An interesting work of journalism from the Washington Post: “U.S. deaths soared in early weeks of pandemic, far exceeding number attributed to covid-19”
The analysis is similar to the New York Times effort that was the basis of “Infidels in Sweden are refusing to die” (at the time, Sweden in its refusal to shut down had 1/25th the percentage of “excess deaths” compared to the shut-down-for-a-month New York City). The authors take a deeper look at the U.S. overall.
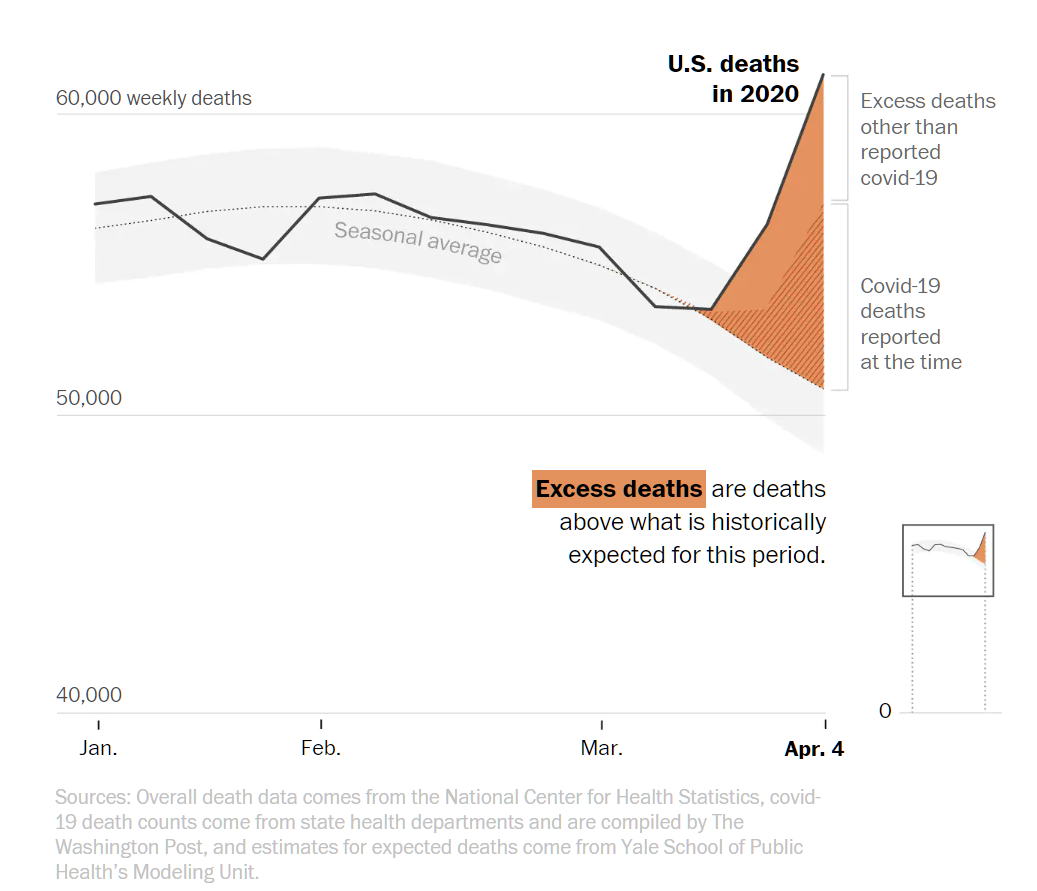
Let’s start by trying to raise everyone’s coronapanic with a chart that starts at 40,000 rather than 0. This makes the recent rise in overall deaths look a lot more scary:
Americans are dropping dead at an alarming rate, either from Covid-19 or from the shutdown of the regular health care system or maybe from eating too much while lying on the couch! (to the newspaper’s credit, a tiny zero-based chart is presented at the bottom right of the above figure)
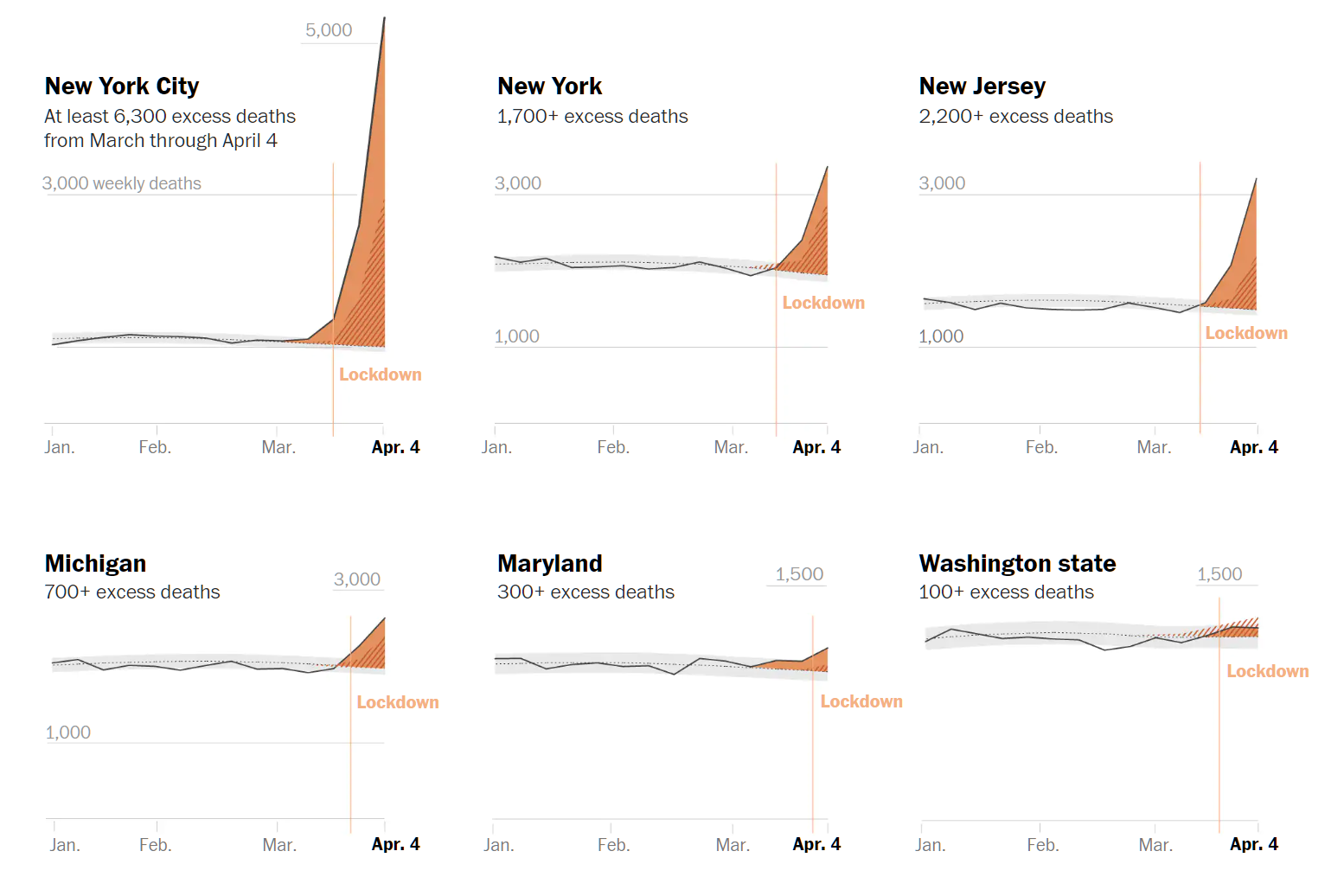
Almost all of these excess deaths are from one place: the New York metro area. And it is difficult to know whether their Covid-19 death numbers are comparable to other parts of the U.S.:
No jurisdiction has been as aggressive as New York City, the U.S. epicenter of the epidemic, in revising its death counts from those early weeks. As of Saturday, the city had added 2,542 covid-19 deaths to those figures, driving the total from that period up to 5,085. The newly added deaths were almost equally split between cases that were confirmed through lab testing and cases that were deemed “probable” covid-19 deaths based only on symptoms and exposure.
How does it look around the bad parts of the U.S.?
(By applying the miracle of begging the question, the above charts, with their dramatic increases in deaths after the shutdown began, actually support continued faith in the Church of Shutdown. Asked how they know that shutdown works, the faithful in the Religion of Shutdown generally respond with “the high number of deaths shows that it would have been far worse if we hadn’t shut down.”)
Is the headline a good summary of the article? Are U.S. deaths soaring? We are all in this together, right?
But in dozens of states, the Yale analysis shows that the reported number of overall deaths are either unchanged or even slightly down compared with historical patterns.
Should we suspect from these data that the problems NYC has had with Covid-19 are idiosyncratic? Some other cities and regions also had exposure starting at roughly the same time (mid-January?) and those places locked down within a few days of the NYC shutdown. Yet excess deaths are fairly low (or actually negative) almost everywhere other than NYC.
Is it possible that we’re fighting a nationwide war against a virus that is attacking only a handful of cities for reasons that are peculiar to those cities? Or possibly peculiar to the strain of the virus that has been circulating in those cities? If we take out metro NYC, Detroit, New Orleans (they’re not going to have a second Mardi Gras this year, right?), and Boston, does the “U.S.” actually have excess deaths or any kind of problem with Covid-19 that couldn’t be handled with the most basic precautions?
(And how would we handle the apparently idiosyncratic problems with these cities? Tell New Orleans that Mardi Gras is henceforth restricted to the sober (90% reduction in crowding?). Reopen the United States economy and use the money to pay roughly half of NYC residents to move out to suburbs and other states. The super high density plainly has made NYC a breeding ground for any enterprising virus. Run more subway trains in Boston so that people aren’t jammed in like sardines and/or pay people to leave the city, as in New York. I’m at at loss to know what to do about Detroit, I must confess!)
In the meantime, we’ve got healthy young people in North Carolina who are under a stay-at-home order. Their personal risk from Covid-19 may be smaller than their risk of being hit by debris from the International Space Station. Have these young people lost their freedom and jobs (and their children their education for this spring) merely because of an accident of political geography, i.e., that they’re inside the same nation-state as plague-ridden New York City and Boston?
Full post, including comments