“Government Model Suggests U.S. COVID-19 Cases Could Be Approaching 100 Million” (NPR):
The actual number of coronavirus infections in the U.S. reached nearly 53 million at the end of September and could be approaching 100 million now, according to a model developed by government researchers.
Since [September], the CDC’s tally of confirmed infections has increased to 12.5 million. So if the model’s ratio still holds, the estimated total would now be greater than 95 million, leaving about 71% of the population uninfected.
The model, created by scientists at the Centers for Disease Control and Prevention, calculated that the true number of infections is about eight times the reported number, which includes only the cases confirmed by a laboratory test. … Some of these antibody studies have suggested that only about one in 10 coronavirus infections is reported.
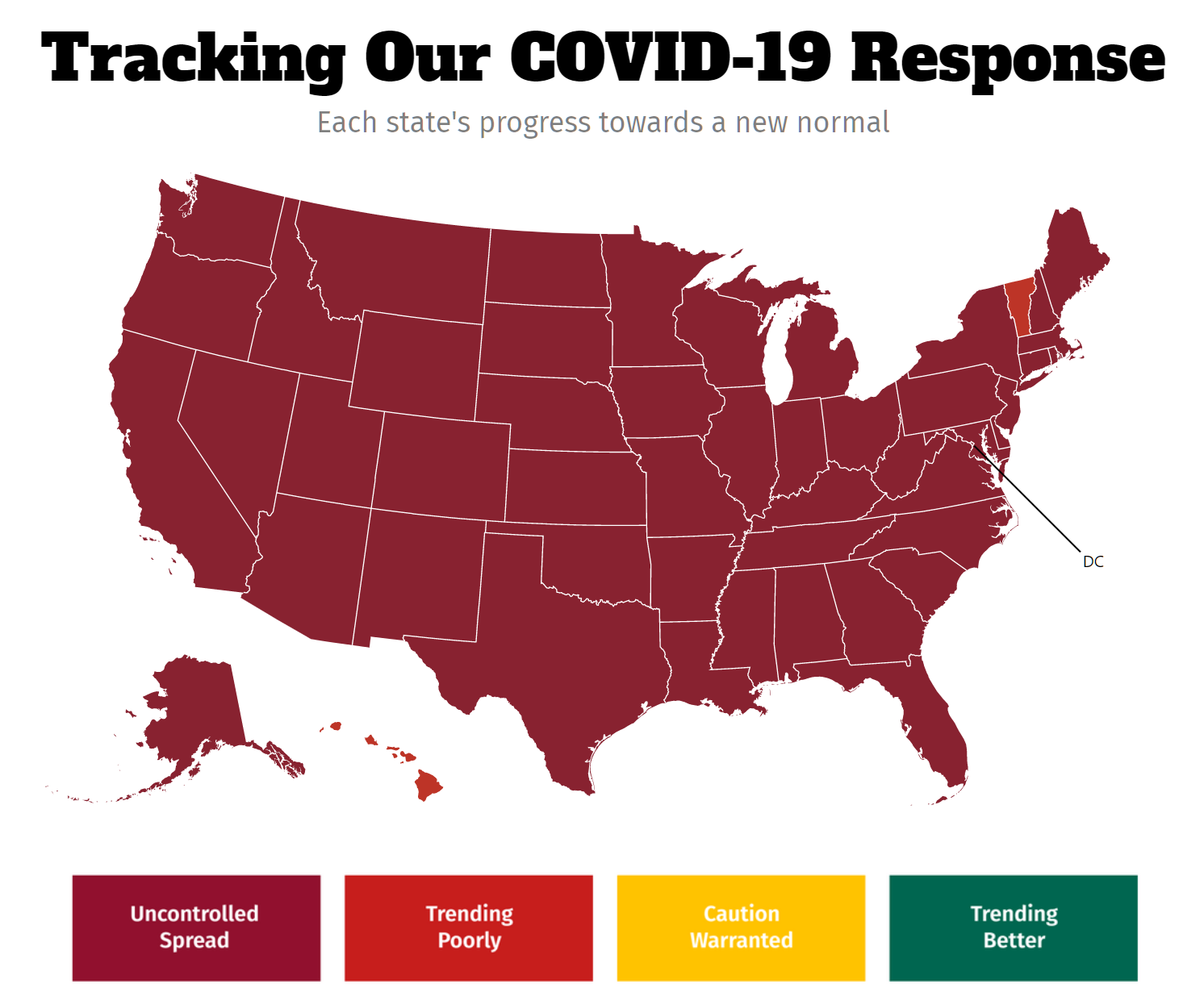
Cases are currently “spiking” all over the U.S.:
We yearned for ventilators and, by the time they were available, realized that we didn’t need or want them (since they actually harm the typical COVID-19 patient). Currently we yearn for vaccines, but perhaps we won’t need or want them by the time they’re available in significant quantity. (Though perhaps a vaccine could be useful to boost the immunity of someone who’d had COVID-19 the natural way a year earlier.)
Coronavirus is a biopagical agent that takes about two weeks to benignly resolve for most people, with rapidly improving therapeutic options. Coronapanic is a collective hysteria, a chronic and progressive condition.
No matter what else happens this year, I nominate this for the most honest statement from a Public Health Professional in the United States.
‘I’m definitely going to get it. We all are,’ – Judith Persichilli, NJ State Health Commissioner, March 21, 2020.
https://www.nj.com/coronavirus/2020/03/im-going-to-get-it-we-all-are-njs-top-health-official-says-as-she-leads-the-states-coronavirus-war.html
Another model (by MIT grad Youyang Gu) suggests that the total number of Americans infected with Covid is somewhere between 10% and 23% of the population – a bit lower, but still remarkably high. The model includes state-by-state and county-by-county numbers.
Nope. The viral epidemic is OVER. What we have is epidemic of false positives somehow declared “cases”. That’s why mortality is flat while “cases” are growing – tracking the number of tests performed. There is no other explanation.
Add to that the fact that RT-PCR tests can (and routinely are) tweaked to generate nothing but noise by dialing the count of cycles up to absolutely ridiculous numbers.
Ever hear words “false positive” from mainstream media or politicos? No? That says everything.
“There is no other explanation.”
Deaths lag cases by about three weeks.
In fatal cases, it usually takes a couple weeks from diagnosis to hospitalization, and then another week or so until death.
I remember seeing footage of the 2011 tsunami, taken in Japan. It starts surprisingly slowly, with the water rising; it’s not like there’s a dramatic wave towering over everything. But the water just keeps rising and rising. The pandemic is like that.
> just keeps rising and rising
Not so far in Sweden. But don’t give up hope, Russil, there’s a still a few weeks left in 2020 for the Coronagod to wreak awful vengeance on the heretical Swedes. Pray hard!
I think Russil is correct. Easy to verify here: https://ourworldindata.org/coronavirus (I can’t seem to past an image of the chart showing deaths in Sweden).
If COVID-19 is so deadly, than we have far worse crises the world should worry about. Let’s start with suicide “In Japan, more people died from suicide last month than from Covid in all of 2020. And women have been impacted most” [1].
Let’s come back to this topic in 1 year and look at the TRUE impact of COVID-19’s misguided life-safety effort that we are forced into. History will record 2020 as one of the worse human made disaster that killed more people because of the slogan “We are all in it together”.
[1] https://www.cnn.com/2020/11/28/asia/japan-suicide-women-covid-dst-intl-hnk/index.html
Paul B: Russil and Lord Palmerston are both correct! Sweden automatically tags anyone who tests positive for COVID-19 and then dies within 30 days as a “Covid death”. So the percentage of Swedes who have been killed by (or with) COVID-19 is enormous (0.065%) and Karen/Russil are correct regarding the tragic wave of death that could have been averted if only Donald Trump had not been the leader of Sweden during these times. Lord Palmerston seems likely to be correct in implying that roughly the same number of Swedes will die (from all causes) in 2020 compared to previous years. https://www.statista.com/statistics/525353/sweden-number-of-deaths/ shows 81,073 deaths from Jan 1-Nov 13, 2020. In 2010 there were 90,487 deaths in Sweden. Adjusted for population growth (9.34 million population in 2010 versus about 10.23 million today), it seems very unlikely that the 2020 death rate will exceed the 2010 death rate.
(Also potentially correct: the Swedish MD/PhDs who said that half of the COVID-19 deaths in Sweden have been among those who were expected to die, due to old age and poor health, at some point in 2020.)
And yet the media continues to flood the airwaves with misinformation: “Supreme Court’s scientifically illiterate decision will cost lives” [1], and “Cuomo Attacks Supreme Court, but Virus Ruling Is Warning to Governors” [2].
The Supreme Court did NOT rule against NY to limit religious gatherings, nor is the SC “scientifically illiterate” (since when the SC is suppose to be a body of “scientist”), instead, and correctly, it ruled that NY’s law is disseminating against houses of worship, period. The decision from SC should have been 9-0, not 5-4 and Cuomo and the news media need to be called out on their misinformation as much as Trump is being called out.
[1] https://www.cnn.com/2020/11/27/opinions/scientifically-illiterate-scotus-covid-decision-sachs/index.html
[2] https://www.nytimes.com/2020/11/26/nyregion/supreme-court-churches-religious-gatherings.html
Lord Palmerston: If you’re in the US, is the situation in Sweden really relevant? This article from BMJ suggests that the Scandinavian countries have mostly converged on common policies for the second wave, with Sweden tightening restrictions and the others loosening them, e.g. keeping schools open. (Philip, the Economist has a country-by-country comparison of weekly reported Covid deaths to excess deaths, and for Sweden they look pretty consistent.)
Because in fatal cases there’s typically a three-week delay from diagnosis to death, we know what’s coming in the US. In early November, there were about 1000 deaths per day. Now it’s about 1500. By early December it’ll be about 2500 and rising.
Philip, what are you hearing from your friends in the medical profession? This report from eastern Tennessee / southern Virginia sounds pretty bad: hospitalizations have doubled in the last month, but a lot of people don’t believe that Covid is real, even when they’re arriving at the hospital. “One nurse told me stories of otherwise healthy 30 year-olds coming in short of breath and not understanding why. She tries showing them chest x-rays and explaining evidence of the disease, but often they don’t believe they have COVID until they’re in critical condition. … People are dying because they don’t seek medical care when they begin having symptoms. They don’t believe they’re sick. And by the time they get to the hospital it‘s too late.”
Russil: Except for one friend who gets paid to treat COVID-19 patients in the ICU, my friends who are physicians or med school professors say that COVID-19 patients should not be in the hospital. There is no medical intervention that is proven effective. So they should be at home with an oxygen bottle and a high-flow cannula (see https://news.uchicago.edu/story/uchicago-doctors-see-remarkable-success-using-ventilator-alternatives-covid-19 for why this is good for patients, but tough to implement in a hospital because you don’t want coronavirus sprayed around the room). Perhaps occasionally a nurse or doc could swing by to administer one of the drugs that are thought (but not proven) to be helpful.
The hospital is great if you’ve been in a car accident or have a heart problem.
(Regarding the Swedish “restrictions”, keep in mind that there are no restrictions on schools, workplaces, or individuals who want to host parties at home. The new rules (first since March) prevent people from operating a commercial movie theater with more than 8 customers. They don’t prevent a company from showing a movie to 75 employees or a school from showing a movie to 200 students or a rich Swede from having 30 people over to enjoy a home theater. And there are no masks. Our Swedish helicopter instructor just confirmed today “My parents in Sweden don’t even own a mask.”)
Thanks, Philip. The CDC talks about people having to be hospitalized “for supportive management of the most common complications of severe COVID-19: pneumonia, hypoxemic respiratory failure/ARDS, sepsis and septic shock, cardiomyopathy and arrhythmia, acute kidney injury.” Also hypercoagulability.
Med school prof’s explanation was simpler: “Home model kills the rationale for the hospital cash cow.”
Russil, oh you gave up hope – so Sweden is now irrelevant! At least their failure to die in numbers that would make them relevant has not dented your belief.
How many more countries will become irrelevant? Most of the numbers associated with Coronaplague – deaths, cases, infections etc – are garbage. However, whether someone is alive or dead is less subject to interpretation by “experts”, so actual deaths from all causes are revealing. To those of us, that is to say, who still seek truth through facts.
And it turns out that we never had excess deaths in the US either, according to a John Hopkins study.
https://web.archive.org/web/20201126163323/https://www.jhunewsletter.com/article/2020/11/a-closer-look-at-u-s-deaths-due-to-covid-19
which contradicts CDC numbers that say that excess deaths are high
https://www.cdc.gov/nchs/nvss/vsrr/covid19/excess_deaths.htm
And the John Hopkins study has been taken off line, not because it is wrong, but because people are criticizing the implications of the study.
https://pjmedia.com/news-and-politics/matt-margolis/2020/11/27/johns-hopkins-study-saying-covid-19-has-relatively-no-effect-on-deaths-in-u-s-deleted-after-publication-n1178930
This pandemic is entirely a media creation. Somebody please prove me wrong.
I gave up trying to convince people like you. You could be dying from the virus and your last word would be “hoax”.
The first shipment of Pfizer vaccines has arrived on United planes carrying seven and a half tons of dry ice to keep them viable.
A source familiar with the process told NBC News the FAA is allowing United to carry 15,000 pounds of dry ice per flight — five times more than is usually permitted — to keep the doses sufficiently cold.
https://www.nbcnews.com/news/us-news/live-blog/covid-live-updates-la-county-orders-post-thanksgiving-lockdown-n1249195/ncrd1249229#liveBlogHeader
Russel,
According to JHU, the cases are up but so is the testing. The percent positive cases seem to be leveling off:
https://coronavirus.jhu.edu/testing/individual-states/usa
The excess deaths are close to normal:
https://www.cdc.gov/nchs/nvss/vsrr/covid19/excess_deaths.htm
Almost none of the serious COVID cases are of 30 year olds unless you’re morbidly obese.
We can agree that COVID was real, but not our interventions have likely had no positive effect on virus deaths:
https://www.israelnationalnews.com/News/News.aspx/291374
More than likely, what we did was actively harmful. Stay scared, my friend.
Bryce: On the plus side, we’re substantially fatter than we were before the government locked us down (5-15 lbs. typical for an adult). So we are better prepared in case the plague is followed by famine. https://www.webmd.com/lung/news/20201029/pandemic-diet-how-to-lose-the-quarantine-15
(There are no health problems associated with obesity, I hope/trust!)