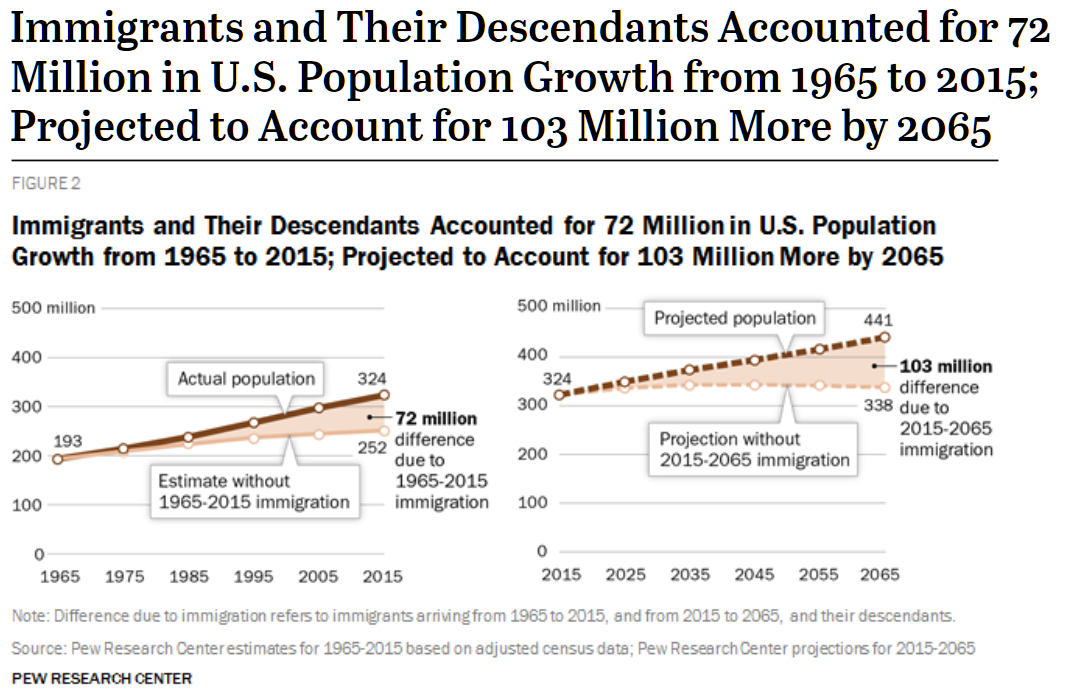
Since the mid-1960s, the U.S. has been embarked on a program of rapid population expansion via low-skill immigration (Pew):
We bring in low-skill migrants who are destined to become lower-than-median earners (if they work at all) and insist that they be provided with at least reasonably high quality housing. This makes sense only if the cost of building housing, and delivering the required energy to that housing, can be reduced via innovation.
What about America’s most successful innovator? His contribution to this challenge has been the solar roof. From Elon Musk:
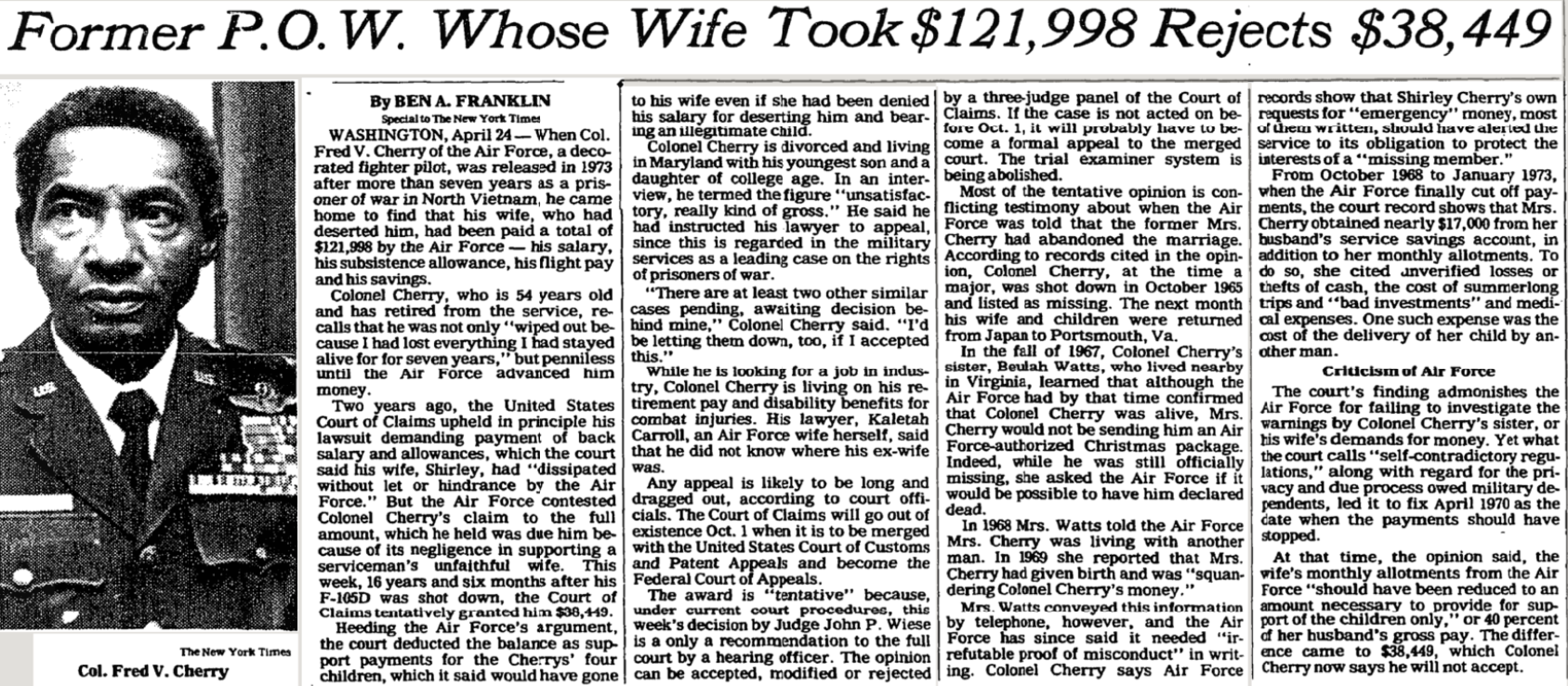
Musk had helped his cousins, Peter and Lyndon Rive, launch SolarCity in 2006, and he bailed it out ten years later by having Tesla purchase it for $2.6 billion.
As always, he invoked to [Brian Dow] the steps of the algorithm and proceeded to show how they should be applied to the solar roofs. “Question every requirement.” Specifically, they should question the requirement that the installers must work around every vent and chimney pipe sticking up from a house. The pipes for dryers and ventilator fans should simply be sheared off and the solar roof tiles placed on top of them, he suggested. The air would still be able to vent under the tiles. “Delete.” The roof system had 240 different parts, from screws to clamps to rails. More than half should be deleted. “Simplify.” The website should offer just three types of roofs: small, medium, and large. After that, the goal was to “accelerate.” Install as many roofs as possible each week.
[during a sample installation in 2021] Musk clambered up a ladder to the peak of the roof, where he stood precariously. He was not happy. There were too many fasteners, he said. Each had to be nailed down, adding time to the installation process. Half should be deleted, he insisted. “Instead of two nails for each foot, try it with only one,” he ordered. “If the house has a hurricane, the whole neighborhood is fucked up, so who cares? One nail is going to be fine.” Someone protested that could lead to leaks. “Don’t worry about making it as waterproof as a submarine,” he said. “My house in California used to leak. Somewhere between sieve and submarine should be okay.” For a moment he laughed before returning to his dark intensity. No detail was too small. The tiles and railings were shipped to the sites packed in cardboard. That was wasteful. It took time to pack things and then unpack them. Get rid of the cardboard, he said, even at the warehouses. They should send him pictures from the factories, warehouses, and sites each week showing that they were no longer using cardboard.
“We need to get the engineers who designed this system to come out here and see how hard it is to install,” he said angrily. Then he erupted. “I want to see the engineers out here installing it themselves. Not just doing it for five minutes. Up on roofs for days, for fucking days!” He ordered that, in the future, everyone on an installation team, even the engineers and managers, had to spend time drilling and hammering and sweating with the other workers. When we finally climbed back down to the ground, Brian Dow and his deputy Marcus Mueller gathered the dozen engineers and installers in the side yard to hear Musk’s thoughts. They weren’t pleasant. Why, he asked, did it take eight times longer to install a roof of solar tiles than one with regular tiles? One of the engineers, named Tony, began showing him all the wires and electronic parts. Musk already knew the workings of each component, and Tony made the mistake of sounding both assured and condescending. “How many roofs have you done?” Musk asked him. “I’ve got twenty years of experience in the roof business,” Tony answered. “But how many solar roofs have you installed?” Tony explained he was an engineer and had not actually been on a roof doing the installation. “Then you don’t fucking know what you’re fucking talking about,” Musk responded. “This is why your roofs are shit and take so long to install.”
The one-nail idea proved to be unworkable, failing during installation rather than requiring a hurricane. Musk’s intervention did result in reduced installation time, but he never got anywhere near the goal of 1,000 roofs per week. A year after the above events, and following the firing and replacing of quite a few top managers, the company was at 30 roofs per week.
(We tried and failed to get a Tesla solar roof for our house in Maskachusetts. See Tesla Solar Roof (the price is not the price). Here in Florida, we are theoretically using all solar power via paying a little extra every month. That extra money is funding a utility-scale solar array owned and operating by Florida Power & Light.)
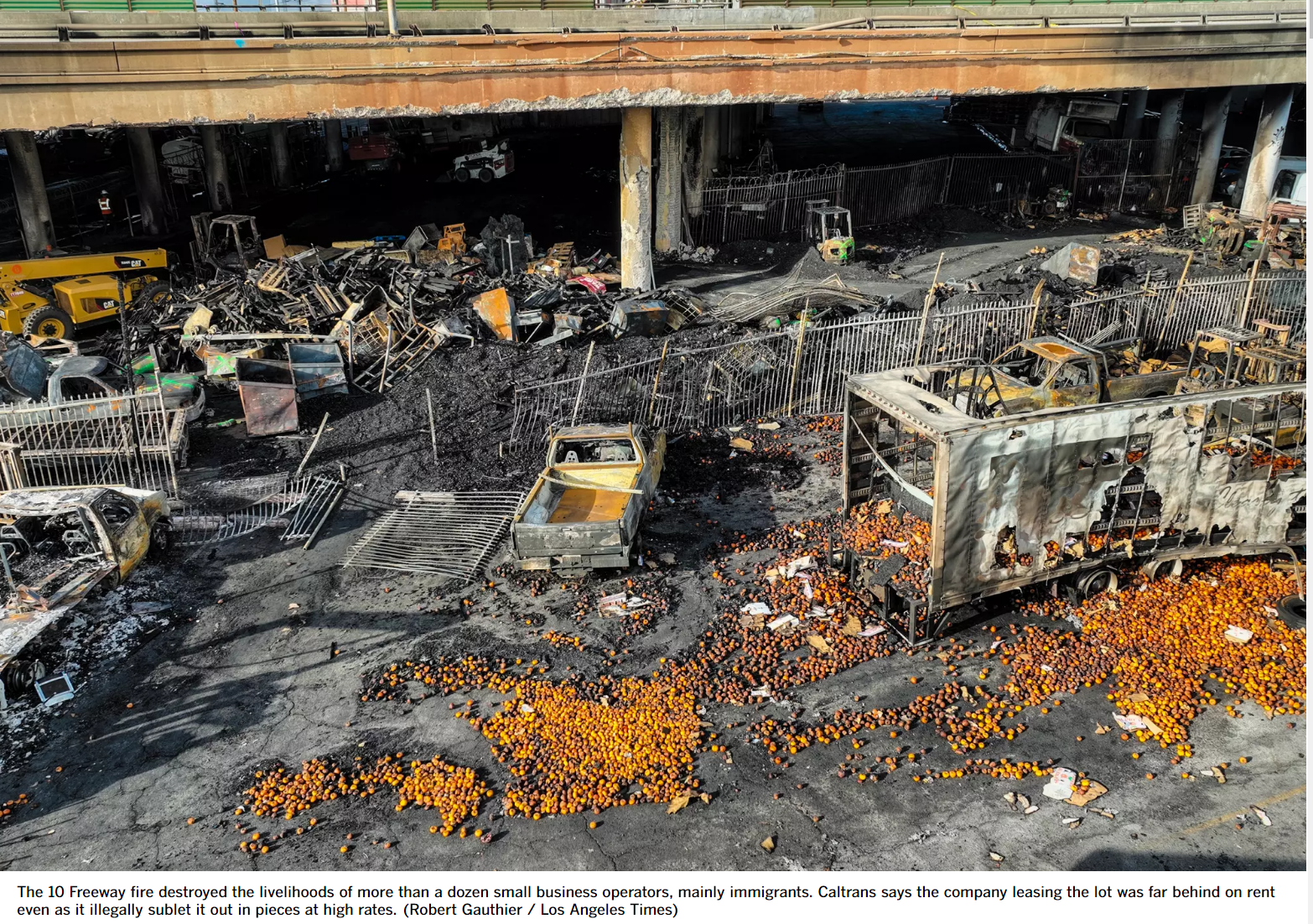
In the rush to expand the U.S. population, nobody seems to have noticed that attempts to reduce construction costs have failed. The single-family home is still stick-built by developers in more or less the same way as 100 years ago. The dream of lower cost via prefab did not pan out. Apartment buildings aren’t getting cheaper to construct, in constant dollars, I don’t think, but inflation has been reduced by lowering quality. Developers use flammable wood and sprinklers instead of concrete. “Why America’s New Apartment Buildings All Look the Same” (Bloomberg 2019)
Los Angeles architect Tim Smith was sitting on a Hawaiian beach, reading through the latest building code, as one does, when he noticed that it classified wood treated with fire retardant as noncombustible. That made wood eligible, he realized, for a building category—originally known as “ordinary masonry construction” but long since amended to require only that outer walls be made entirely of noncombustible material—that allowed for five stories with sprinklers.
By putting five wood stories over a one-story concrete podium and covering more of the one-acre lot than a high-rise could fill, Smith figured out how to get the 100 apartments at 60 percent to 70 percent of the cost.
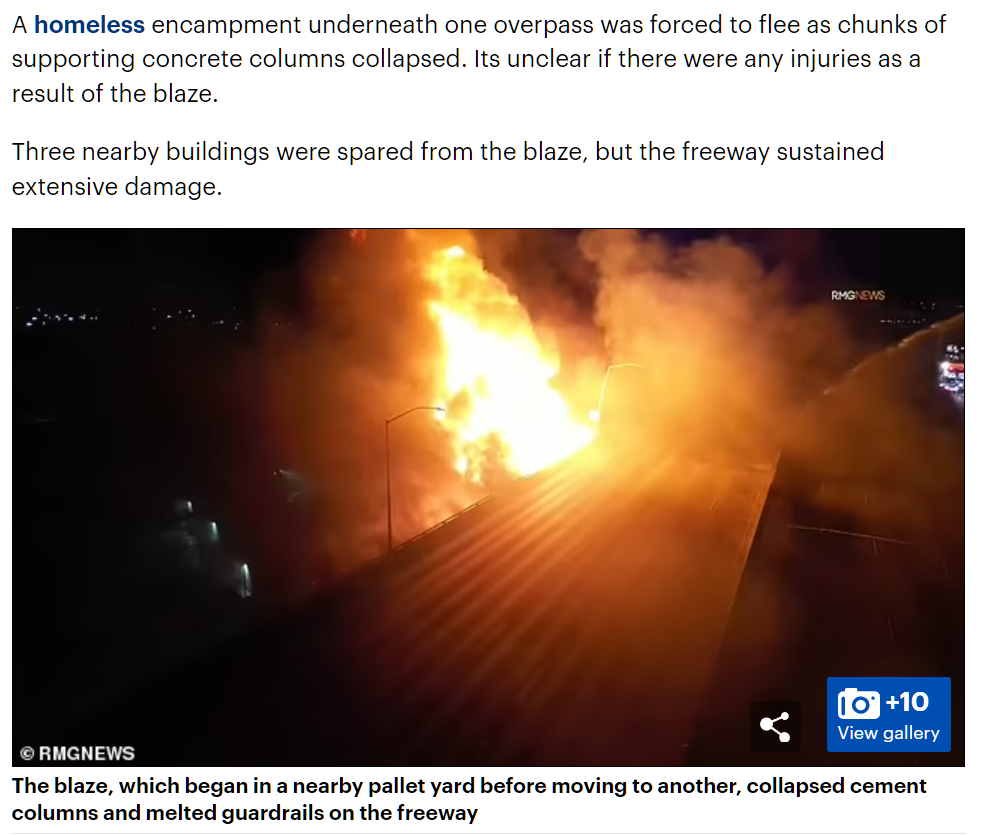
the buildings have proved highly flammable before the sprinklers and walls go in. Dozens of major fires have broken out at mid-rise construction sites over the past five years. Of the 13 U.S. blazes that resulted in damages of $20 million or more in 2017, according to the National Fire Protection Association, six were at wood-frame apartment buildings under construction.
Maybe these buildings won’t burn, but I expect them to degrade and sag more than a concrete apartment building would and be more resistant to rehab.
So… even our most successful innovator, backed up by $billions in capital, hasn’t been able to scratch, much less dent, the problem of housing costs being far higher than what immigrants can afford. And yet we continue to keep our border open.
Health care, obviously, is not affordable for today’s typical migrant, though the true cost is often disguised either by an employer or the government (Medicaid). Let’s also look at car prices. A car is the typical family’s third largest expense after housing and health care. It seems unfair to compare today’s pavement-melting SUVs to the cars of 1965. Maybe we could look at the bottom end of today’s car market as a comparable. CNBC says that this is 30,000 Bidies. That translates to about $5,500 in 1965 dollars (BLS). How much did a car cost in 1965? Hemmings says that a Corvette cost $4,223 in 1965 while a Mustang with a V-8 was $2,734. A basic Dodge Dart was $1,959 and a full-sized Chevy Impala was $2,295 (I think both would seat 6 humans, so they actually had more utility than today’s cheap cars!), according to this source.
So… the costs of producing all of the basics of American life have gone up, in real terms, since the modern immigration wave began, we do not seek to preferentially admit those who are likely to earn higher incomes, and even heroes such as Elon Musk can’t get the construction industry out of its productivity stagnation.
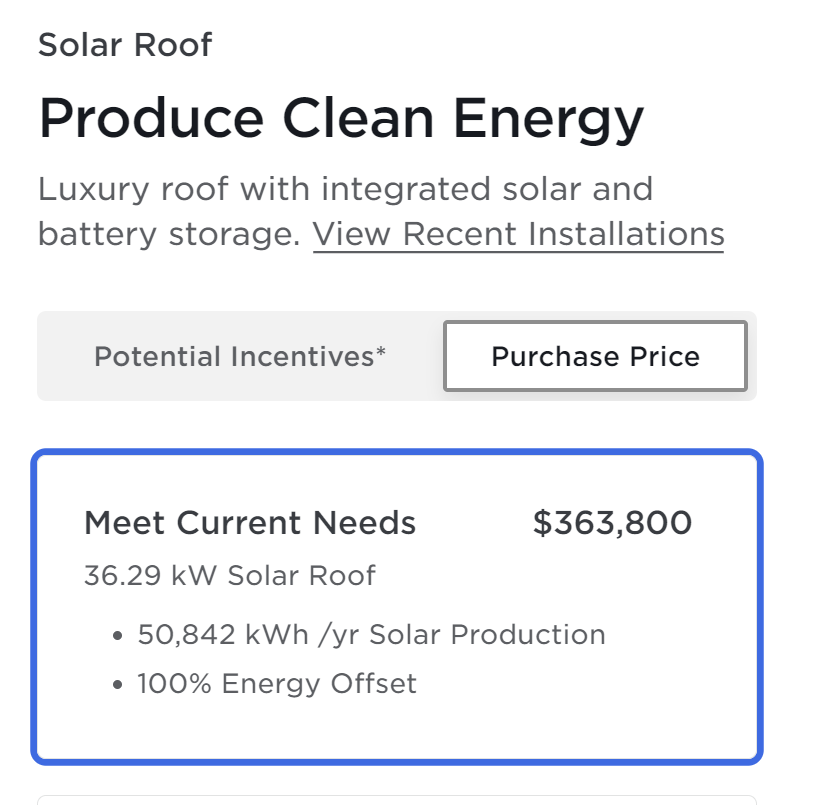
As there is no Spanish tile option for the Tesla solar roof, I don’t think that we would be able to get one. I typed in some data on our house, including that we pay $600/month for electric (the average number might be closer to $500) and got a quote from their web site:
If we assume a zero interest rate environment, the purchase price works out to 606 months of electric bills. The roof then pays for itself in 50 years. Perhaps it would be fairer to subtract the likely cost of a new tile roof since we will need one of those eventually. Let’s call that $80,000. Now we’re down to a 39-year payback period. This is before considering the subsidies from working class renters that our rulers have generously decreed.
Related:
Full post, including comments