How do I return 6 square miles of Plexiglas?
What if you rejected my harebrained idea, Build downdraft paint booths for K-12 schools?, and #FollowedScience by investing in acrylic barriers?
“Those Anti-Covid Plastic Barriers Probably Don’t Help and May Make Things Worse” (NYT, 8/19/2021):
Covid precautions have turned many parts of our world into a giant salad bar, with plastic barriers separating sales clerks from shoppers, dividing customers at nail salons and shielding students from their classmates.
Intuition tells us a plastic shield would be protective against germs. But scientists who study aerosols, air flow and ventilation say that much of the time, the barriers don’t help and probably give people a false sense of security. And sometimes the barriers can make things worse.
Research suggests that in some instances, a barrier protecting a clerk behind a checkout counter may redirect the germs to another worker or customer. Rows of clear plastic shields, like those you might find in a nail salon or classroom, can also impede normal air flow and ventilation.
(Note the “false sense of security”, which is why the Swedish MD/PhDs didn’t want to order residents to wear bandanas and paper/cloth masks. Masked humans would be more comfortable crowding together and the vulnerable would feel comfortable entering indoor public environments that, in fact, could not be made safe with these primitive tools.)
Maybe the plastic barriers work better to separate diseased K-12 students? “The Science of Masking Kids at School Remains Uncertain” (New York, August 2021) says “no”:
At the end of May, the Centers for Disease Control and Prevention published a notable, yet mostly ignored, large-scale study of COVID transmission in American schools. A few major news outlets covered its release by briefly reiterating the study’s summary: that masking then-unvaccinated teachers and improving ventilation with more fresh air were associated with a lower incidence of the virus in schools. Those are common-sense measures, and the fact that they seem to work is reassuring but not surprising. Other findings of equal importance in the study, however, were absent from the summary and not widely reported. These findings cast doubt on the impact of many of the most common mitigation measures in American schools. Distancing, hybrid models, classroom barriers, HEPA filters, and, most notably, requiring student masking were each found to not have a statistically significant benefit. In other words, these measures could not be said to be effective.
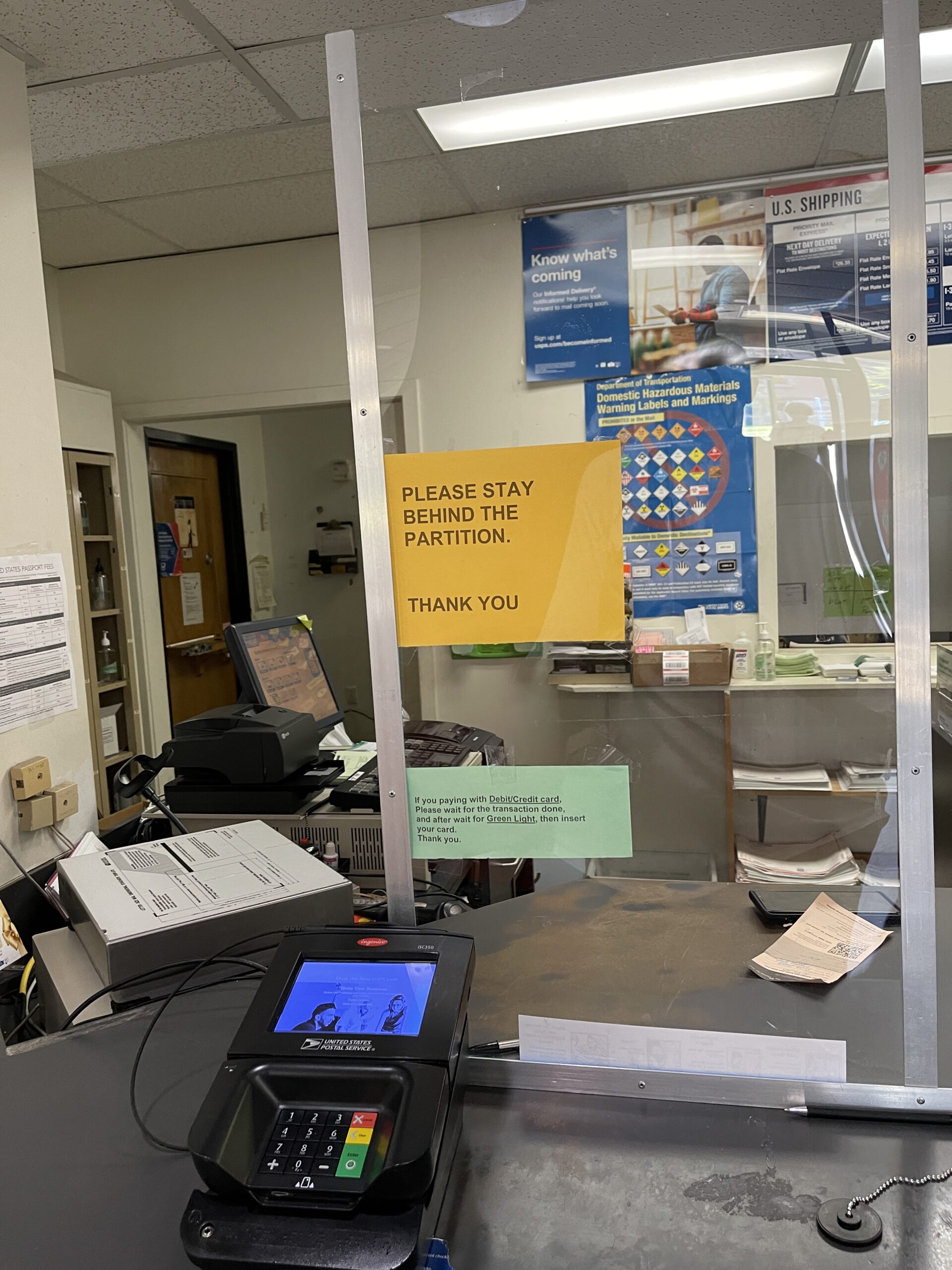
#Science did not evaluate my downdraft paint booth idea, sadly. From the Watertown, Maskchusetts central post office, August 27, 2021:
Related:
- “The 60-Year-Old Scientific Screwup That Helped Covid Kill” (WIRED, 5/13/2021): “The distinction between droplet and airborne transmission has enormous consequences. To combat droplets, a leading precaution is to wash hands frequently with soap and water. To fight infectious aerosols, the air itself is the enemy. In hospitals, that means expensive isolation wards and N95 masks for all medical staff. … An indoor-air researcher at the University of Hong Kong, Li had made a name for himself during the first SARS outbreak, in 2003. His investigation of an outbreak at the Amoy Gardens apartment complex provided the strongest evidence that a coronavirus could be airborne. But in the intervening decades, he’d also struggled to convince the public health community that their risk calculus was off. Eventually, he decided to work out the math. Li’s elegant simulations showed that when a person coughed or sneezed, the heavy droplets were too few and the targets—an open mouth, nostrils, eyes—too small to account for much infection. Li’s team had concluded, therefore, that the public health establishment had it backward and that most colds, flu, and other respiratory illnesses must spread through aerosols instead.”