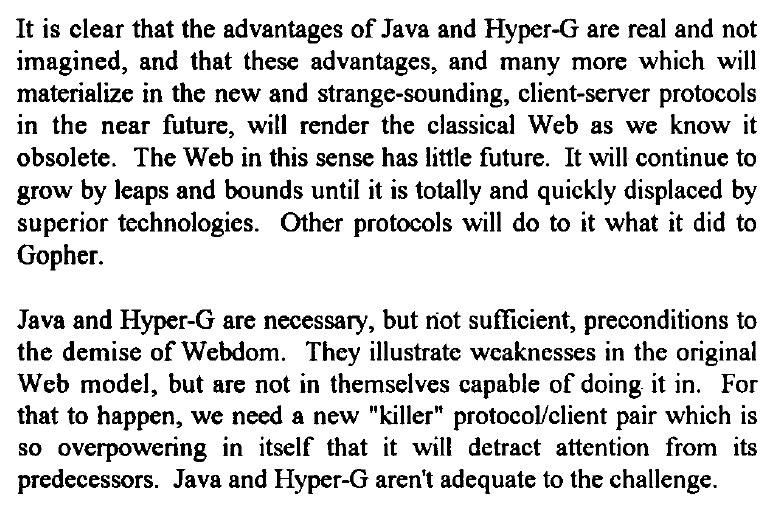
Remember to listen to the credentialed experts, such as Hal Berghel, Ph.D. computer nerd. A 1995 academic paper… “The inevitable demise of the Web”:
There is no doubt that the fastest growing part of the Internet is the World Wide Web. From its inception in 1990, the Web has established itself as the leading packet hauler on the Internet, passing beyond FTP, Telnet, WAIS Gopher and all of the other, more established Internet client protocols. The reason for this success is that the Web has established itself as the standard unifying environment for the Internet’s digital riches.However, the days of the Web are numbered. The technology behind the Web is outdated already and may not survive the decade. The current growth rate, which some estimate at 15% per month, suggests that if the end of the Web is to come soon, it will likely be cataclysmal. If this seems unrealistic, consider that this fate befell Gopherspace. As Figure 1 shows, Gopher lead the Web in packet volume as late as March, 1994. In the following twelve months Gopher presence on the Internet all but disappeared. Life cycles are accelerated to frightening paces on the Internet.
Dr. Berghel predicts that, with a little more innovation (from funded academic research?), the muscular connection-oriented Hyper-G protocol will crush HTTP and Java will replace HTML.
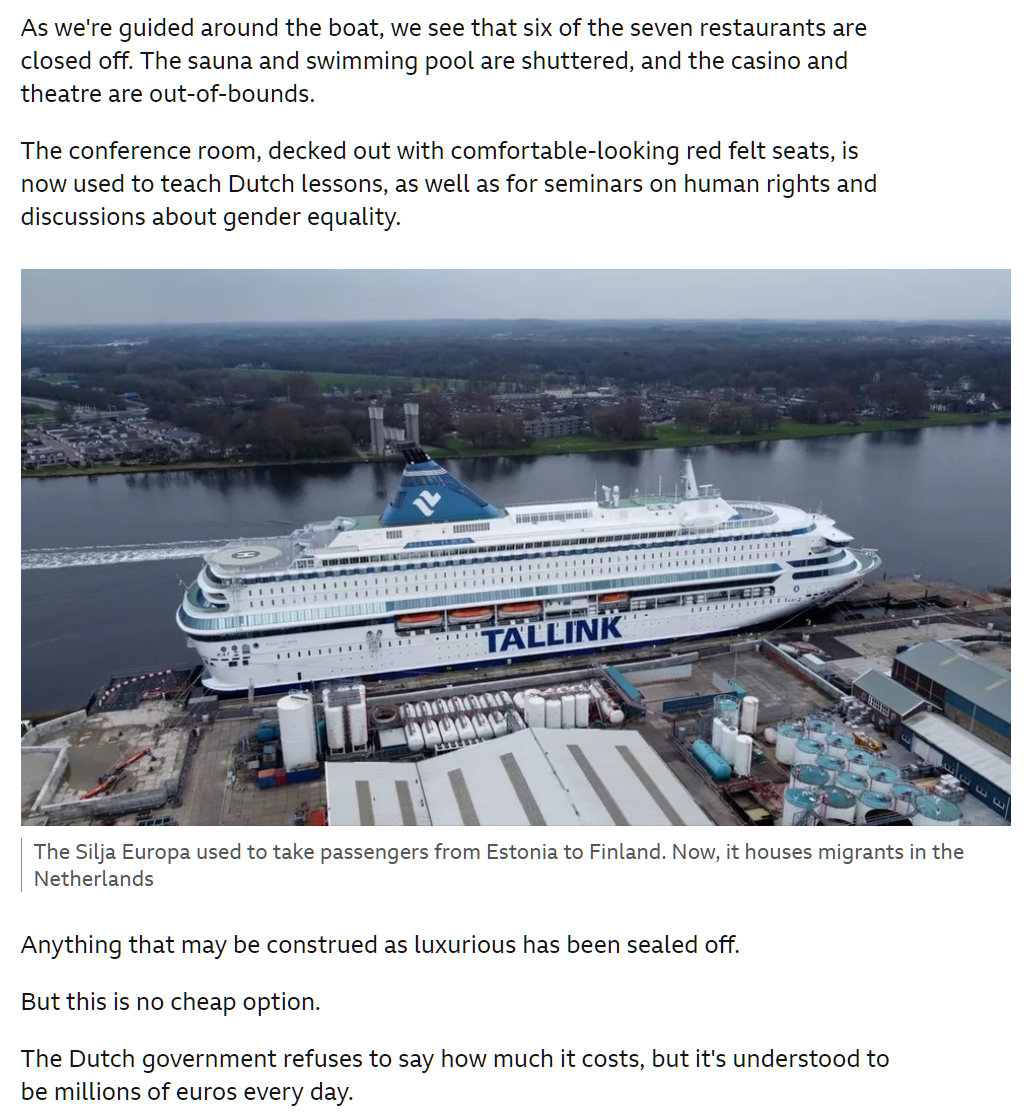
His conservative VVD party had been trying to limit the flow of asylum seekers, following a row last year about overcrowded migration centres.
This week Mr Rutte tried to force through a plan which included a cap on the number of relatives of war refugees allowed into the Netherlands at just 200 people per month.
But junior coalition partners the Christian Union, a pro-family party, and the socially liberal D66, were strongly opposed.
A compromise proposal, known as the “emergency brake”, which would only trigger the restrictions in the event of an excessively high influx of migrants, was not enough to save the government.
The proposed law seems unworkable. What’s “excessive”? Roughly 27 percent of people who live in the Netherlands aren’t “Dutch” (stats). There was never a popular vote asking for this level of immigration or any other level. The native-born people with whom I have spoken so far have said that the country is too crowded with both low-skill migrants and mass tourists and that their desired number of both would be 0. None of them was ever asked “In an ideal world, what percentage of your neighbors would be from Africa and the Middle East?”
How does it look on the ground? I’m staying in a college town (Delft), but have seen no coffee shops or stores practicing Rainbow-first Retail (examples from Bozeman, Montana), which would be likely to offend Islamic migrants. Any trip by public transit includes companions who don’t appear to share Western sexual mores. Near the center of The Hague, the third-largest Dutch city:
Some 2.2 million people moved to the Southeast in just over two years. That’s roughly the population of Houston.
Maskachusetts did its share to unload rich people with lockdowns, mask orders, vaccine papers checks, and a recent boost to the income tax rate. Nobody on welfare would have had an economic motivation to move because welfare in Maskachusetts pays approximately 118 percent of the median wage, compared to just 40 percent in Florida and Texas (see Table 4 in this CATO report).
Massachusetts is buying billboard space in places like Florida and Texas with a clear message for Pride month. The billboards say “Massachusetts For Us All” and feature pictures of LGBTQIA+ couples in the Bay State.
“At a time when other states are misguidedly restricting LGBTQIA+ rights, we are proud to send the message that Massachusetts is a safe, welcoming and inclusive place for all.” Gov. Maura Healey said in a statement. “To anyone considering where they want to live, raise a family, visit or build a business – we want you to join us here in Massachusetts.”
The largest LGBTQ+ rights organization in the country issued a Florida travel advisory in May.
People who identify as lesbian, gay, bisexual, or transgender (LGBT) have higher rates of poverty compared to cisgender (cis) heterosexual people, about 22% to 16% respectively.
So… Massachusetts is spending taxpayer funds to recruit a low-income demographic, which will be great for those who qualify for the state’s comparatively lavish welfare benefits.
Here are the billboards. Note the implicit message that people should have sex only with those whose skin color matches their own and whose age is approximately the same as their own.
Is this appropriate 2SLGBTQQIA+ promotion? The sacred Rainbow appears next to an article about Jose Salvador Hernandez, whose alleged actions are nothing to be proud of:
Deputies were later called to a house for a burglary in progress and arrived to find two witnesses struggling with Hernandez, who had broken into the home, grabbed the teen, held her down, told her “just be quiet” and lifted up her shirt “with the intent to commit sexual battery,” the report states.
As of Tuesday morning, Hernandez was being held without bond in the BSO Main Jail on charges of sexual battery, false imprisonment, burglary with assault or battery and leaving the scene of a crash.
Local news tends to cover the worst side of human nature. Should local TV stations refrain from changing their Twitter icons to rainbows?
And finally, a story that doesn’t seem to fit under the Love Wins rubric:
Detectives accused Ramirez, who is a migrant from Guatemala, of raping the teenage girl early Sunday morning in Homestead, according to the police arrest form.
Here’s how it looks next to the rainbow flag:
Separately, when is Elon going to give us reactions other than “love”. I seriously doubt that 6 people actually “love” this story about Sarvelio Gabriel Ramirez.
Nominally “private” colleges and universities get so much money from taxpayers that they are essentially part of the government. Taxpayers fund tuition grants that go straight into the colleges’ pockets. Taxpayers subsidize student loans that boost revenue by letting students pay more. Taxpayers fund research grants from which universities extract “overhead”.
All persons born or naturalized in the United States, and subject to the jurisdiction thereof, are citizens of the United States and of the State wherein they reside. No State shall make or enforce any law which shall abridge the privileges or immunities of citizens of the United States; nor shall any State deprive any person of life, liberty, or property, without due process of law; nor deny to any person within its jurisdiction the equal protection of the laws.
College admission isn’t exactly a “law”, but various cases have been decided in which this clause was applied to government programs generally, e.g., forcing states to allow same-sex marriage (and, eventually, throuples?). It wouldn’t be okay for the FAA to say “Your mom held a pilot certificate so therefore we’re going to let you have a pilot certificate at 35 hours instead of the usual minimum of 40.” Nor could the FAA say “We’re cutting you slack on the practical test because you paid $1 million in federal income tax last year.” Why is it okay for government-funded schools, such as Yale and Stanford, to say “We’re going to lower the bar for you because your parents attended and/or donated”?
Is the answer simply that no high-scoring-but-rejected-by-Yale applicant ever sued and obtained discovery showing that (1) second-rate legacy kids got admitted instead, and (2) Yale is firmly entrenched underneath a shower of government money?
“Elite Colleges’ Quiet Fight to Favor Alumni Children” (NYT 2022): Describing its incoming class of 2025, Yale boasted that its students hailed from 48 states, 68 countries and 1,221 high schools. What’s more, the university announced last year, 51 percent of the class identified as students of color. … 14 percent were the offspring of a Yale graduate, receiving the kind of admissions boost also used at other elite institutions.
The Son Also Rises: economics history with everyday applications (work by UC Davis economists that suggests a rational basis for legacy admissions: success is heritable, independent of how much money a child receives from parents; i.e., the characteristics necessary to succeed are mostly genetic and a high-scoring applicant from an unsuccessful family will likely eventually revert to his/her/zir/their family mean)
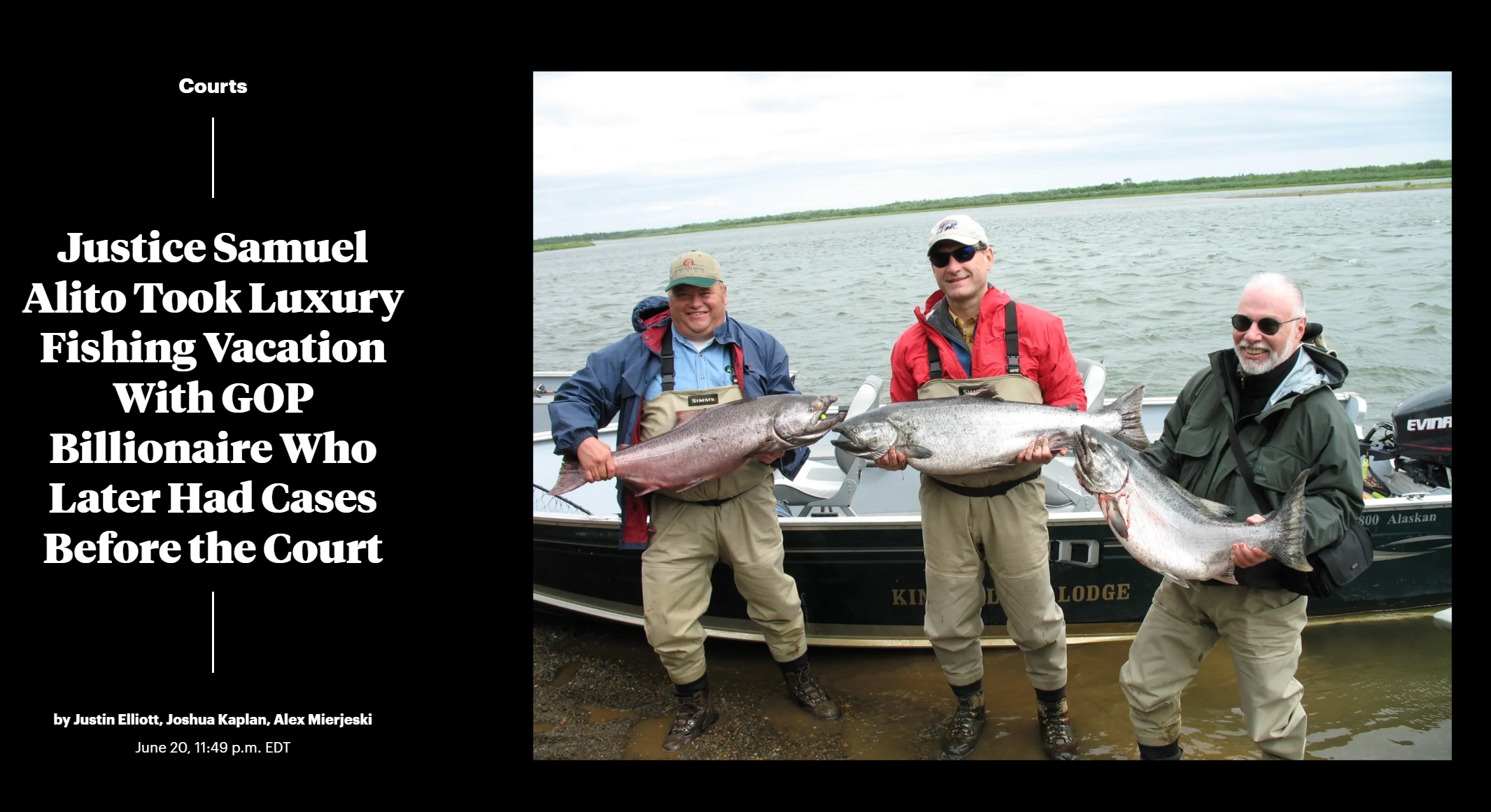
I always wondered why Supreme Court Justices didn’t quit their $400,000ish/year (total compensation) jobs and become law firm partners making $5 million/year arguing cases. Why live like civil servants when they could easily be living the multimillionaire lifestyle? And why not retire prior to becoming 98% dead? Recently we’ve learned the answer: they’re living like billionaires just as long as they keep sitting on the Court. Examples: “I shot myself a deer,” Elena Kagan said of a recent big game hunting trip with the conservative justice [Scalia] in Wyoming.” (Atlantic) and “Justice Samuel Alito Took Luxury Fishing Vacation With GOP Billionaire Who Later Had Cases Before the Court” (ProPublica).
If ethics rules were changed so that Supreme Court Justices couldn’t spend weekends and vacations on Gulfstream G700s, I wonder if they’d retire at a more typical age and/or leave government at 60-65 to earn some big $$ in the private sector before hanging up their pens.
Here’s one of our heroes on a July 2008 trip to a $1,000/day fishing lodge in Alaska:
(i.e., right before the world was about to melt down for the peasants)
From the ProPublica article:
“If you were good friends, what were you doing ruling on his case?” said Charles Geyh, an Indiana University law professor and leading expert on recusals. “And if you weren’t good friends, what were you doing accepting this?” referring to the flight on the private jet.
If nothing else, I guess we can be sure that our legal system will remain friendly to the interests of billionaires!
For British Readers: Happy Traitorous Rebellion Day. For Americans: Happy Great Patriotic Revolution Day.
One of the freedoms for which we ostensibly rebelled and that would not have been available had we stayed part of the British Empire is enshrined in our First Amendment. We are informed by the New York Times that, apparently contrary to the Constitution, books have been banned in Utah and that residents of the state no longer have “freedom to read”. “Book Bans Rising Rapidly in the U.S., Free Speech Groups Find” (April 2023):
Seven states, including Florida, Tennessee, Oklahoma and Utah, passed laws last year that impose limits on material in libraries, according to analysis done by EveryLibrary, a political action committee for libraries. This year, the group is tracking 113 bills across the country that it says would negatively impact libraries or curtail people’s freedom to read.
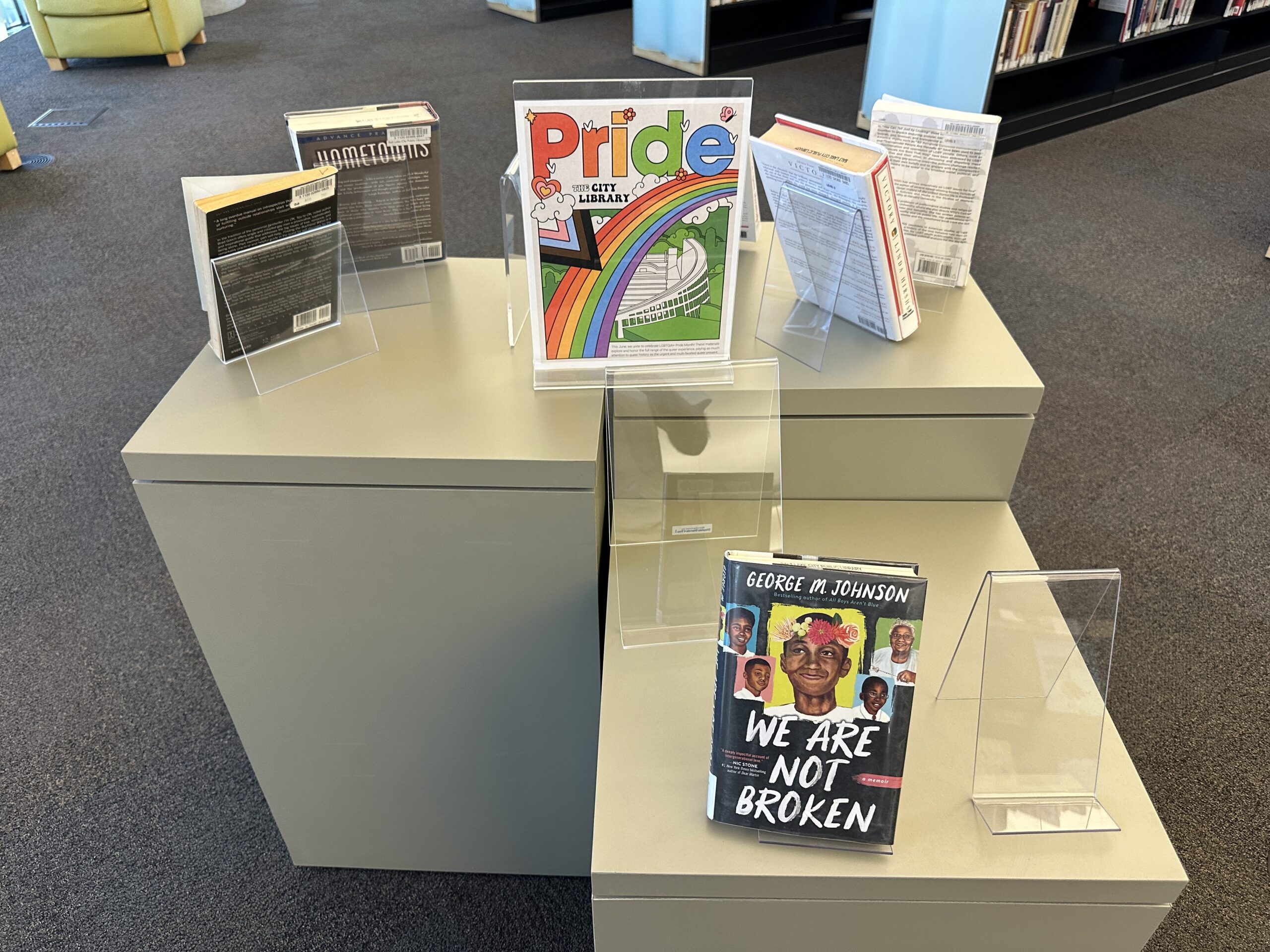
Florida was already covered here (see Palm Beach County Library Kids’ Section). Below are some photos from a June 15, 2023 visit to the public library in Salt Lake City, Utah (designed by Moshe Safdie). The atrium is inspiring, but the roof deck sadly closed for repairs in November 2022. A librarian explained that the repairs won’t begin until August 2023 and “it’s a government project so who knows how long it will take.”
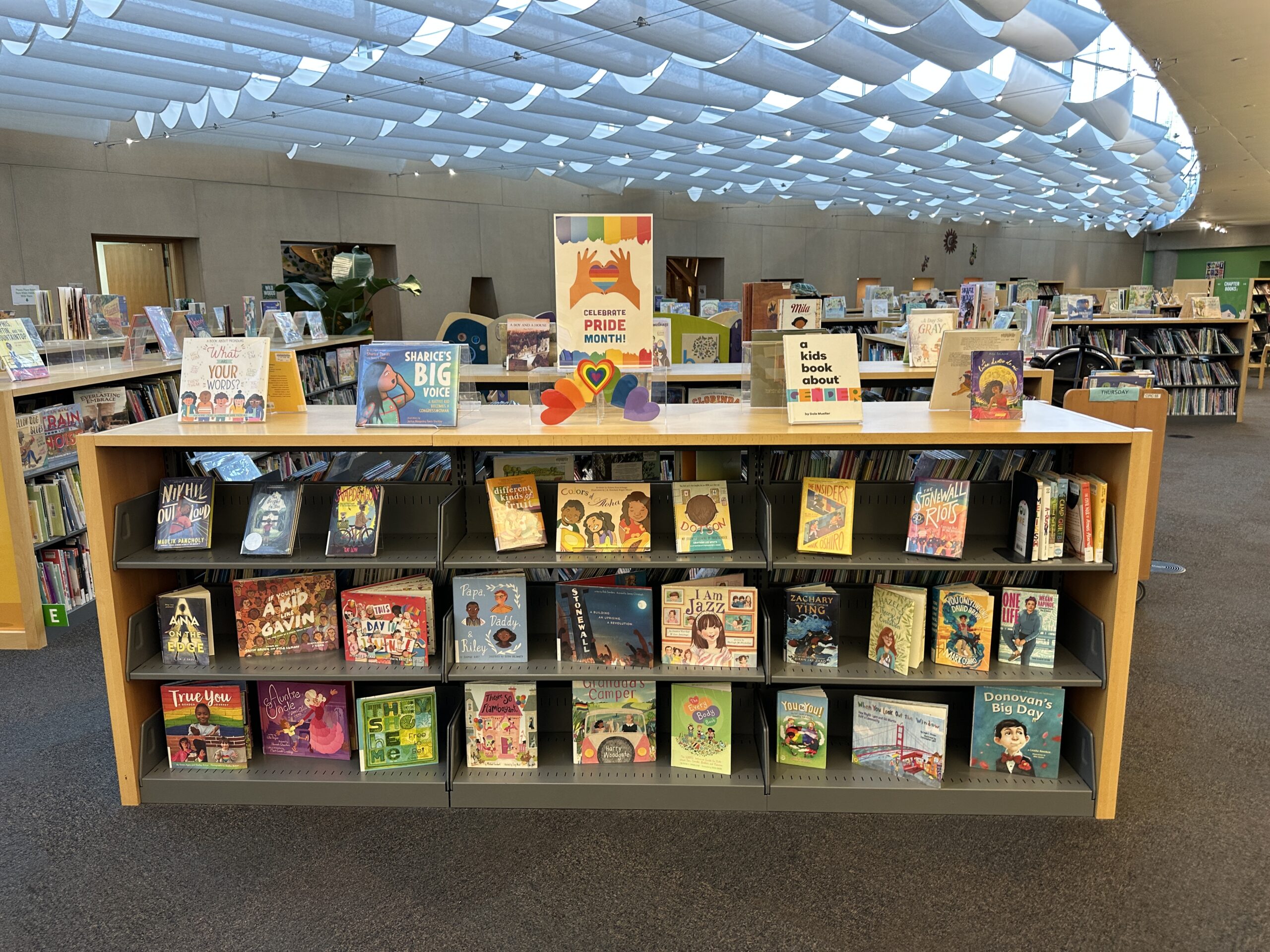
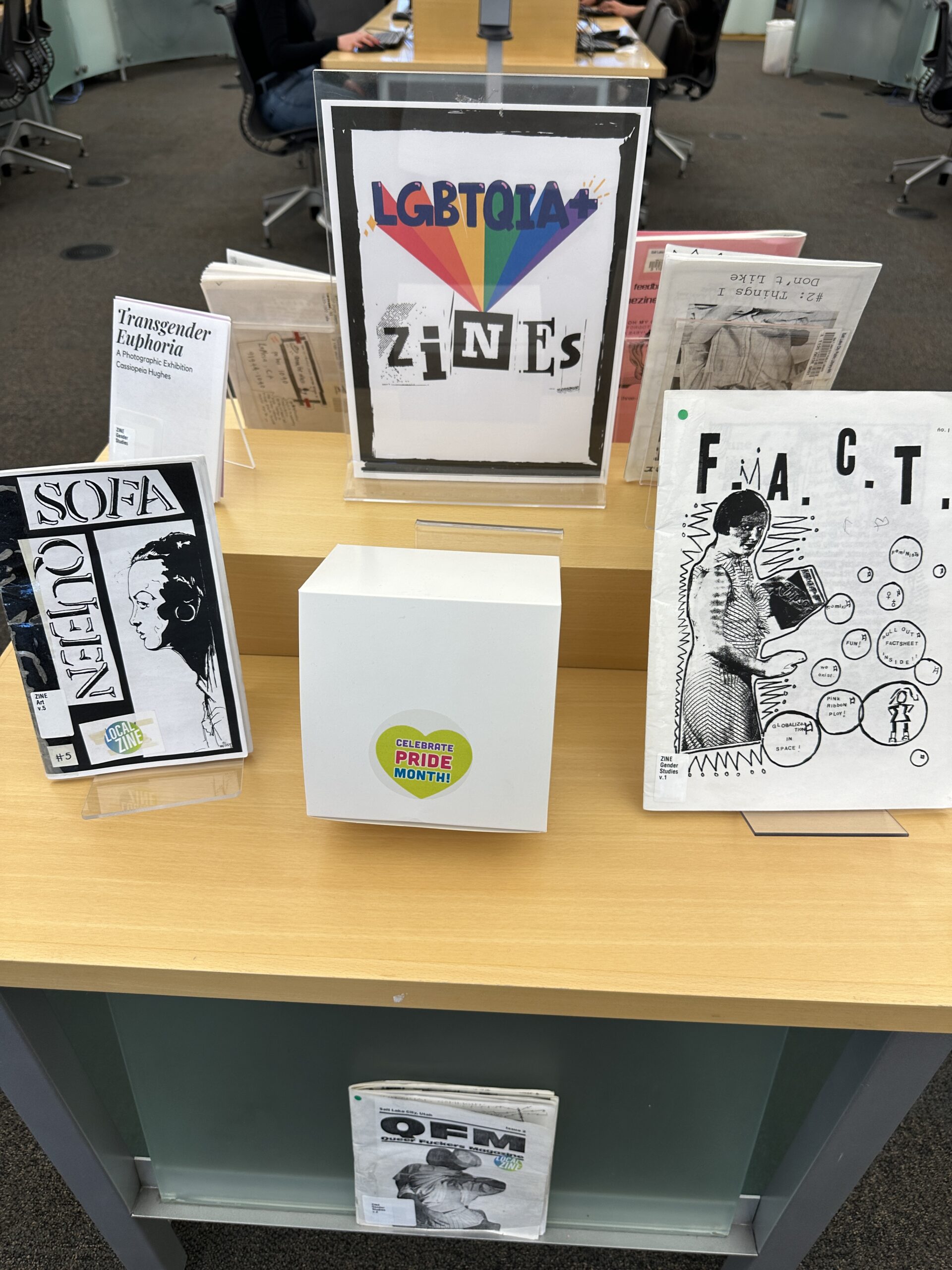
The first thing that a family sees on entering the kids’ section, which is downstairs, is a “picture book” cabinet with a “Celebrate Pride Month” sign on top.
The books featured include Different Kinds of Fruit (a sixth grader learns that her father is trans), Donovan’s Big Day (“Donovan’s two moms are getting married”), They She He Me: Free to Be! (a book about gender identity that Amazon customers are using with 4-year-olds), and A Kids Book About Gender (“it’s meant to help kids and grownups understand gender and create an open and safe environment for kids to question, experiment, and discover their authentic selves.”).
A child of perhaps 3 wears a mask and is joined by a librarian (far left of second image):
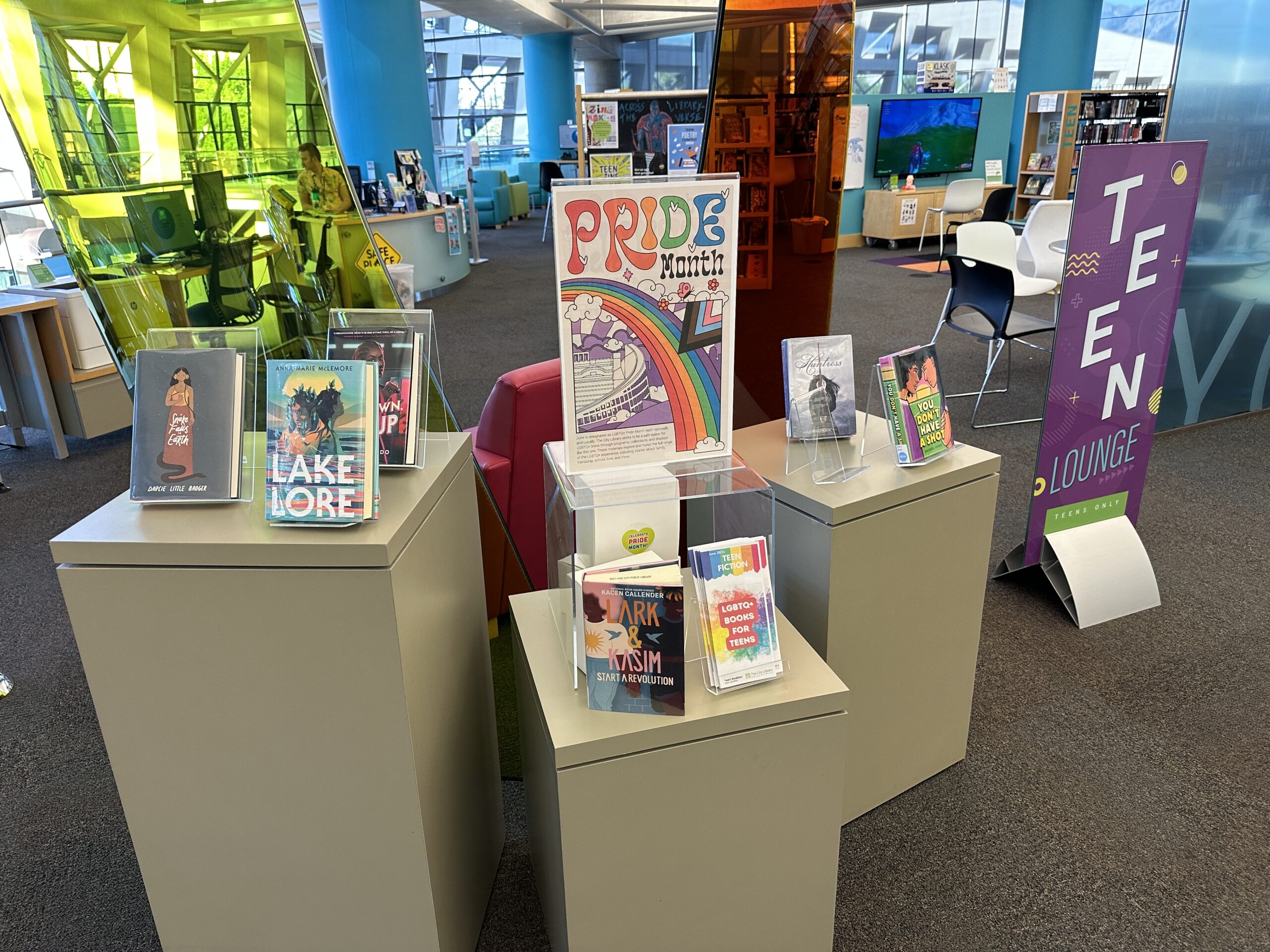
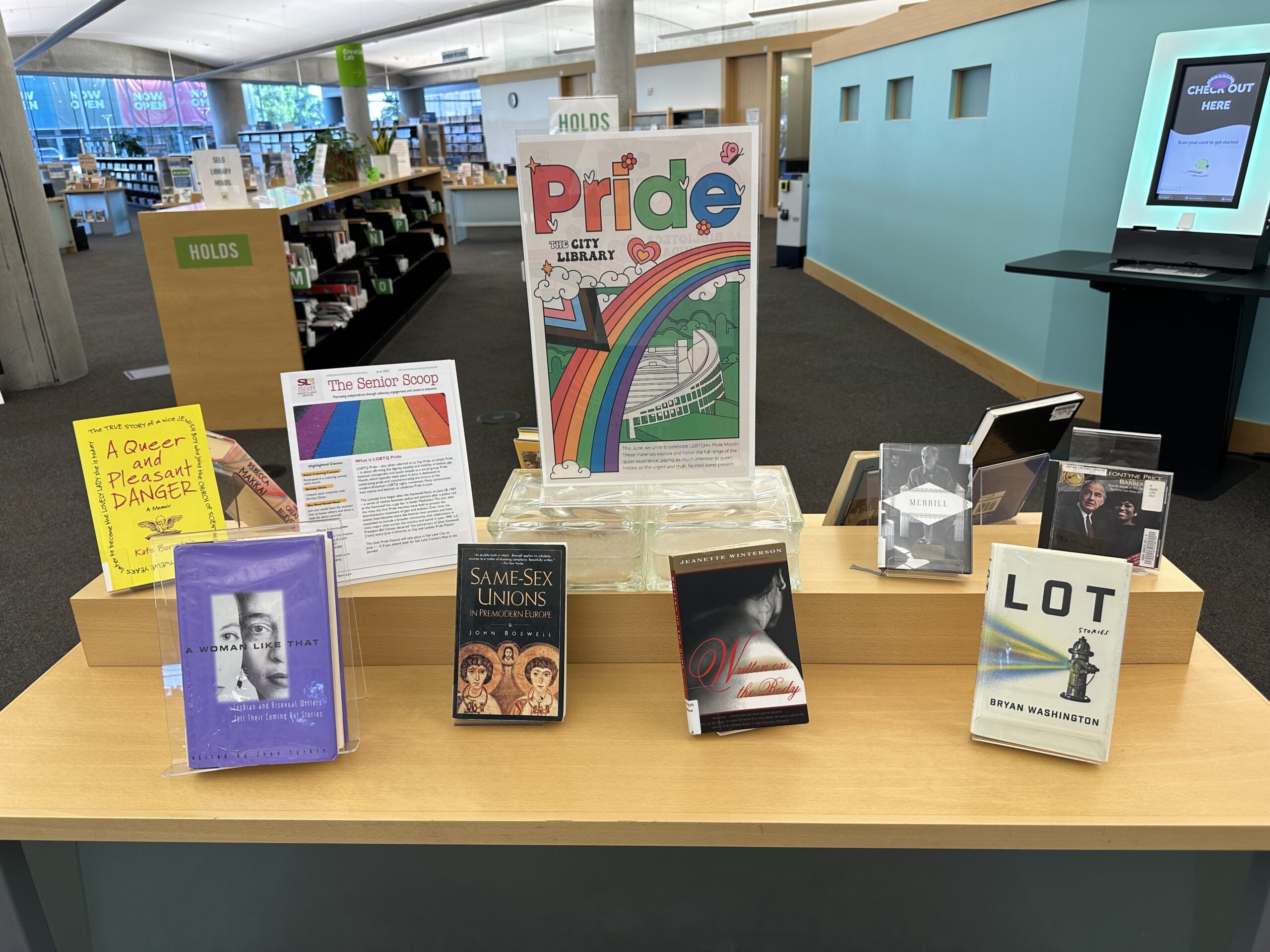
How about the Teen section? It is impossible to enter without first paying obeisance to Rainbow Flagism:
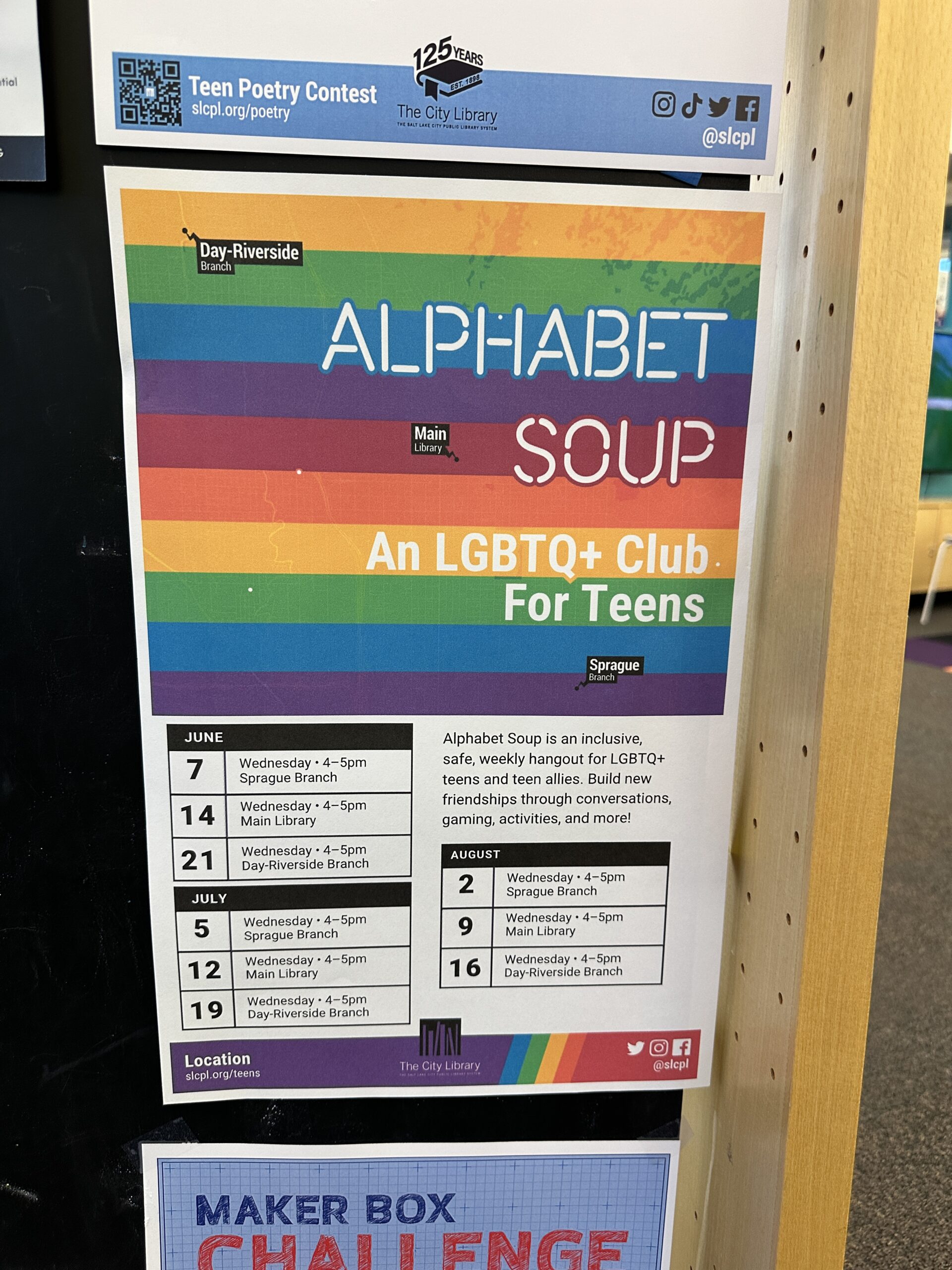
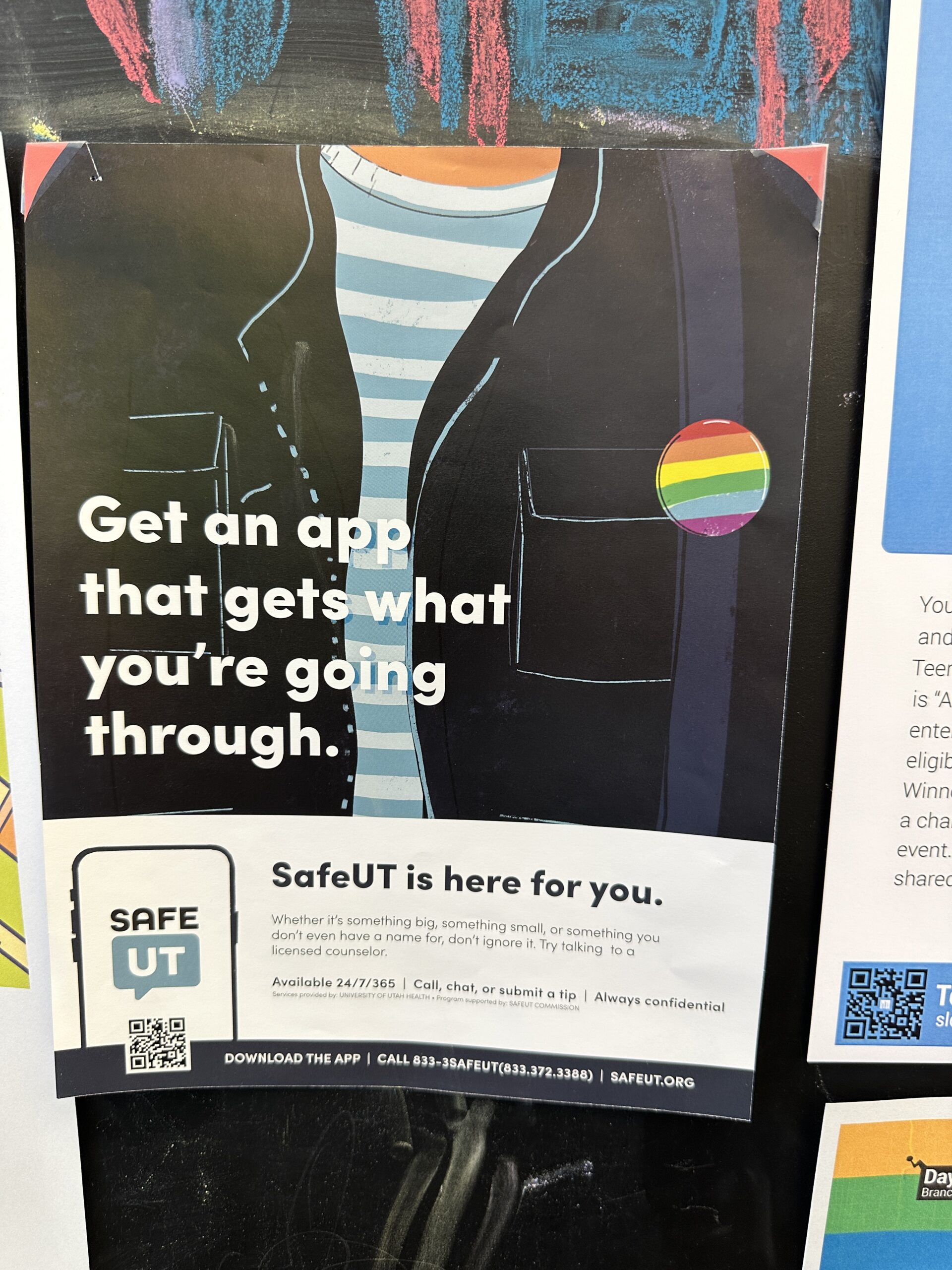
Once inside, the teen is invited to join 2SLGBTQQIA+ clubs and download 2SLGBTQQIA+ apps.
On the same floor (featured in the center), but not within the teen lounge per se:
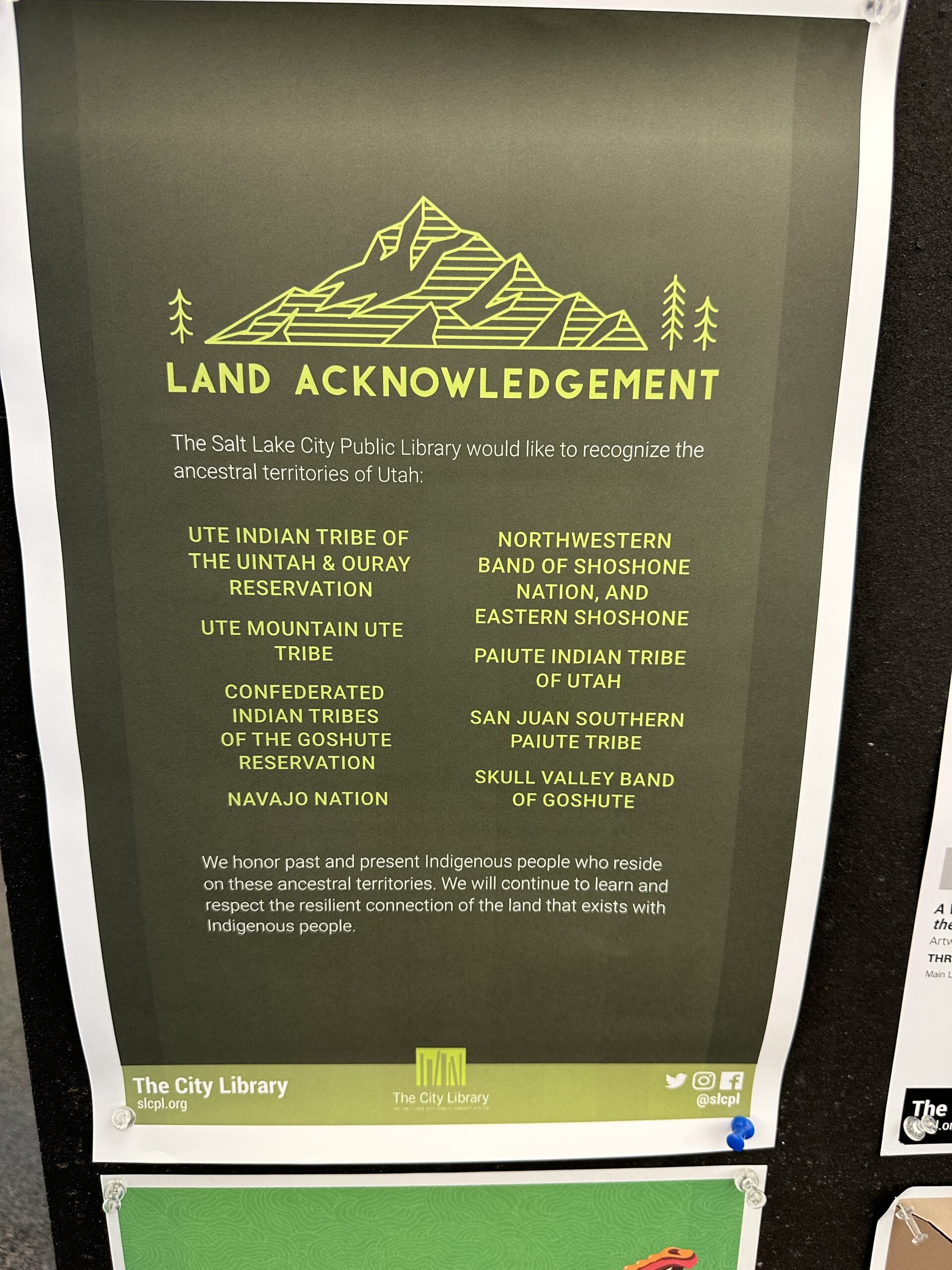
Teens are reminded on this floor that adults are raging hypocrites (admitting that they stole the land from the Native Americans, but refusing to give it back or at least pay rent):
(If you were Elizabeth Warren or some other Native American would you rather have white invaders “learn and respect” or have the white devils pay you in gold?)
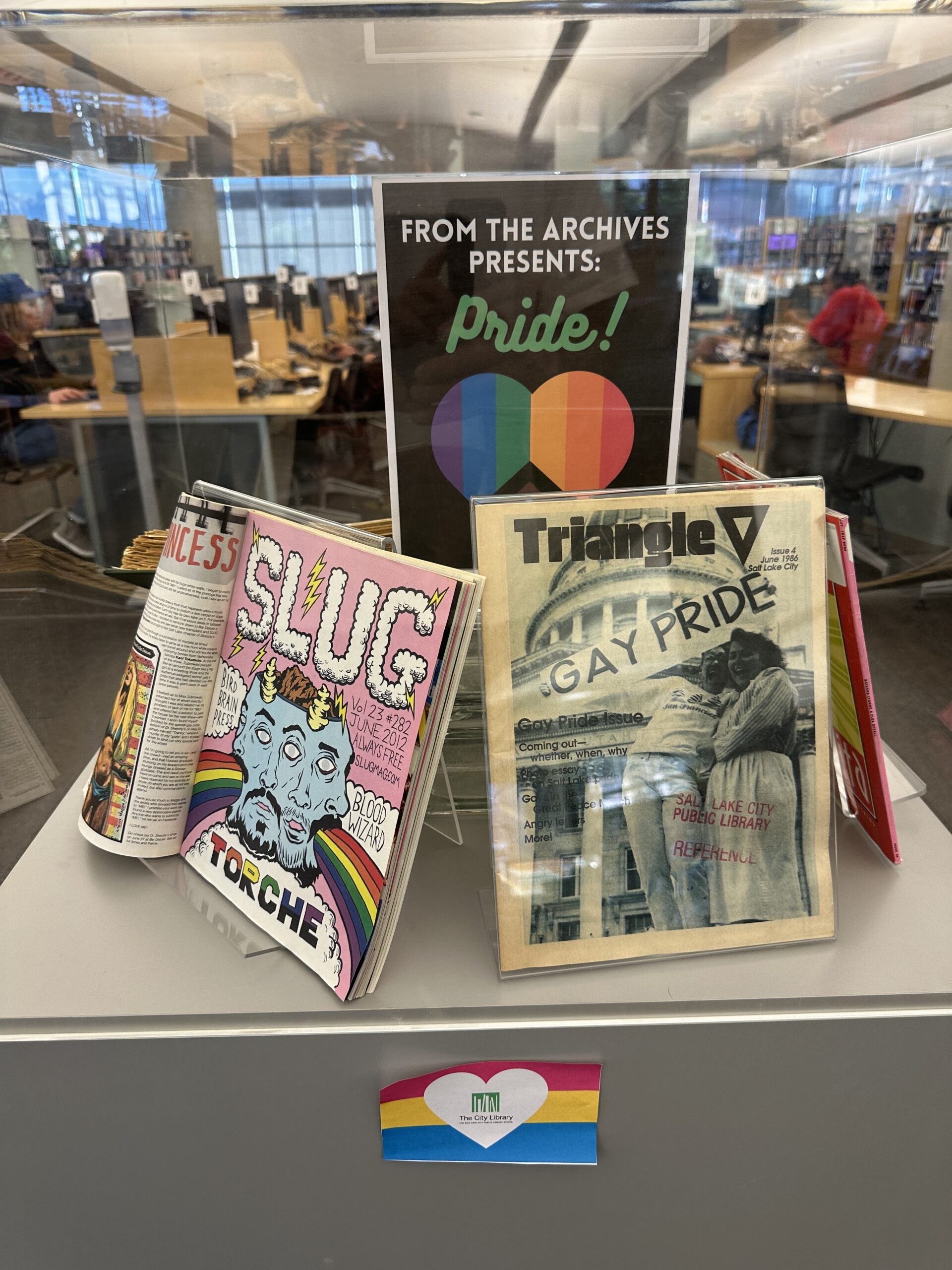
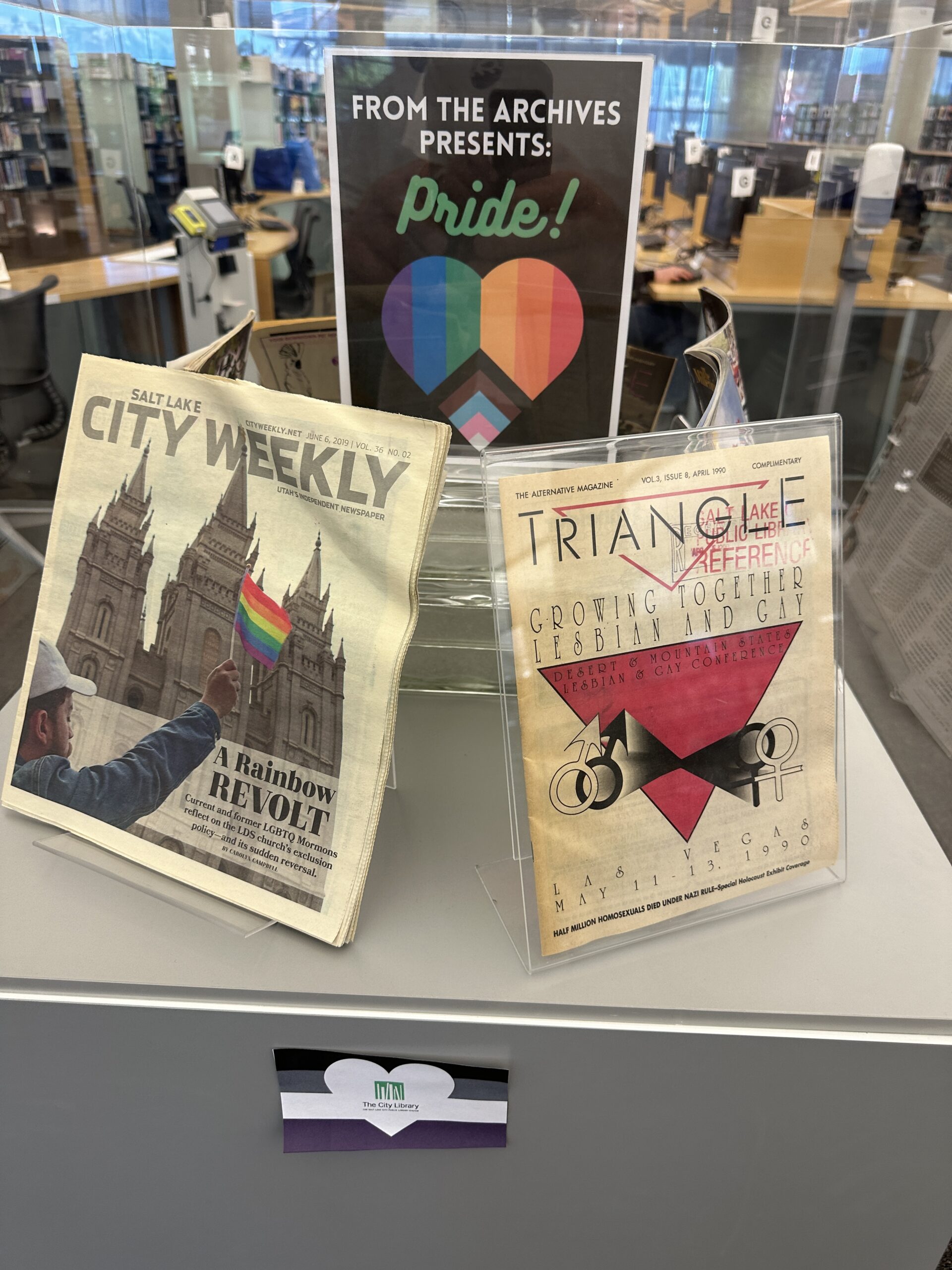
What about for adults? On the ground floor, just as you enter the library:
Upstairs, but not on the teen floor:
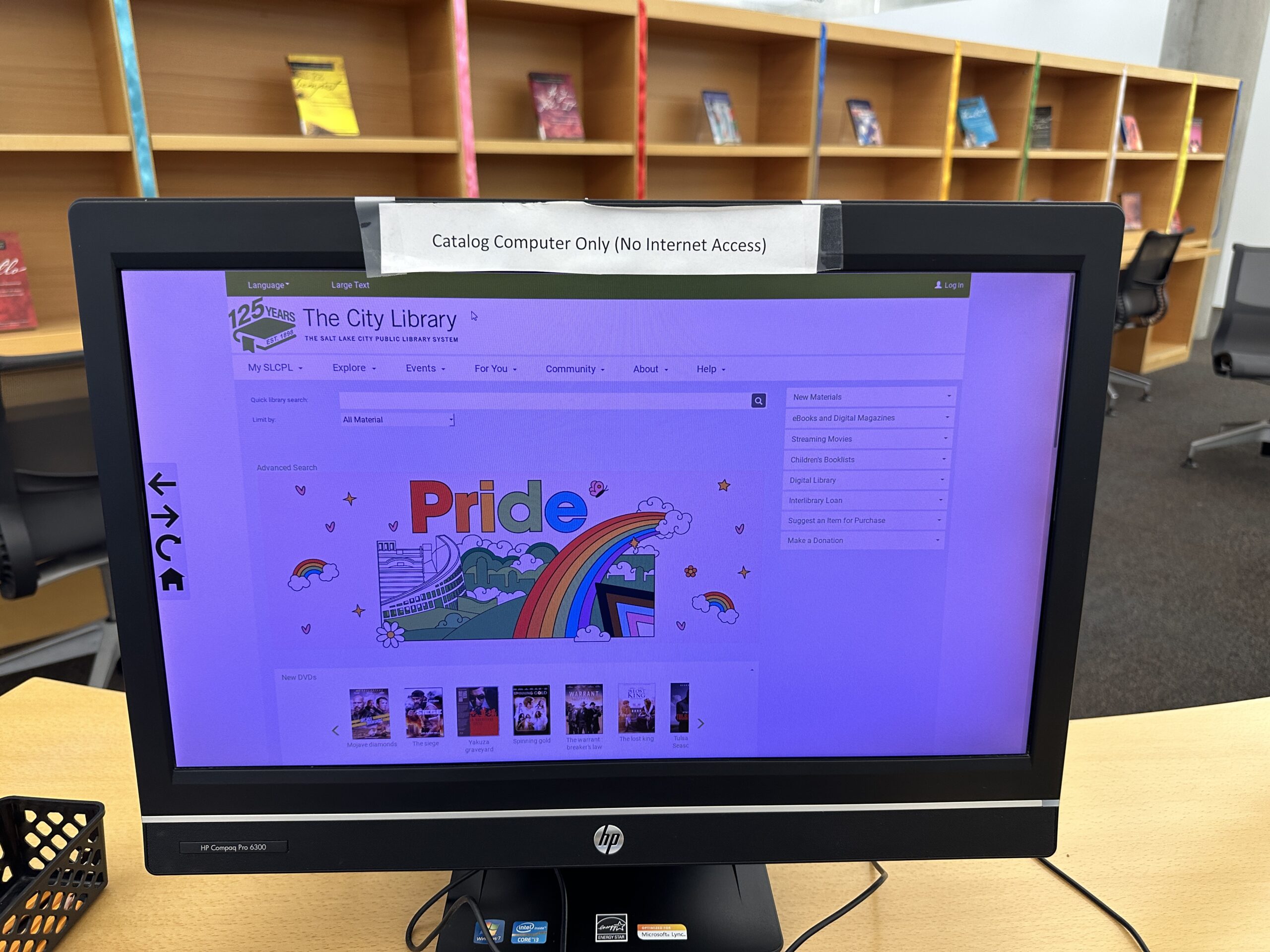
Whether adult, teen, or child, if you were to use a computer to search the catalog you’d have to first pay obeisance to Rainbow Flagism. The home screen through which you are required to pass:
The public web site has the Pride message, but as one of a set of messages that scroll:
Readers: In terms of freedom to read would we have been better off staying under the British umbrella and/or waiting for a peaceful separation as the Canadians did? Who currently has more freedom to read, Canadians or Americans?
(Speaking of Canadians and Utah, Senior Management covered our kids in so much zinc oxide during this recent trip that they looked like Justin Trudeau‘s cousins from a parallel universe.)
Folks: I’m heading over to mostly-peaceful Europe this week. I’ll be at the Delft University of Technology in Holland for a few days and then going to Ireland (Dublin, Sligo, and Belfast) for some aviation projects. If anyone would like to get together over there, please email philg@mit.edu.
Pickets and blockades of roads are often held outside refugee centres in working-class neighbourhoods but on Saturday activists marched in the heart of the capital.
“It’s not about racism. There is no room for them,” said Gavin Pepper, 37, as he and about 350 others denounced the increasing number of asylum seekers. “Why should migrants skip Irish people on the housing list? I won’t accept it.”
An acute housing and homelessness crisis has collided with the state’s struggle to accommodate Ukrainians and asylum seekers, fuelling accusations that foreigners receive preferential treatment.
Protesters also say centres with “unvetted” young male refugees make them feel unsafe. “I have five girls and two boys and the girls are afraid to go out at night,” said one man, who declined to give his name.
I won’t be staying in a work-class neighborhood, so I may not meet the migrants.
A new report from France’s Ministry of Interior quantifies the damage done after nearly a week of protests in response to the police killing of a teen of North African heritage.
The report, obtained by the French newspaper Le Parisien, recorded 5,662 vehicle fires and more than 1,000 damaged buildings.
Since rioting first broke out on Tuesday, police have made 3,354 arrests – 1,282 of which were in the Paris metro area alone, according to the report.
“Asian tourists, in particular, who are very concerned about security, may not hesitate to postpone or cancel their trip,” he warned. Didier Arino, managing director of the Protourisme firm said: “Tourists who know us well, like the Belgians or the British, who also have problems themselves in their suburbs, will be able to make sense of things”.
Our National Parks get less than 10 percent of their budget from entrance fees. In other words, people who don’t go to the parks are subsidizing people who do go to the parks. A 2015 report found that visitors paid $186 million in fees directly and $85 million via concessions (food and hotels) while the Park Service spent $3.1 billion.
Part of the reason for this is that prices are low. Not quite as low as in 1938, when the parks were free:
But an annual pass that enables 8 people in a minivan to spend 3-4 weeks in the parks is $80. I had already purchased a pass for the Vegas/Pahrump trip (Death Valley, Sheri’s Ranch to try to meet up with Hunter Biden, Corvette School, etc.) so it cost us $0 in fees to spend 3 weeks in the National Parks in June. Even if we had paid $80 that would have been less than the cost of housekeeping tips ($5 is the new $3).
Let’s assume a family of 4. What do the Navajo charge for them to look at something interesting? We took a one-hour tour of Antelope Canyon and it worked out to $100 per person. Here’s a photo from that excursion:
Let’s assume that a typical family won’t be able to pay $400 per hour every hour, but $100 per person per day is the “Navajo rate” for what could reasonably be charged. The National Park Service budget is up to $3.6 billion in Bidies. For the agency to be fully funded by visitors, therefore, they’d have to host 36 million person-days. Is that practical? State-sponsored NPR says that 312 million people visited in 2022. It is unclear if they’re counting how many days each person spent in the park and, of course, visitation would fall if Navajo pricing were established rather than give-away pricing, but it seems clear that the Park Service could easily fund itself from entrance fees.
For reference, the Chileans charge foreigners $35 per adult to visit their signature national park for one day. Even at Chilean prices it would seem that the NPS could easily be self-funded.
What about families where nobody has worked for 4 generations? How are they going to enjoy the Grand Canyon? As with museums, anyone with a SNAP/EBT card could be admitted for free.
What’s wrong with the current system? Nothing, if you’re a member of the elite! Since the NPS isn’t charging anything for park entry, the people who own hotels and restaurants in the parks (i.e., the cronies) can charge higher prices. It ends up costing about $1000/day to visit the parks in any degree of comfort, so the visitors themselves tend to be elite.
Gift shops at National Parks sell books, stickers, posters, and quilts featuring all of the parks for those who wish to try to hit them all (my favorite is a scratch-off). If you’re old and remember when the “National Park” designation was reserved for truly spectacular places you will greatly underestimate the challenge. There are now 63 National Parks. How is that possible? 63 places in the U.S. that deserve to be mentioned as peers to Yellowstone and the Grand Canyon?!?
It turns out that there has been a substantial amount of Parkflation.
Eero Saarinen’s 1965 Gateway Arch in St. Louis was redesignated from Jefferson National Expansion Memorial to Gateway Arch National Park in 2018 (Wikipedia).
Black Canyon of the Gunnison was a National Monument starting in 1933. Without any upgrades to the sights, which Coloradans say are worth a half-day visit, it became a National Park in 1999.
Cuyahoga Valley National Park is a set of hills cut through with highways just south of Cleveland. Half of Connecticut and all of New Hampshire qualifies as a National Park if this place does. From Wikipedia:
Cuyahoga Valley was originally designated as a National Recreation Area in 1974, then redesignated as a national park 26 years later in 2000, and remains the only national park that originated as a national recreation area.
We checked off the park on the way to Oshkosh 2021. It’s a pleasant place for an afternoon walk if you don’t mind being able to hear road noise.
The UNESCO World Heritage folks are more discriminating. Only 12 natural sites, all National Parks, make the cut:
Carlsbad Caverns National Park (1995)
Everglades National Park (1979)
Grand Canyon National Park (1979)
Great Smoky Mountains National Park (1983)
Hawaii Volcanoes National Park (1987)
Kluane / Wrangell-St. Elias / Glacier Bay / Tatshenshini-Alsek (1979, 1992, 1994)
Mammoth Cave National Park (1981)
Olympic National Park (1981)
Redwood National and State Parks (1980)
Waterton Glacier International Peace Park (1995)
Yellowstone National Park (1978)
Yosemite National Park (1984)
(One’s in Florida!)
Readers: What are your predictions for the next few U.S. National Parks? Here are mine:
Biden-Corn Pop National Park, centered on the swimming pool where our greatest president confronted a bad dude
Climate Change National Park in some of the neighborhoods of New Orleans that were flooded by Hurricane Katrina in 2005 (an event that would never have occurred but for human-caused climate change)
George Floyd National Park centered on the site of the current George Floyd Square
The southern edge of Vermilion Cliffs, as viewed when driving from Grand Canyon North Rim to Page, Arizona: