives Matter”, we know that Americans actually do riot and loot. But that is legal because it is true?
Phil –
I’m not a lawyer, nor do I play one on the internet. But… there are well-reasoned several articles about this: https://www.theatlantic.com/national/archive/2012/11/its-time-to-stop-using-the-fire-in-a-crowded-theater-quote/264449/ and https://www.thefire.org/a-reminder-about-shouting-fire-in-a-crowded-theater/
In 1969 the Supreme Court narrowed free speech restrictions to where the speech is “directed to inciting or producing imminent lawless action and is likely to incite or produce such action”.
My reading is that falsely screaming “fire” in a theater wouldn’t meet this standard.
Seems like several European countries did subscribe to the Church of the Shutdown, and like Florida, it worked like it was supposed to. However, looking today (https://ourworldindata.org/coronavirus) at Spain, France, Denmark, UK, Germany, Norway, Italy, Portugal, and Belgium, cases are trending up/capita in all except Portugal and Belgium.
Also, Phil, in an earlier post (https://philip.greenspun.com/blog/2020/06/10/team-america-saved-our-country-from-covid-19/) we debated the US vs Sweden death rate. Well, you may have been wrong with Dr Arron, but you were right about the convergence. On June 10, the US death rate was 26% lower than Sweden (see that post). Today it is about 14% lower using figures from: https://coronavirus.jhu.edu/data/mortality. Maybe I need to buy you a cup of coffee 🙂
Arizona is about two weeks ahead of Florida and well past it’s peak in case growth. As of right now they have deaths per capita about half of Maskachusetts, and I don’t think they’re going to catch us. Florida also appears to be on the downslope, and is at maybe 1/3 our level, but will keep rising for another week or two.
I suspect that the outbreak in the Northeast in Feb-April was 3-10 times larger than the official case count reflects. It was difficult to impossible to get a test before mid-late April up here (and still slow today) unless you were in pretty bad shape. Otherwise the docs told you to stay home and take Tylenol and chicken soup. I suspect the FL/AZ/etc outbreaks are capturing a lot more of the true cases so the comparative numbers of cases:fatalities are going to look different.
Phil …
You owe many of us …
The idea of shutdowns after the virus was circulating in the community was to buy time and prevent hospital overload (mitigation), not to eradicate the virus. And the efforts worked. Now, several vaccines are showing significant promise. So there is light at the end of the tunnel. Many lives were saved by flattening the curve to the extent we did, and many more can be saved by continuing distancing etc … until we are vaccinated. Shifting an exponential growth curve to the right by delaying growth in sections or making it flatter by lowering growth rate overall can save large number of lives to the right of a fixed vaccination date. This has been obvious from the start.
As for “no evidence masks work” … Lack of evidence is not evidence of lack. Masks obvious deflect most infectious exhalation away from the person one faces when talking. So do face shields. It is reasonable to wonder whether cloth or surgical masks work better or worse than face shields. It is not reasonable to suspect that neither of them have a significant beneficial effect. It would be extremely surprising if they did not. Our eyes and mouths are in the front of our heads. So unfortunately we face each other while talking. Getting our possible infected exhalations to go sideways instead of forward is an obvious and easy mitigation. Most cloth masks are too resistive to air flow to do much more than deflect exhaled air to the side and back. Probably that’s the main mechanism of action. And it is probably good enough in many cases, regardless of thread count, extra filters, etc …
People wear surgical masks all the time in Japan when the have a cold. It is a little weird, but easy to get used to.
Gill: Agreed that the Japanese considerately wear masks when they are not feeling well (just as WHO recommended regarding coronaplague from February through early June). But it doesn’t seem to have helped them with influenza. Their death rate from the flu in Japan was more than 2X the (unmasked at the time) U.S. death rate from this ancient scourge. https://www.worldlifeexpectancy.com/cause-of-death/influenza-pneumonia/by-country/
Masks sound great in theory, and I’m sure that they could work well in a lab experiment, but the Europeans who think that masks are counterproductive are factoring in human nature. People seem to be able to follow one rule at a time. They either maintain a 6′ distance OR they wear a mask and ignore the 6′ distance.
I don’t believe that the U.S. sacrifices (shutdowns, kids thrown out of school, adults forced to stay home and get fat/depressed, health care for non-Covid-19 conditions shut down) delayed infections/deaths long enough to make a big difference. There is no vaccine available right now. IHME forecasts that the U.S. will have a higher death rate than no-shutdown Sweden by early September. (see https://covid19.healthdata.org/united-states-of-america and click on “Compare”). If you look at the curves, the U.S. shutdown seems to have delayed some infections/deaths by about three months. Given all of the deaths that we caused via shutdown, that was not a rational decision for anyone who is interested in minimizing deaths overall.
(see https://thehill.com/opinion/healthcare/499394-the-covid-19-shutdown-will-cost-americans-millions-of-years-of-life for an attempt to calculate some of the life-years lost due to shutdown. That was before the U.S. erupted into riots/looting, another social ill that the Swedes have been spared.)
Phil,
2 recent studies (one I believe Russel V pointed out) conclude masks do help (at a macro level)
https://www.medrxiv.org/content/10.1101/2020.05.22.20109231v5
“Conclusions. Societal norms and government policies supporting the wearing of masks by the public, as well as international travel controls, are independently associated with lower per-capita mortality from COVID-19.”
and
https://www.healthaffairs.org/doi/10.1377/hlthaff.2020.00818
“The study provides evidence that US states mandating the use of face masks in public had a greater decline in daily COVID-19 growth rates after issuing these mandates compared with states that did not issue mandates. These effects were observed conditional on other existing social distancing measures and were independent of the CDC recommendation to wear face covers issued April 3, 2020. As international and state governments begin to relax social distancing restrictions, and considering the high likelihood of a second COVID-19 wave in the fall and winter of 2020,30 requiring the use of face masks in public could help in reducing COVID-19 spread.”
Could you please examine the excess death rate? That is, in a population there is a usual death rate per year of some number per capita/ per million population. How much “extra” death has Covid caused?