Pinflation II: the Millionaire machine
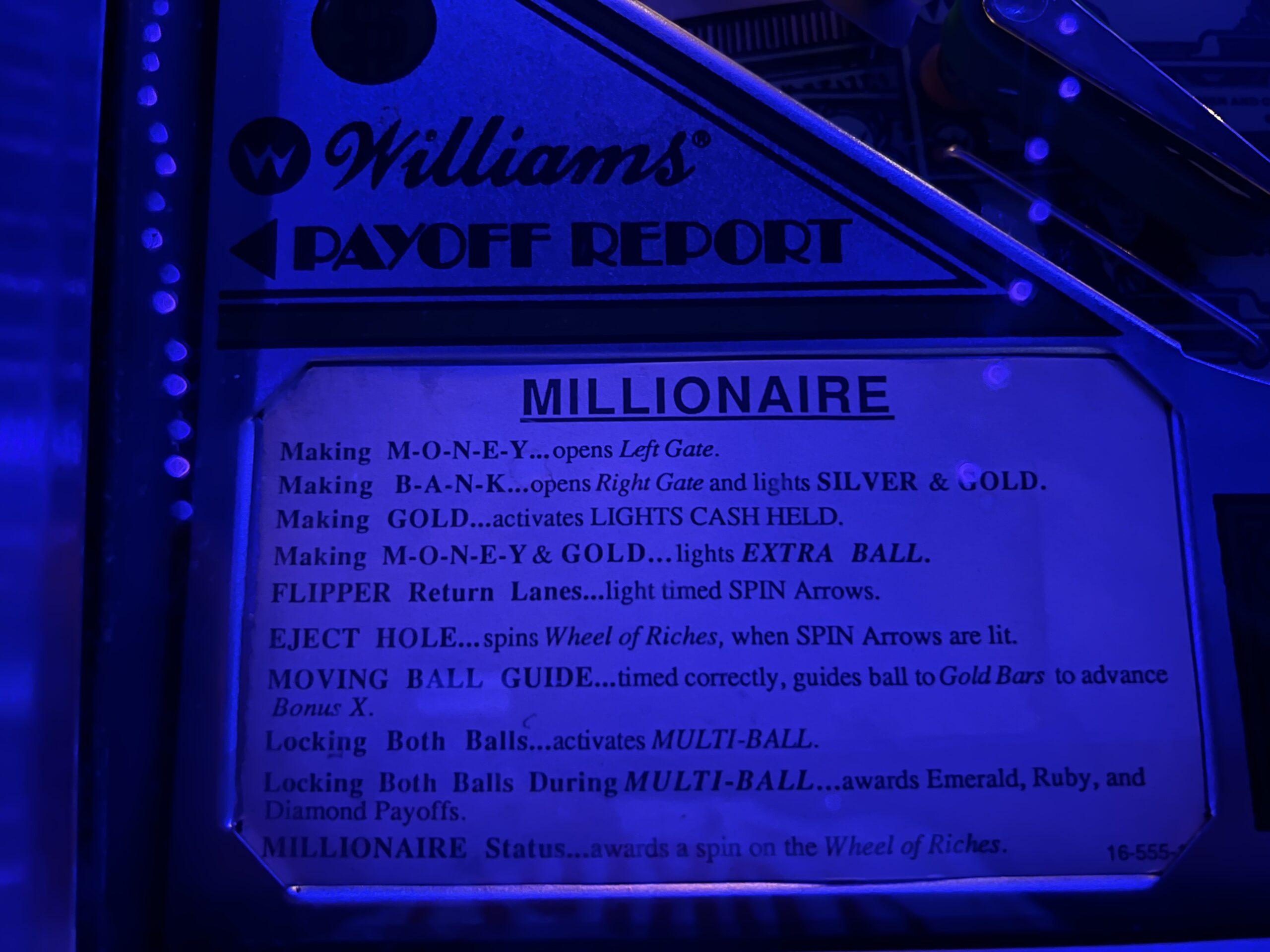
From an arcade in Stuart, Florida, the Millionaire pinball machine (1987) renamed “Billionaire”:


Related:
Full post, including commentsA posting every day; an interesting idea every three months…
From an arcade in Stuart, Florida, the Millionaire pinball machine (1987) renamed “Billionaire”:
Related:
Full post, including commentsInterview season has commenced, which means we get days, weeks, or even a month off to travel to residency programs. With the exception of a few specialities such as urology and ophthalmology, the Match starts when the Electronic Residency Application Service (ERAS) opens at the beginning of September and interview offers start shortly after the end-of-September application deadline. The application includes volunteer and professional experiences, research publications, and letters of recommendation from attendings. A letter from one’s medical school dean is required, but we are told that this is ignored by programs. We also have to submit a personal statement. Popular topics include challenges overcome [Editor: a victimhood narrative!] and motivation for becoming a doctor (“earn money” will not appear here). The less competitive programs will send their interview invitations first.
Students apply to as many as 90 programs and even more if they are applying to multiple specialities. Our Dean of Student Affairs sent an email out overviewing the process, highlighting that we are nearly guaranteed to match into a chosen speciality if we interview at 12 or more programs. “If by December 1st you do not have that many interviews, contact me.”
Most programs email four interview dates that fill up within hours. The Dean of Student Affairs recommends giving login information to a trusted family member to accept interviews as they come in case you are in the operating room and don’t open the email soon enough. One program sends more interview offers than slots. Lanky Luke responded within 30 minutes, but “I was waitlisted because they already filled.” Sarcastic Sally empathizes: “This happened to me too! I just don’t understand why a program would leave it to chance to decide who they interview. Select the better candidate. I don’t buy it that someone who responds within 30 minutes shows more interest in coming than someone who doesn’t respond for an hour.”
Every specialty and program has different interview date ranges. Our dean explains that around 2010 there was a movement to cluster interview dates by region to allow for decreased travel costs. For example, southwestern surgery programs would have their interviews clustered around one week but coordinated to avoid overlap. “They no longer do this,” said the dean. “Expect to spend $7,000 to $10,000 during interview season on hotels, cars, and airfare. This has been budgeted into the MS-4 cost of attendance so you can borrow more money if needed.”
I’m applying to general surgery, which requires 4 recommendations. Mine are from three surgeons, a research mentor, and, unconventionally, an internist with whom I worked frequently.
Statistics for the week… Study: 5 hours. Sleep: 7 hours/night; Fun: 2 nights. Dinner party with Lanky Luke and Sarcastic Samantha.
The rest of the book: http://fifthchance.com/MedicalSchool2020
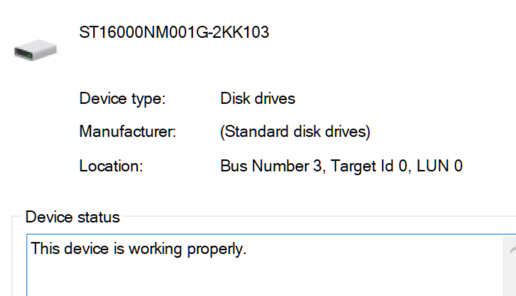
Full post, including commentsHere’s a riddle that I hope the Windows experts among us can help solve. I have an internal Seagate Exos 16 TB drive that is dedicated to Windows File History. It was installed in July 2021, assigned to R:, formatted as NTFS, and functioned just fine through mid-March. Now it doesn’t show up under “My Computer”.
Device Manager says it is “working properly”:
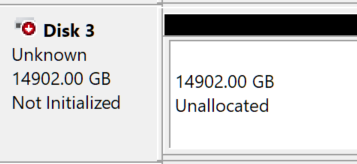
Disk Management can see it, but thinks that there is no partition on it:
Following Paul’s steps from the comment:
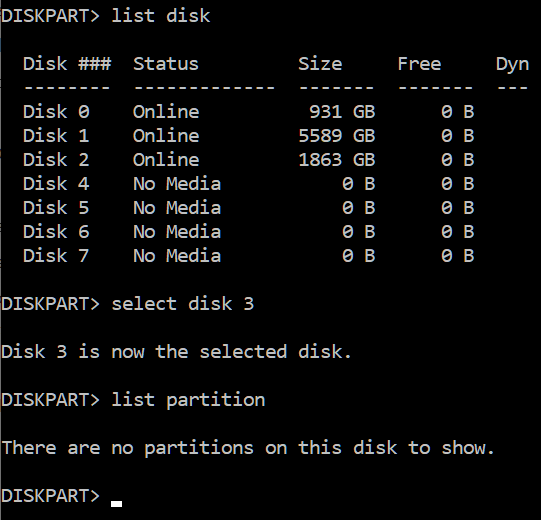
The two internal hard drive peers are shown (disks 1 and 2, but not the 16 TB drive that is the subject of this post).
Seagate offers free “SeaTools” software that could see the drive and blessed it with a green status check, but then failed it on a “short self test”.
I could start over and reformat it, but I don’t want to lose 9 months of file history. And I would like to know how the disk lost its memory of having an NTFS partition (not a good sign considering that the disk’s job is to hold a memory of my beloved files).
What should my next step be?
For the foreseeable “throw it out and buy a Mac” comments…
Six months ago, the New York Times’s in-house Nobel-winning economist wrote “Wonking Out: I’m Still on Team Transitory” (9/10/2021):
if we finally get this pandemic under control, the inflation of 2021 will soon fade from memory.
Professor Krugman was correct about Joe Biden getting the pandemic until control. When the Science-rejecting Donald Trump was in the White House 350,000 Americans died with/from COVID-19 in 2020. Due to President Biden’s leadership and the vaccines that He developed, we’re on track to suffer only roughly a third of a million deaths in 2022.
Professor Krugman also seems to have been correct in predicting “the inflation of 2021 will soon fade from memory”, but maybe that is because the inflation of 2022 has been so much more dramatic?
The Nobel laurate is back this week with “How High Inflation Will Come Down”. He starts by doing what my former hedge fund manager friend says nearly all analysts do, i.e., extrapolating from recent events:
Rising prices will get worse before they get better.
Something new for an American journalist or politician… He blames Russia:
Russia’s invasion of Ukraine has caused the prices of oil, wheat and other commodities to soar.
This time it is different:
Forty years ago, as many economists will tell you, inflation was “entrenched” in the economy. That is, businesses, workers and consumers were making decisions based on the belief that high inflation would continue for many years to come.
Things are very different now. Back then almost everyone expected persistent high inflation; now few people do. Bond markets expect inflation eventually to return to prepandemic levels. While consumers expect high inflation over the next year, their longer-term expectations remain “anchored” at fairly moderate levels. Professional forecasters expect inflation to moderate next year.
If the professional forecasters are good at their jobs, why aren’t they absurdly rich via trading on their own previous forecasts and, thus, retired from forecasting?
Nobel-grade thinking… Prices will go down as soon as prices go down:
A lot of recent inflation will subside when oil and food prices stop rising, when the prices of used cars, which rose 41 percent (!) over the past year during the shortage of new cars, come down, and so on. The big surge in rents also appears to be largely behind us, although the slowdown won’t show up in official numbers for a while. So it probably won’t be necessary to put the economy through an ’80s-style wringer to get inflation down.
Professor Krugman agrees with what Chauncey Gardiner pointed out, i.e., that there will be growth in the spring:
The inflation of 2021-22 looks very different, and much easier to solve, from the inflation of 1979-80.
What if it takes a few springs for inflation to subside?
Related:
Disney supposedly has cut its maximum capacity, but the new maximum still results in multi-hour waits for rides, up to a one-hour wait to get through security before even reaching the ticket booths, no way to get food without waiting in an epic line, etc.
We stayed at a hotel near Disney Springs in mid-March and would not have been able to go to Disney if we’d wanted to because all of the reservation slots had been taken. The guests who had planned months in advance and who did go to the hotel reported having a mediocre or bad experience. They paid extra for the Genie+ system that is supposed to enable getting on rides without waiting in line, but using the app was a huge hassle. We heard about some folks paying an out-of-park planner $1800 to manage their Disney app interactions and then text them with instructions for where to go.
Disney obviously has captured 100 percent of the market for people who want to plan their vacations three months in advance, including which rides they’ll do and where they’ll eat, etc. They also have an offering for people who have an extra $850 per hour to spend on a VIP guide. The guide can’t get guests into restaurants, however, as explained in my 2019 review of this experience. In that review, I posted the following idea:
Plainly the mobs are buying a lot of hotel rooms, food, and souvenirs. But I wonder why Disney doesn’t have “Crowd-hater Days” in each park to capture the market of people who would be willing to pay a lot more to have the 1990s experience. There are four core parks within Disney World. Why not say that every Monday through Thursday one of these parks will be designated “Crowd-hater” and tickets will be sold at whatever price it takes to keep max line length down to 15 minutes? If ticket prices were doubled, for example, I think Disney would actually make more money in ticket revenue since demand should not be cut by more than 50 percent. By using a high price to limit admission to only one park at a time they should still be able to keep all of their hotels filled (tourists who don’t value the less-crowded experience will still go to the other core parks and/or the water parks).
Apparently, Disney is never going to do this. So I have a new idea… a pre-planned itinerary that includes reserved meal stops. It will be like Genie+ except that the guest doesn’t have to plan, think, or do anything other than show up at the pre-planned times and pay for whatever is ordered at the meals. The Disney in-house expert figures out in which order all of the rides should be done so as to minimize walking time. I think that this could easily be sold for 2X the price of a regular park ticket plus Genie+ and the cost to Disney and impact on the park should be the same as if someone diligently used Genie+ as designed. Perhaps there is a risk of cannibalizing the VIP guide sales, in which case the price would have to be higher.
How crowded is Walt Disney World now that Americans don’t need to go to work? Disney Springs, which is essentially just an outdoor shopping mall, had 45-90-minute waits for tables at the various restaurants on a Wednesday night in mid-March. Then people would wait in line for another 45 minutes to get a generic ice cream from Ghirardelli. Here are the lines to check out of the Disney trinket shop with $40 T-shirts, to get some BBQ, and to go into a LEGO store that sells the same sets as the LEGO store in your local shopping mall:



The Road to Serfdom is dedicated to “socialists of all parties,” reflecting Hayek’s view that love of central planning is near-universal. Why not a centrally planned no-line Disney vacation?
Full post, including commentsA reader sent the following:
The product can be ordered at jeremysrazors.com.
Based on the photos, it doesn’t look like this is yet another private-label Dorco (the Korean experts behind the marketeers at Dollar Shave Club).
The commercial is fun and the product description includes “It identifies as the best shave kit ever assembled and its preferred pronouns are Buy/Now.” However, I’m not convinced it is worth $60 (8 blades, handle, and some shaving cream in a “socialism-resistant bag”). The comparable Dorco product has a trimmer on the back, a “3D Motion” handle, and is available on Amazon for $23 (then every time you stop at CVS for a COVID-19 vaccine booster pick up some Edge, which is no doubt superior to Jeremy’s cream). Dorco hasn’t taken any position on American politics as far as I know. If you’re in Maskachusetts and need to disguise the fact that you’re not using Gillette anymore, put all of the above in this zippered pouch:
Update: for those who wondered about where razors are made, I did some exhaustive Scientific research (i.e., drove to CVS). I found Gillette products made in China (the latest and greatest “GilletteLabs” razor) and Germany (the core Fusion5 cartridges).
Related:
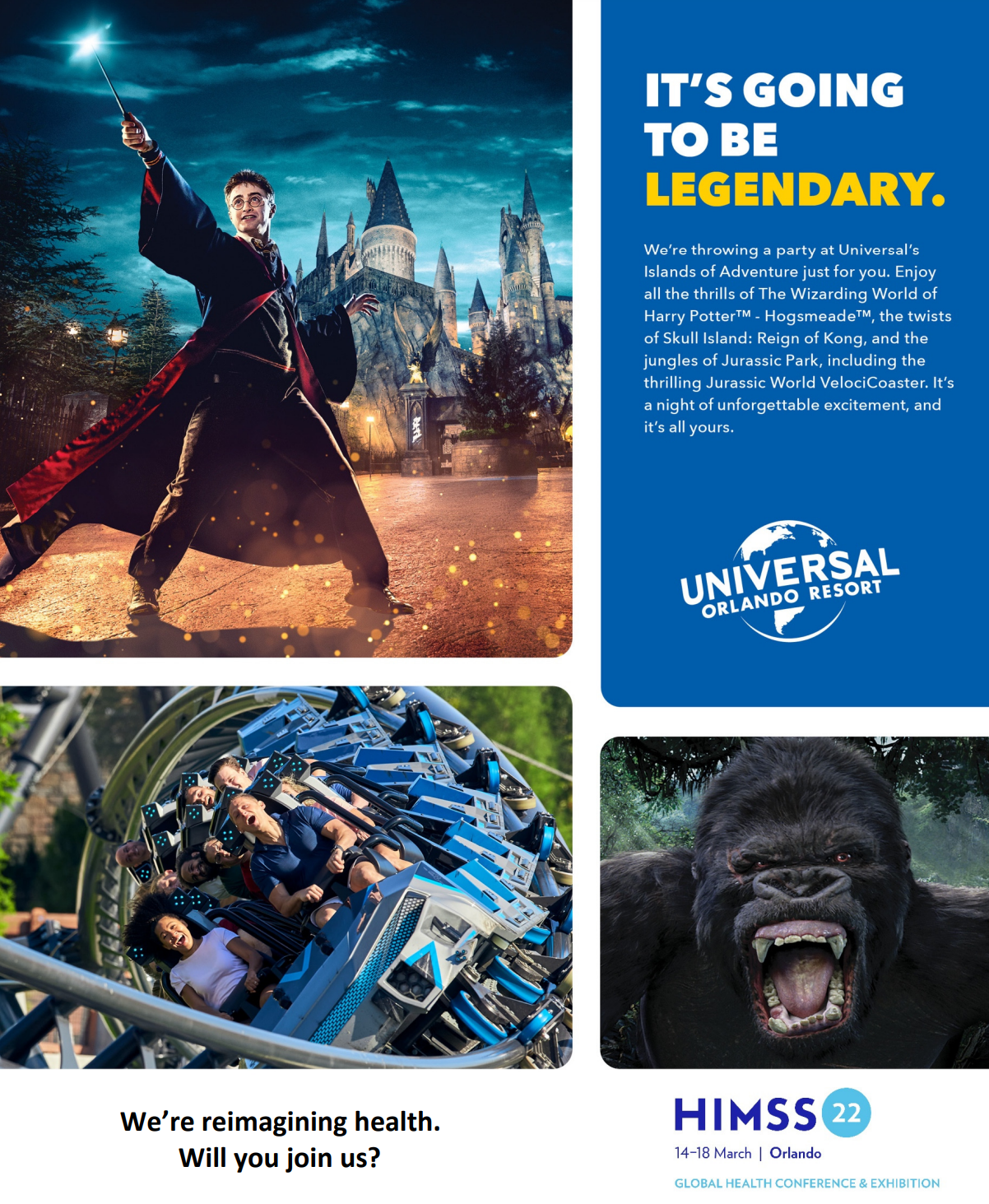
We overlapped in Orlando last week with an electronic medical record expert friend who was attending HIMMS 2022, a conference for 20,000 senior hospital executives and the software companies trying to sell them stuff (the first round of digital stuff was paid for partly with $30 billion of taxpayer funds showered on hospitals by the Obama administration). Attendees had to be vaccinated against a 2.5-year-old version of SARS-CoV-2:

Due to the cruel tyranny of the Florida Legislature, they were forced to add a test option:
Our Right of Entry Policies were specifically designed with consideration of relevant Florida regulations. Our policies allow an attendee to voluntarily show validation of their vaccine status if that is their preference (Option A), or to voluntarily show proof of a negative COVID-19 test within one day of badge pick up, if that is their preference instead (Option B).
How about using a saliva-soaked bandana to cancel out the effects of sharing indoor space for five days with 20,000 other people?
Masks are highly encouraged but not required on the HIMSS22 campus.
What happened in practice? My friend: “I didn’t see a single mask.” (Most of these experts on health care and, therefore, avoiding COVID-19, had brought their families to share the hospital-paid hotel rooms and roam the packed-for-spring-break theme parks during the day.)
How rich have hospitals and their vendors become off the river of tax-subsidized health insurance and tax-funded Medicare/Medicaid? They had sufficient $millions to pay Universal to close Islands of Adventure’s doors to the general public at 5:00 pm, clear the rabble out of the park, and run all of the rides exclusively for the HIMMS attendees starting at 7:30 pm. How was the party? “It was awesome! I got on every ride with no line!”
Related:
Full post, including commentsI haven’t been following the Supreme Court confirmation hearings for Ketanji Brown Jackson (CNN) closely, but it seems that nobody could apply for the job unless he/she/ze/they identified as a “Black woman”. From state-sponsored NPR:
PRESIDENT JOE BIDEN: The person I will nominate will be someone with extraordinary qualifications, character, experience and integrity. And that person will be the first Black woman ever nominated to the United States Supreme Court. It’s long overdue in my view.
A person who switches racial identity from white to Black may be condemned (see Nkechi Amare Diallo, formerly “Rachel Dolezal”), but we celebrate those who change gender identity from “man” to “woman” (see Rachel Levine, for example).
If a Black judge who previously identified as a “man” had, after Dr. Biden’s husband announced his hiring policy, said “I identify as a woman and am proud to be a member of the 2SLGBTQQIA+ community”, would that judge then have become eligible for the Supreme Court position?
William Thomas, for example, who was nominated by President Obama (see “Rubio Withdraws Support for Gay Black Judge’s Nomination to the Federal Bench” (NYT)) and who continues to serve as a judge in a Florida state court. Judge Thomas was already identified by the newspaper of record as “Black” and, under our prevailing theories of gender, only Judge Thomas can pick his/her/zir/their gender ID. What would have stopped Judge Thomas from being considered for the Supreme Court job as a “Black woman”?
Related:
We visited Madame Tussauds Orlando earlier this month and learned that Madonna might not be the best celebrity advocate for years of lockdowns, mask orders, and school closures: “It’s better to live one year as a tiger, than one hundred as a sheep.”
This inspired a search that turned up “Madonna’s Instagram account flagged for spreading misinformation” (BBC, July 2020):
Pop star Madonna has been censured by Instagram after sharing a video about a coronavirus conspiracy theory to her 15 million followers.
In her post, the singer claimed a vaccine for Covid-19 had already been found, but was being hidden to “let the rich get richer”.
Instagram blurred out the video with a caption saying: “False Information”.
It also directed users to a page debunking the claims in the video, noting there is no coronavirus vaccine.
Facebook and Twitter had previously removed the video, flagging it as misinformation; while Donald Trump Jr. was banned from tweeting for 12 hours as a penalty for sharing the clip.
What about the absurd “vaccine for Covid-19 had already been found” claim? From December 2020, “We Had the Vaccine the Whole Time” (New York Magazine):
You may be surprised to learn that of the trio of long-awaited coronavirus vaccines, the most promising, Moderna’s mRNA-1273, which reported a 94.5 percent efficacy rate on November 16, had been designed by January 13.
And the “let the rich get richer” calumny against Science? From October 2021, “The richest Americans became 40% richer during the pandemic” (Guardian):
The 400 richest Americans added $4.5tn to their wealth last year, a 40% rise, even as the pandemic shuttered large parts of the US, according to Forbes magazine’s latest tally of the country’s richest people.
“World’s richest become wealthier during Covid pandemic as inequality grows” (NBC, January 2021):
Almost every country in the world is likely to see an increase in inequality because of the pandemic, according to a new report.
“Wealth of world’s 10 richest men doubled in pandemic, Oxfam says” (BBC, January 2022):
Danny Sriskandarajah, Oxfam GB’s chief executive, said the charity timed the report each year to coincide with Davos to attract the attention of economic, business and political elites.
“This year, what’s happening is off the scale,” he said. “There’s been a new billionaire created almost every day during this pandemic, meanwhile 99% of the world’s population are worse off because of lockdowns, lower international trade, less international tourism, and as a result of that, 160 million more people have been pushed into poverty.”
“Something is deeply flawed with our economic system,” he added.
Separately, on the subject of inequality, Madame Tussauds invites visitors to compare their achievements to some Americans who were selected at random:
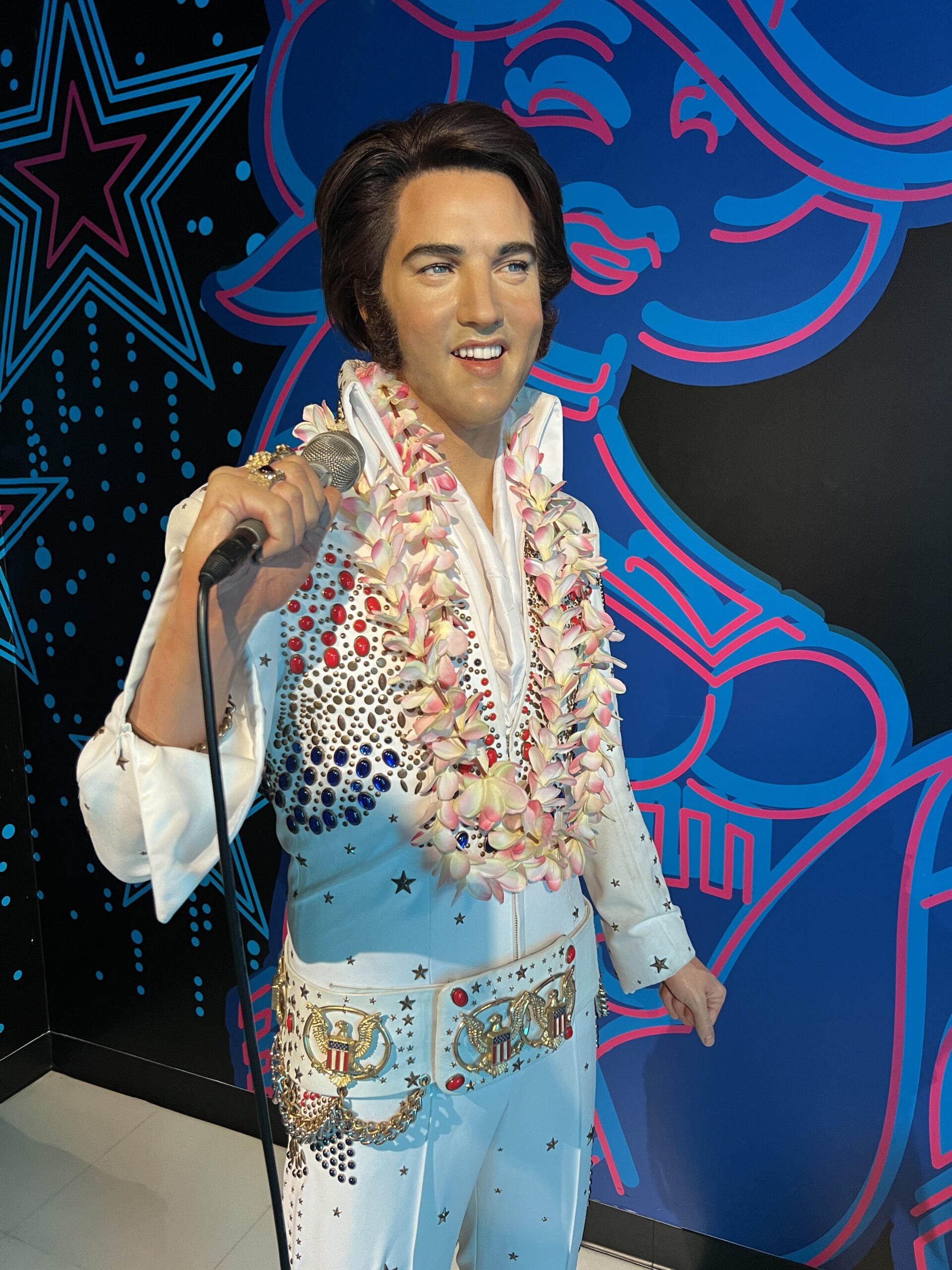

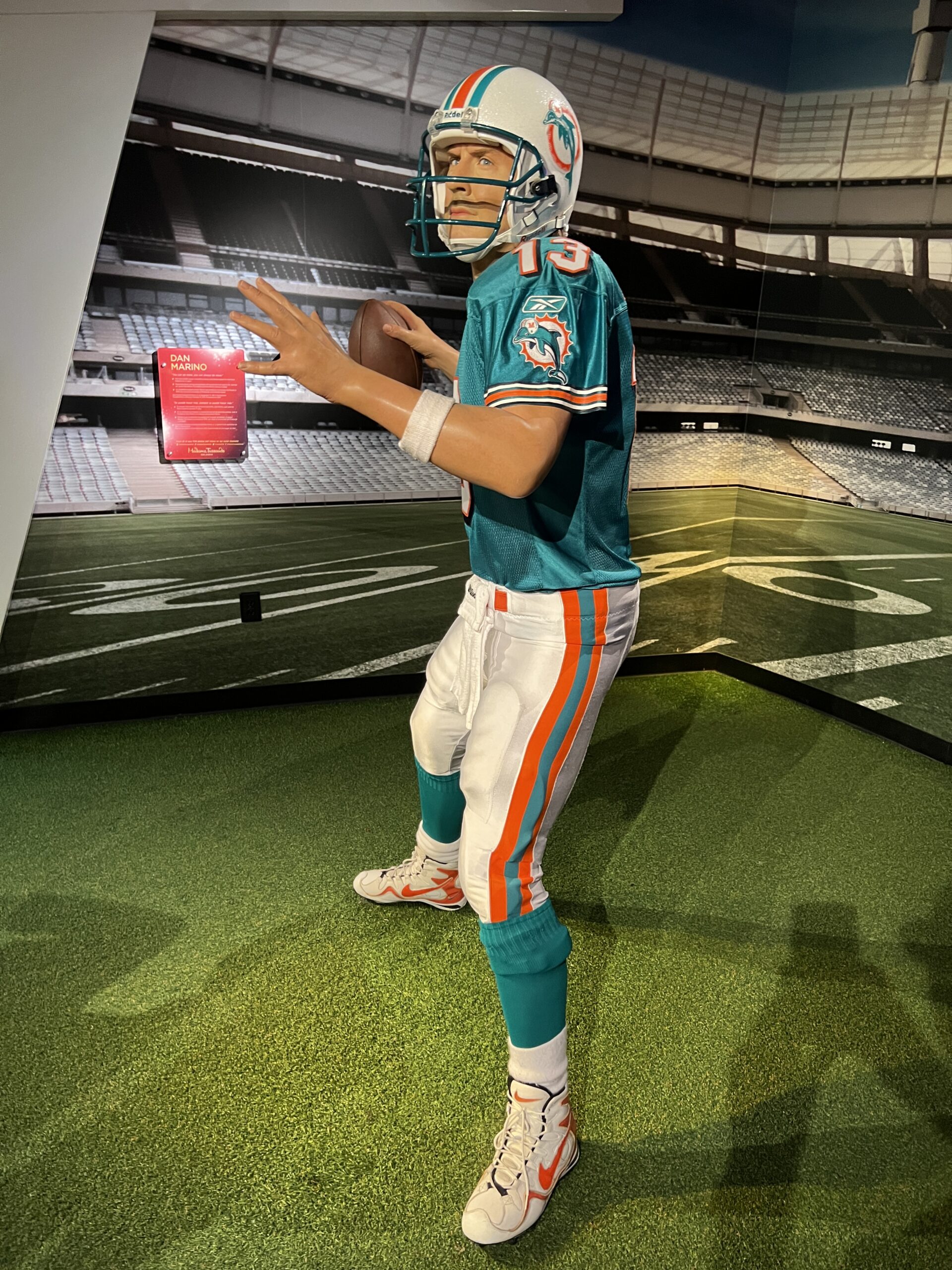
(Elvis, Oprah, and Dan Marino)
Regarding the rich trying to become richer, here’s child support plaintiff Angeline Jolie and the cash source that she has been tapping:


The best part of visiting Madame Tussauds was hearing our 8-year-old ask, after seeing a realistic sculpture of the King of Pop, “Was Michael Jackson a boy or a girl?”
Full post, including commentsFriends have been asking about China Eastern Airlines Flight 5735, the Boeing 737 (non-MAX) that departed Kunming and crashed nose-down near Wuzhou yesterday.
Without the flight data recorder it will be tough to determine what happened, but what I’ve been telling friends is that there are a variety of ways that an airplane can end up in an uncontrollable nose-down attitude.
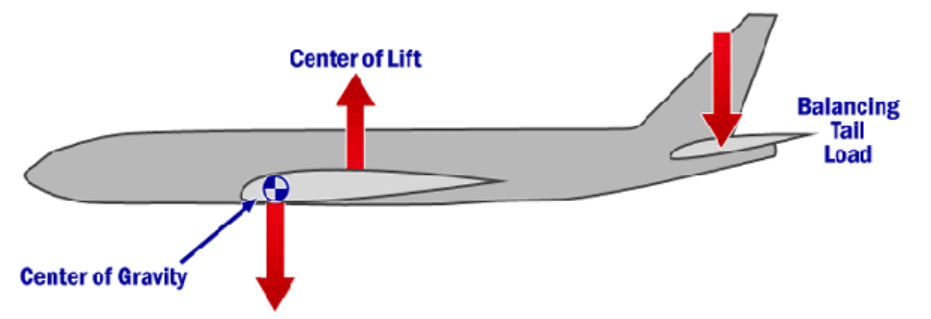
In a conventional airplane, the wings lift up from just behind the center of gravity (CG) and the tail pushes down. If the horizontal stabilizer, which looks like a small wing near the tail, were to break off in flight, for example, thus resulting in a “no tail” situation, the airplane would nose-dive because the wings are lifting from behind the CG. See the following force diagram (source):
There is a substantial amount of overdesign in an aircraft and thus extreme maneuvers may result in a component getting stressed or cracked, but it is almost impossible for the horizontal stabilizer to come off. In the comments section below, a reader highlighted Japan Air Lines Flight 123, a Boeing 747 whose tail, and, more seriously, hydraulic systems, were damaged by the failure of a 7-year-old patch to the pressure vessel.
Is it possible to lose the downforce from the tail without parts of the tail becoming detached? Yes. This can happen due to ice accumulation (see NASA videos below). It seems unlikely that the accident Boeing got into severe icing at 29,000′ (where the steep descent began), however, because the air at that altitude is extremely cold and simply cannot hold much moisture. For the tail to stall while the wings were still lifting powerfully would likely require an unusual failure of the pneumatics, which take hot compressed air from the engines to melt ice off the wing and tail surfaces leading edges.
The horizontal stabilizer’s angle relative to the fuselage can be adjusted via the airplane’s trim mechanism. The runaway-trim-by-design is what brought down the Boeing 737 Max airplanes, but runaway trim can also occur in the non-Max 737, as in other planes. There are a variety of safeguards intended to prevent runaway trim (except in the Max where the computer actually held its finger on the “trim down” button in response to absurd data from a failed sensor), but if those safeguards fail somehow and the airplane is trimmed full nose down it might not be possible to recover.
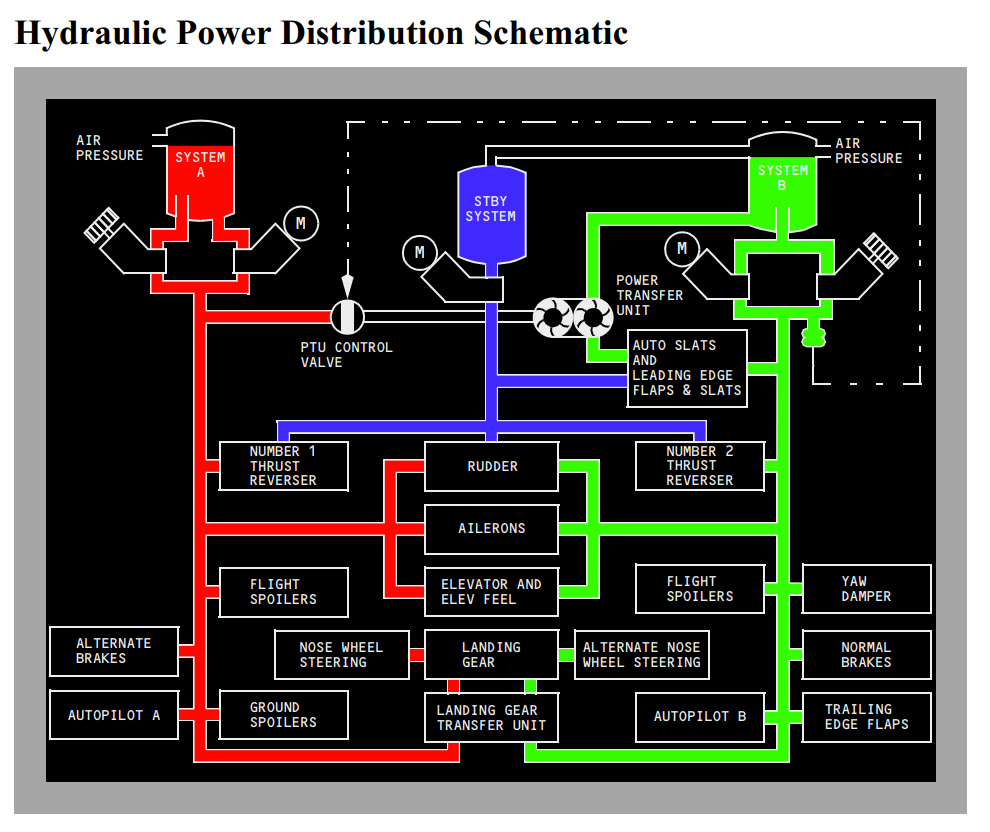
An easy-to-understand cause of a nosedive is movement of the standard flight control surfaces, in particular, the elevator (just behind the horizontal stabilizer). This can be seen at airshows, e.g., in this video of Mike Goulian at Sun ‘n Fun (I’ll be there this year on Saturday and Sunday if you want to meet). Of course, Goulian pulls out of the dive by pulling back on the stick as he gets closer to the ground. If the elevator was stuck in the “stick forward” position does that mean that the pilots of the accident Boeing had the stick full forward? (i.e., the pilot suicide theory) No. Unlike in a lightweight family airplane, the flight control surfaces of a heavy jet are not directly connected to the pilots’ yokes/control columns. No human is strong enough to overcome the air loads of the wind rushing over the control surfaces. What drives the flight controls is 3,000 psi of hydraulic pressure generated by engine-driven and electric pumps (source):
(See also this thorough video explanation.)
How do the pilots of a heavy jet (or “pilot” if one is in the restroom) move a flight control surface then? Ignoring the modern fly-by-wire systems of the Airbuses, the standard technique is a cable that goes from the control column to a power control unit (PCU) next to the aileron, elevator, or rudder. The PCU uses the position of the cable to modulate the application of hydraulic pressure and it is the hydraulic pump that actually moves the surface. (more) Like everything else in aviation, these PCUs are almost perfectly reliable, but if one were to fail/stick it could lead to an impossible-to-control airplane. Here’s an NTSB report regarding an elevator PCU that got stuck in 2009:
On June 14, 2009, a Boeing 737-400, registration number TC-TLA, operated as Tailwind Airlines flight OHY036, experienced an uncommanded pitch-up event at 20 feet above the ground during approach to Diyarbakir Airport (DIY), Turkey. The flight crew performed a go-around maneuver and controlled the airplane’s pitch with significant column force, full nose-down stabilizer trim, and thrust. During the second approach, the flight crew controlled the airplane and landed by inputting very forceful control column inputs to maintain pitch control. Both crewmembers sustained injuries during the go-around maneuver; none of the 159 passengers or cabin crewmembers reported injuries. The airplane was undamaged during the scheduled commercial passenger flight.
An investigation found that the incident was caused by an uncommanded elevator deflection as a result of a left elevator power control unit (PCU) jam due to foreign object debris (FOD). The FOD was a metal roller element (about 0.2 inches long and 0.14 inches in diameter) from an elevator bearing. During its investigation of this incident, the NTSB identified safety issues relating to the protection of the elevator PCU input arm assembly, design of the 737 elevator control system, guidance and training for 737 flight crews on a jammed elevator control system, and upset recovery training.
See also this Wikipedia page on problems with B737 rudder and B747 elevator control due to PCU malfunctions.
So that’s everything that I know, which is to say… almost nothing relevant or helpful, unfortunately, just like everyone else on Planet Earth until and unless the flight data recorder and, perhaps, cockpit voice recorder, are recovered.
More on tailplane icing can be found in these NASA videos…
an older version…
Related:
Full post, including comments