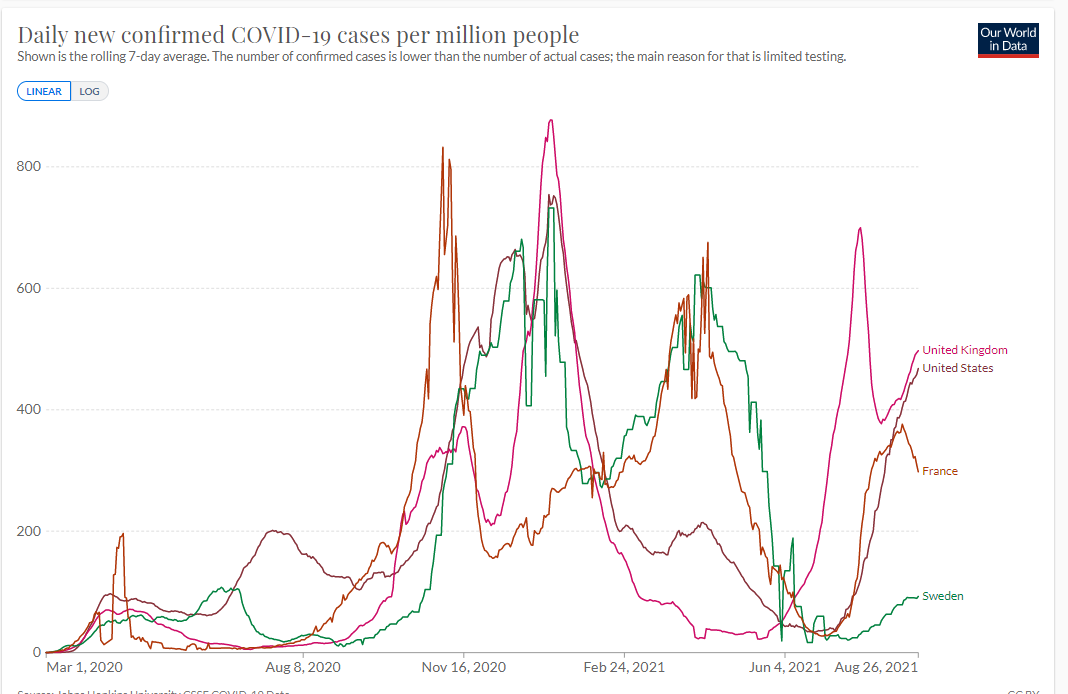
Sweden hasn’t been in the news lately. Let’s see if the wicked never-masked never-locked-down Swedes are being punished by the mighty and just CoronaG*d. First, “cases” (adjusted for population size):
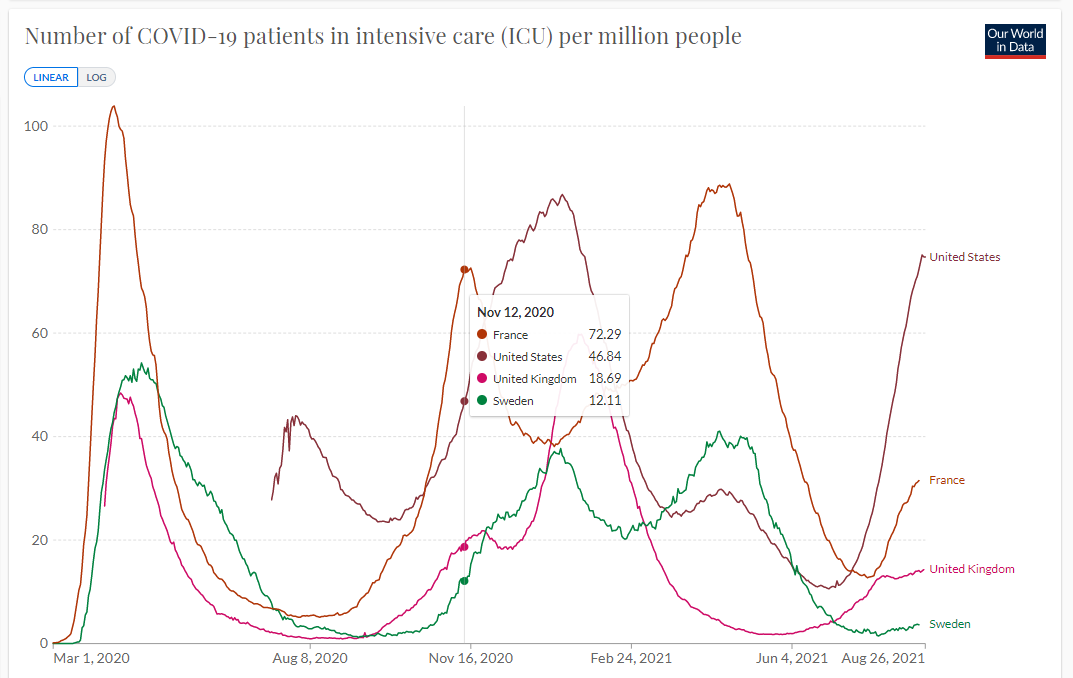
Case rate can vary tremendously depending on a country’s love for running PCR machines. Let’s look at ICU hospitalization rate:
Why aren’t the Swedes being punished for their sins?
Remember that the typical Swede lives a fairly urban existence, as noted in Analysis of Sweden versus UK COVID-19 outcomes. So it isn’t that Swedes don’t encounter one another.
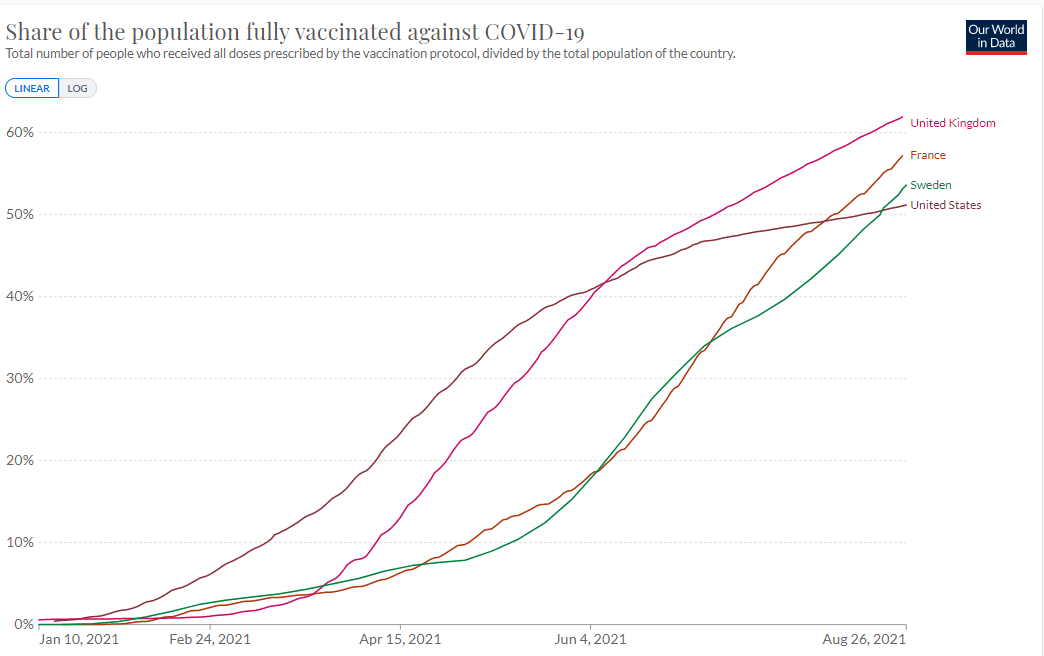
Maybe it is the miracle of vaccines? It turns out that vaccination rate is almost the same in Sweden compared to the U.S.:
How about hot weather driving people into air-conditioned shared indoor environments as an explanatory factor? The case rate (above) in the UK is higher than in the US, despite the UK being cooler than the US.
How about the choice to let humans co-evolve with what the Swedish MD/PhDs predicted would be a permanent companion virus, similar to influenza? “Having SARS-CoV-2 once confers much greater immunity than a vaccine” (Science, August 26, 2021):
The natural immune protection that develops after a SARS-CoV-2 infection offers considerably more of a shield against the Delta variant of the pandemic coronavirus than two doses of the Pfizer-BioNTech vaccine, according to a large Israeli study that some scientists wish came with a “Don’t try this at home” label. The newly released data show people who once had a SARS-CoV-2 infection were much less likely than vaccinated people to get Delta, develop symptoms from it, or become hospitalized with serious COVID-19.
The new analysis relies on the database of Maccabi Healthcare Services, which enrolls about 2.5 million Israelis. The study, led by Tal Patalon and Sivan Gazit at KSM, the system’s research and innovation arm, found in two analyses that people who were vaccinated in January and February were, in June, July, and the first half of August, six to 13 times more likely to get infected than unvaccinated people who were previously infected with the coronavirus. In one analysis, comparing more than 32,000 people in the health system, the risk of developing symptomatic COVID-19 was 27 times higher among the vaccinated, and the risk of hospitalization eight times higher.
Note that the above data contradict #Science as known to American public health experts. There would be no point in ordering the previously infected to get vaccinated before going to work or school if we didn’t know from #Science that vaccines confer much better protection than infection with the actual virus. (Remember that staying home and playing Xbox doesn’t require any vaccination, masking, or other COVID-19-related compliance!)
Readers: What’s your theory as to why Sweden is not suffering a dramatic plague right now?
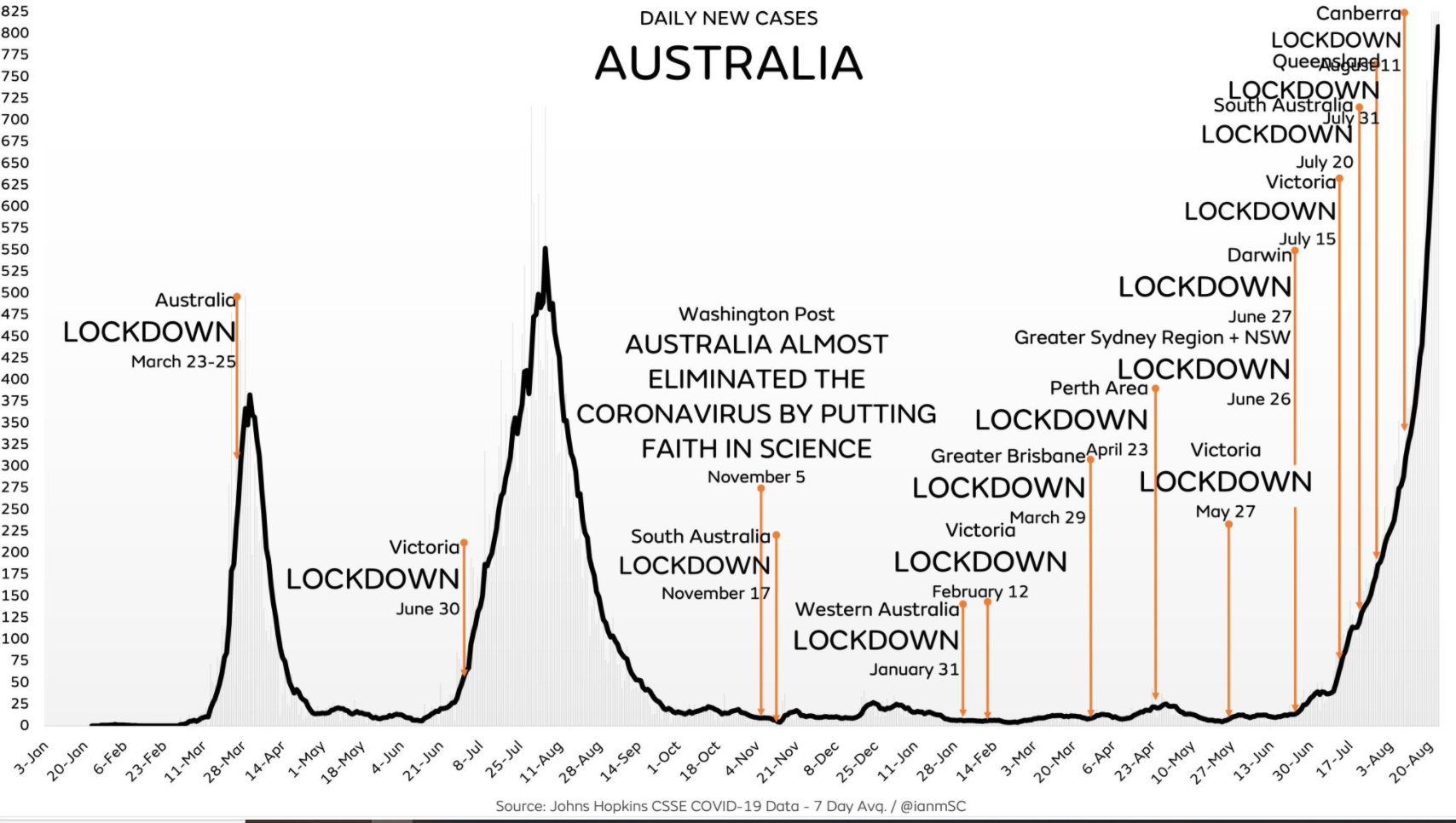
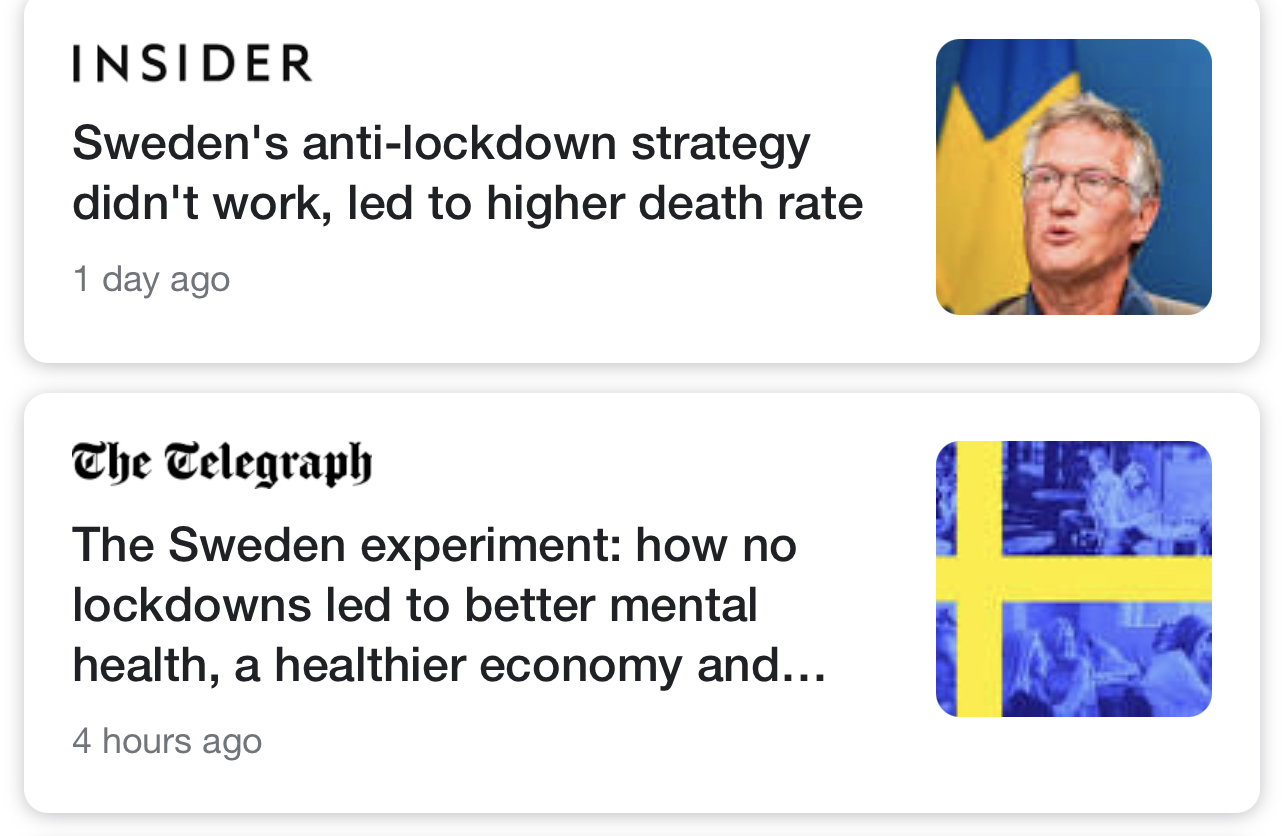
Separately, how should science-following journalists characterize a country that gave the finger to the coronavirus and ended up with half the death rate of masked-and-shut Maskachusetts (where the urban kids whose lives purportedly matter lost an entire year of education)? It all depends! Part of a screen from Apple News:
(Note that even the Telegraph folks who are apparently willing to consider the advantages of children being able to leave the house and attend school refer to Sweden following W.H.O. pandemic respiratory virus advice from pre-2020 as an “experiment”. It is not the countries that have tried general public mask orders and year-long school shutdowns that are experimenting.)
Full post, including comments