On Friday, June 24th 2021 aircraft engine Manufacturer Lycoming announced a significant mid-year price hike to take effect next month on 24 July, 2021. The company cited “inflation costs associated with components, surcharge increases, and ongoing availability” as the primary drivers for the sudden increase which was made even more unexpected by the timing of the increase well ahead of the company’s usual annual price increases made each December. Communication from Lycoming attached below.
Rotorcorp has conducted a thorough analysis of the new prices on O-320-B2C, O-360-J2A, O-540-F1B5 and IO-540-AEA5 engines utilized in Robinson R22 and R44 helicopter models. It would appear that the July pricing will represent an additional 13% cost to owners and operators requiring Lycoming Factory new, rebuilt “zero time” and overhaul exchange engine options. It also appears that the price increase (roughly 13%) has been added to all small parts and cylinder kits. In real numbers an Lycoming Rebuilt “Zero Time” Exchange O-540-F1B5 Engine will spike by more than $5500 from the current retail price of $48,303 to $53,879.
The rest of the industry won’t be far behind, presumably. So order everything now if you think that you might need it within the next year or two!
(in the 20 years that I’ve been keeping up with aviation, this is the first time that I have seen this occur. Each manufacturer typically has a date on which the next year’s prices are announced. They don’t issue price increases at mid-points)
Department of First World Problems, email from today:
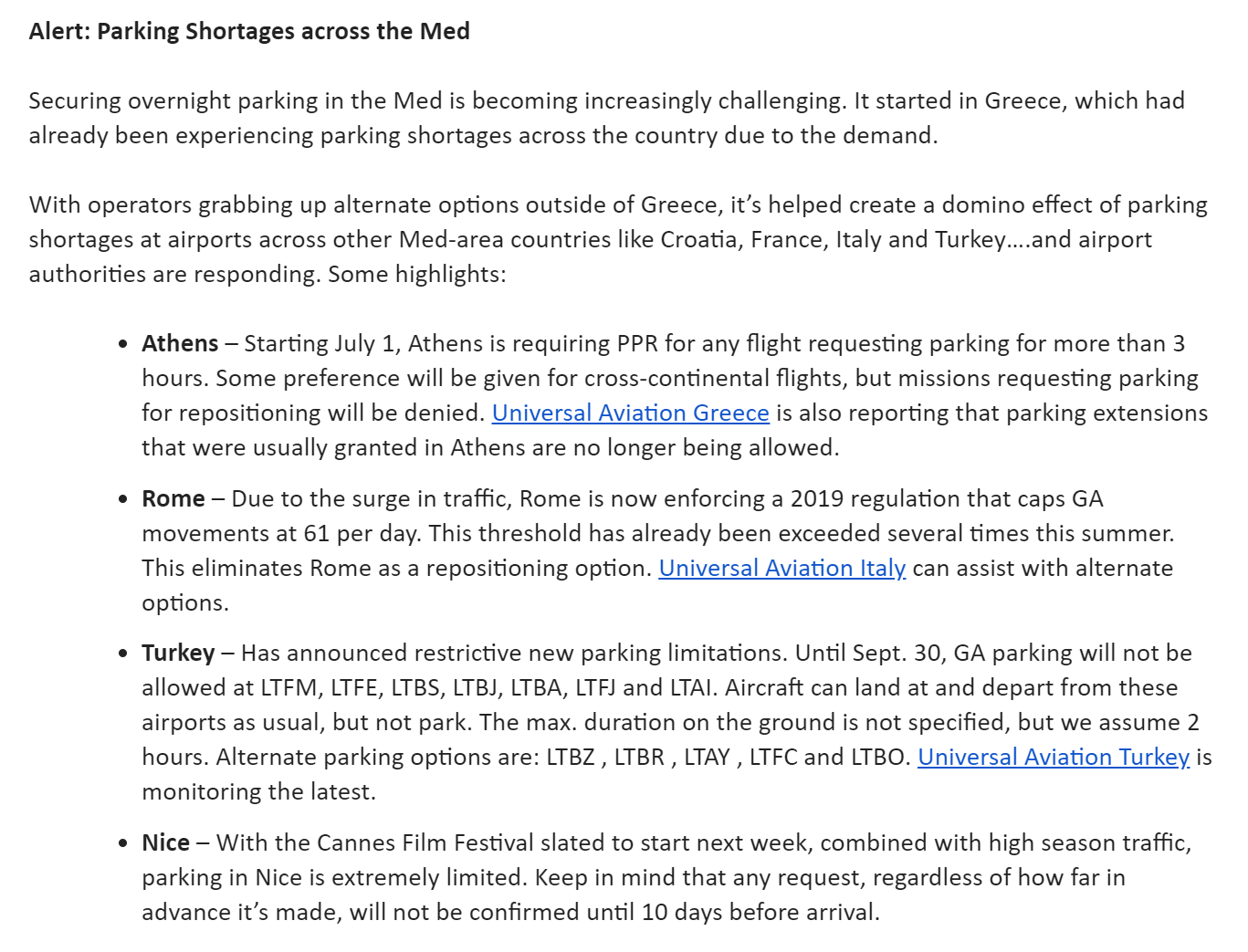
What to do when you get there?
Charter Yacht Market Preps for Record Season – … Some yachts that normally would be heading across the Atlantic are staying back in the Caribbean to maximize booking there. Others are being repositioned to the Eastern Med where countries like Greece and Croatia have less uncertainty right now than France and Spain. And Costa Rica is predicted to be a new hot yacht destination.
The U.S. government is bigger and more heavily funded than ever, but government employees prefer not to work:
U.S. CBP is still on reduced hours at many airports vs pre-pandemic, so don’t assume an airport that used to have 24-hour customs still does.
(I’m going to guess that the hours reduction did not come with a paid staff reduction.)
For the move from Massachusetts to Florida we decided that it would make the most sense to use at least two containers and a dumpster. Container A for the apartment we’re moving into. Container B to a storage facility near the apartment for eventual delivery to a house when we become stupid enough to purchase one. Dumpster for everything else.
We looked at the market leader, PODS, first. They wanted $4,770 per container (16x8x8′) for the move and $265/month per container for rental or storage. The container is wood, steel, and fiberglass and can hold up to 4,200 lbs.
PACK-RAT does not have as large a service area, but they cover West Palm Beach and Boston. The container is the same size, but all steel, like a standard container for a container ship (suitable for jamming into the Suez Canal!). The price for the container/storage is about the same, but they’ll move three containers to Florida (all fit on one truck) for what PODS charges to move two.
A typical cluttered house will require three containers. We’re hoping to trash a lot of stuff, but we also have some aviation gear currently stored in hangars.
In their 79-page opinion, the judges wrote that a “non-prosecution agreement” that had been struck with a previous prosecutor meant that Mr. Cosby should not have been charged in the case, and that he should be discharged. They barred a retrial in the case.
In 2005, Mr. Cosby was investigated in the case of Ms. Constand, and a former district attorney of Montgomery County had given Mr. Cosby his assurance that he would not be charged in the case. The former district attorney, Bruce Castor Jr., has testified that while there was insufficient evidence to bring a criminal prosecution, he had given Mr. Cosby the assurance to encourage him to testify in a subsequent civil case brought by Ms. Constand.
In that testimony, Mr. Cosby acknowledged giving quaaludes to women he was pursuing for sex — evidence that played a key part in his trial after Mr. Castor’s successors reopened the case and charged Mr. Cosby in December 2015. That was just days before the 12-year statute of limitations expired in the case, and it came amid a number of new accusations from women who bought similar accusations of drugging and sexual assault against Mr. Cosby.
“In light of these circumstances, the subsequent decision by successor D. A.s to prosecute Cosby violated Cosby’s due process rights,” the appeals ruling said. “No other conclusion comports with the principles of due process and fundamental fairness to which all aspects of our criminal justice system must adhere.”
Here’s a question for readers… how long will it be before some other state or the Feds charge Bill Cosby with some crime?
California added five more states, including Florida, to the list of places where state-funded travel is banned because of laws that discriminate against members of the LGBTQ community, the state attorney general announced Monday.
Democratic Attorney General Rob Bonta added Florida, Arkansas, Montana, North Dakota and West Virginia to the list that now has 17 states where state employee travel is forbidden except under limited circumstances.
“Make no mistake: We’re in the midst of an unprecedented wave of bigotry and discrimination in this country — and the State of California is not going to support it,” Bonta said.
Lawmakers in 2016 banned non-essential travel to states with laws that discriminate against lesbian, gay, bisexual and transgender people. The 12 other states on the list are: Texas, Alabama, Idaho, Iowa, Oklahoma, South Carolina, South Dakota, Kentucky, North Carolina, Kansas, Mississippi, Tennessee.
Nearly half of the country is now unclean, from a California religious perspective, defiled by failure to fly enough rainbow flags. Why not also ban the untouchables from those 17 states from coming into California? Dig a moat and build a wall to enforce the ban (maybe people who swear a loyalty oath to the rainbow flag and bathe in a ritual bath that cleanses them of hate can be admitted through the checkpoints?).
Speaking of now-banned Florida, here are a few photos of Hate Central (St. Petersburg) from June 25/26 (“Every Day is Pride Day”):
I attended an opera performance in St. Pete and sat next to two middle-aged ladies who had formerly run a B&B in Provincetown, Massachusetts (not exactly the center of straightness). “We’ve been here for two years and love it,” one said. “The government seems to do a better job here. The city is clean, but you never see the cleaners. The roads are very well maintained. Everything is so much cheaper than in Massachusetts.”
Related:
“California lawmakers take trip to Hawaii amid COVID surge, travel advisory” (Sac Bee, November 2020): COVID-19 has squashed most holiday and vacation plans this year amid travel restrictions and quarantine recommendations to slow the spread of the virus. Yet some California lawmakers have traveled to Maui this week for the California Independent Voter Project’s annual policy conference. … The Hawaii trip follows on the heels of backlash over Gov. Gavin Newsom attending a friend and political adviser’s 50th birthday party at a Napa County restaurant called French Laundry, known for its expensive meals.
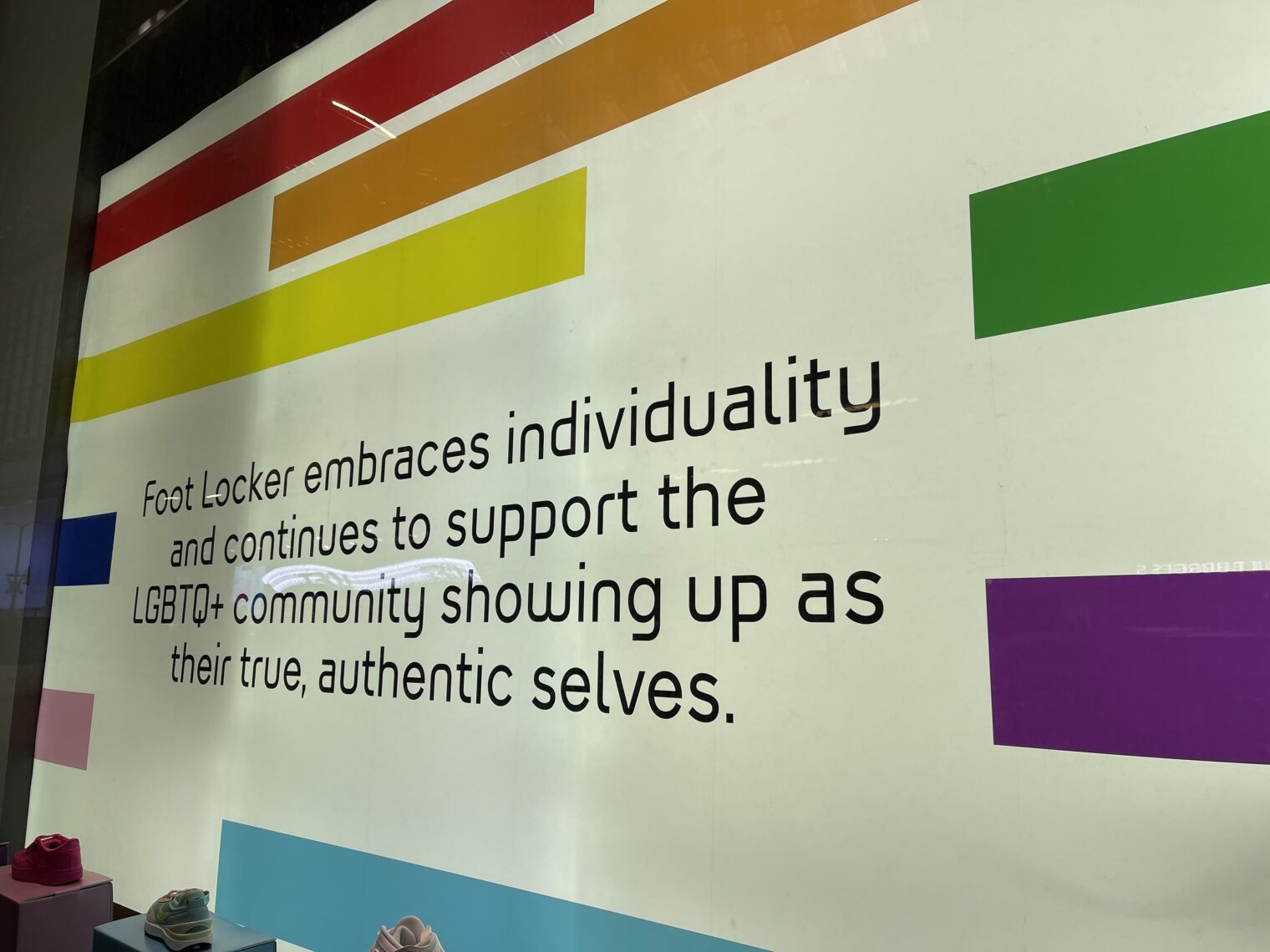
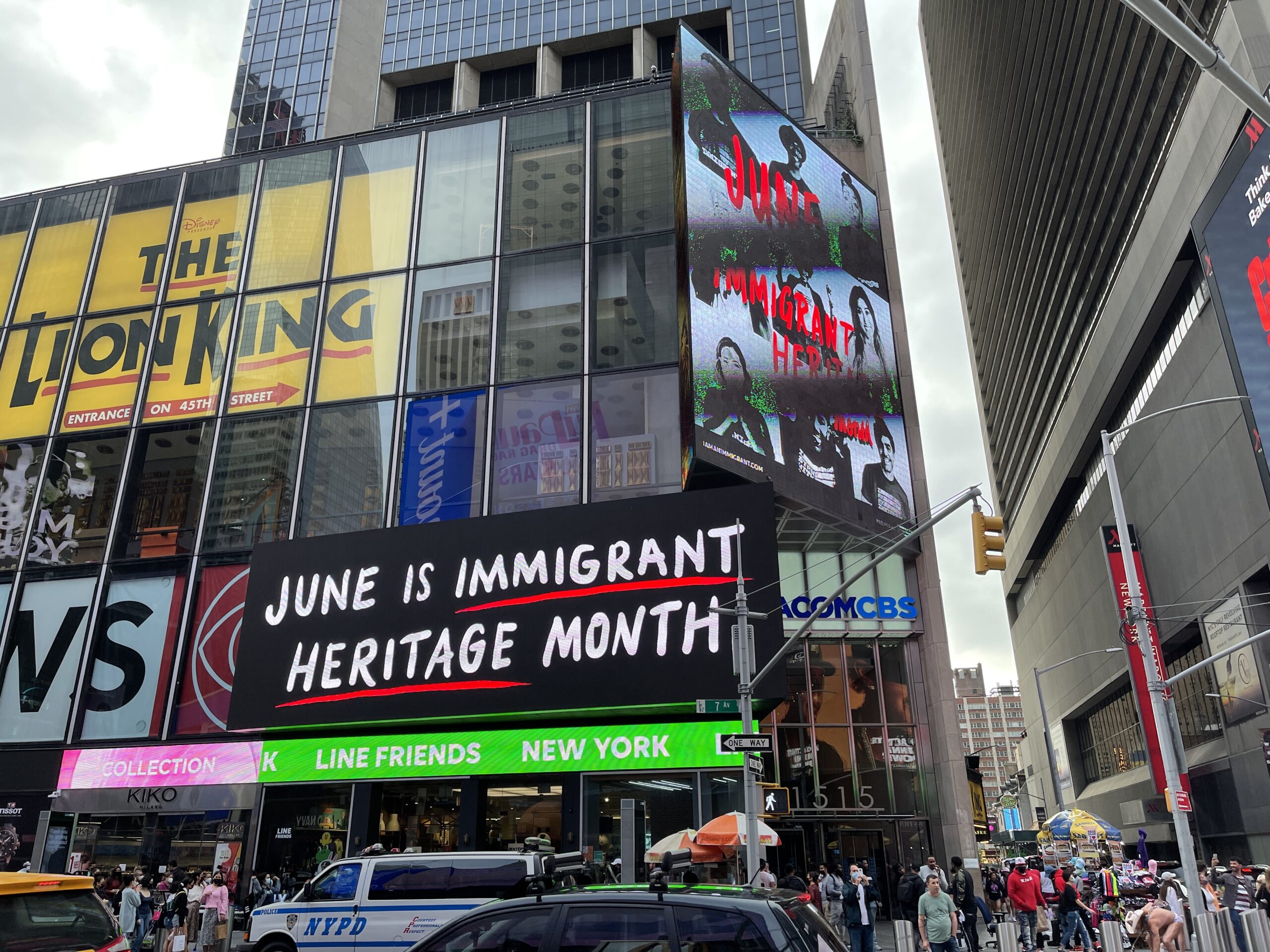
A few images from Manhattan (June 12-13) as we say goodbye to Pride Month. Nordstrom, CVS, Foot Locker, and Pain Quotidien want to remind you of their commitment to LGBTQIA+:
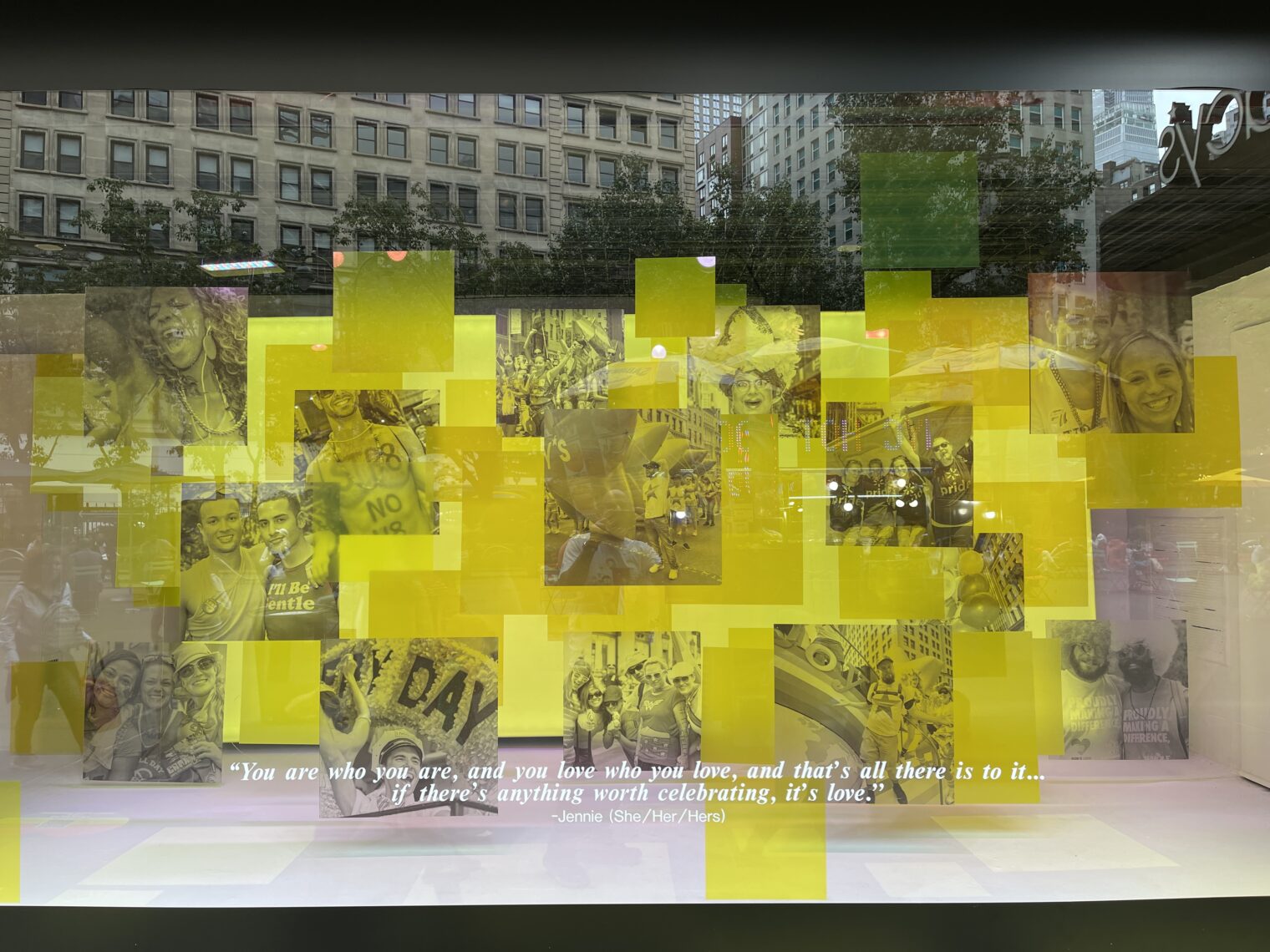
The windows at Macy’s:
“You are who you are, and you love who you love, and that’s all there is to it… if there’s anything worth celebrating, it’s love.” (But what about old people who love to have sex with young people? We don’t always celebrate that, right, unless the people having sex are of the same gender ID? What about Kevin Spacey’s love for William Little (age 18 at the time)? Is that worth celebrating?)
But also remember that June is Immigrant Heritage Month. How many Native Americans celebrated?
According to the Institute of Caribbean Studies, “Caribbean immigrants have been contributing to the well-being of American society since its founding.
And I hope everyone celebrated National Turkey Lover’s Month. If your method of loving turkeys is to kill them and roast them at 350 degrees, celebrate National Candy Month just after. Fully vaccinated and still wearing a double mask while driving solo? That’s a perfect way to spend June, which is National Safety Month. Sleepless in your bunker for fear that coronavirus has slipped inside on a grocery store bag that you forgot to wipe down with bleach? In 2014, the U.S. Senate designated June as PTSD Awareness Month (see the Los Angeles Times, 2014: “As disability awards for PTSD have grown nearly fivefold over the last 13 years, so have concerns that many veterans might be exaggerating or lying to win benefits.”).
This is a report on a June 23 visit to the TWA Hotel, a conversion of the former TWA Flight Center terminal, designed by Eero Saarinen and used from 1962 through 2001. Essentially two big new apartment/hotel blocks were built and the preserved portion is used as the lobby.
If you don’t mind paying $200 to park overnight, the best way to arrive is by single-engine piston airplane. Once the controllers stop laughing, taxi to Sheltair, chat with the helicopter taxi pilots, and the line guys will give you a ride to the hotel.
Try to schedule your visit for a day when the airport is using the 4/22 runways. The pool and the “runway view” rooms overlook 4L/22R, with 4R/22L behind. The action won’t be all that dramatic if the 13 runways are in use, but there is a reasonably good view of 31L. We visited when the 13/31 runways were closed for most of the day (painting?). It irked me slightly that I had to land the Cirrus in a crosswind gusting 20 knots when the airport has a 14,500′ runway oriented straight into the wind, but we were rewarded with a great afternoon and morning of plane-watching.
The hotel celebrates everything that was great/groovy about the 1960s. You won’t learn about the Vietnam War or the Great Society programs that have turned roughly half of Americans into government dependents (not to say “on welfare”!). There is an awesome car collection, including a Lincoln Continental with suicide doors, a Chrysler Newport, a Fiat Jolly, and an Isetta.
You’ll want to buy a reservation in advance to use the rooftop pool on the afternoon of your arrival (it is open to everyone from 7-10:30 am). When it is time for dinner, walk through the lobby to get to the restaurant (great food, stretched-thin service, reasonable (for NYC+airport) prices).
The hotel is tremendously fun for kids, with surprises in a lot of corners. Play Twister, visit Eero Saarinen’s office and drafting table, sit in a 1962 living room, sit at Howard Hughes’s CEO desk.
How about the rooms? Here’s ours before we trashed it (the kids are like 1970s rock stars, but without the musical talent). Perhaps 1/2 to 2/3rds the size of a standard Hampton Inn room. Note the Saarinen Womb Chair ($1000). There is no coffee maker in the room and no room service is available, so consider bringing some cold brew and keeping it in the mini-bar fridge (empty).
Can you run a hotel without bothering to answer the phone? Sort of. As an experiment, I called the hotel prior to arrival and waited on hold until a human answered. 50 minutes. From the room, however, dialing 0 for the front desk, as the rotary phone suggests one do, never resulted in any contact. This proved to be a problem when two dogs nearby embarked (so to speak) on an extended barkfest starting around 9:30 pm (past the sacred bedtime for our boys!). Senior Management was forced to walk down the hallway, go into the elevator, walk through the connector tube, and talk to the front desk in person. She was informed that the hotel didn’t have enough staff to figure out from which room the barking was emanating. Therefore, it became the guest’s job to explore the floors above and below our room. (We determined that the dogs were in the room just above ours, then went back to the front desk to report. The dogs’ owners were reached, but apparently they couldn’t make it back to their room so the situation continued until midnight).
(Other U.S. hotels seem to be on the same plan. I recently stayed at the Hilton in St. Petersburg, Florida and one of the members of our group waited on hold for nearly an hour, calling from the room, to reach the front desk.)
Speaking of noise… the windows are marvels of acoustic engineering and hardly any noise from 22R makes it into the room. Isolation from other rooms and the hallway is not as good, however, as we found out when listening to the canine chorus.
Due to ongoing health concerns regarding COVID-19, as of Friday, March 20,2020 concessions are only offering grab and go and takeout options, consistent with the latest New York and New Jersey directives. Food courts remain open, but we remind passengers to follow social distancing guidelines and to maintain at least 6 feet of separation between other guests. Many retail stores in the airports have closed. Please note that concessions are adjusting their hours of operation and opening status on a daily basis, and so we cannot guarantee any specific concessions or eateries will be open.
A minimum of 16 months to flatten the curve because 15 months plus vaccines plus PCR tests for nearly all passengers plus masks weren’t sufficient?
From the reservation service used by the hotel restaurant:
Per NYC indoor dining guidelines for COVID-19 safety, all guests will be required to have their temperature checked with a reading of 100.00 degrees or less and must provide a contact name, number, and mailing address prior to entering the restaurant as well as wear a mask at all times when not seated at their table.
Even if you want to read about how wise Dr. Fauci is, you can’t do so. The reading room has been closed for 15 months, but that’s “temporarily” and they “look forward to welcoming [us] soon”. Given the postage stamp sized rooms, it is a shame that any of the common space is sealed off.
Gym showers will be disinfected after use, in case surface contamination turns out to be a significant source of COVID-19. You will be protected from the hazard of drinking fountains by using these dangerous devices only to refill water bottles.
The actual gym is huge, perhaps 5X the size of what you’d expect. Nobody inside the gym actually cared about his/her/zir/their health, apparently, because nobody was wearing a mask (consistent with Manhattan customs, roughly half of the folks in the lobby, hallways, elevators, etc. were masked).
Taxiing out… (photo taken by a 7-year-old)
Summary: It’s a fun experience and well worth the $$ (about $500 for the room, pool reservations, dinner, breakfast for two adults and two kids; let’s try not to think about what it cost to run the Cirrus SR20!). We were not even done with the first day before the kids asked when we’d be coming back.
Sad contrast: The JetBlue Terminal 5 that has replaced this magnificent Jet Age building functionally. It is huge without being inspiring, packed with dispirited people being hassled every minute or two with signs and audio announcements regarding masks, and features long lines, e.g., for security. On the plus side, the kids enjoyed riding the AirTrain around all of the terminals!
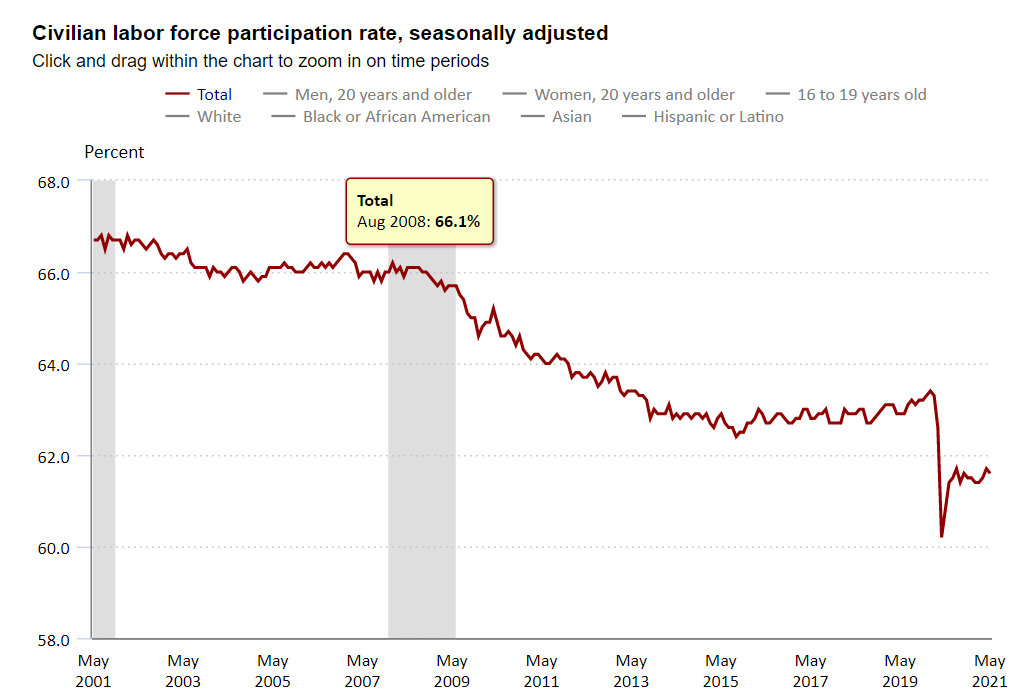
[wife] is pissed at government for extending unemployment. Our nanny won’t work until September because she is being paid to not work.
Many of the Americans collecting unemployment checks (often more spending power than what is obtainable from a median job; see nytimes) are happy to work in exchange for untraceable cash that won’t jeopardize their continued revenue stream from Uncle Joe. They’re examples of Homo economicus from Econ 101, in other words. They put some value on leisure time, but it wasn’t such a high value that it kept them from entering the workforce some years ago. If their value of leisure time hasn’t changed, they should be happy to exchange time for cash money that government computer systems won’t see.
The above-cited nanny, however, did not make the working parents the expected offer to continue her efforts in exchange for cash rather than the previous stream of checks followed by a 1099. Instead, she said that she had “enough” to meet her needs and was not interested in work at all (presumably there was some cash price per hour that would have changed her mind, but she didn’t come up with a quote).
The central planners in Washington, D.C. presumably had some idea of how the enhanced/extended unemployment benefits would change the American workforce, but I wonder if there are way more people sitting on the beach than planned due to an overreliance on the Homo economicus assumption and an underestimate of the number of satisficers like our friends’ nanny. If there are a lot of working-age people who aren’t especially materialistic, it might be easier to shrink the American workforce than economists imagine.
Many young adults are foregoing Covid vaccines for a complex mix of reasons. Health officials are racing to find ways to change their minds.
But the straightforward sales pitch for older people — a vaccine could very possibly save your life — does not always work on healthy 20-somethings who know they are less likely to face the severest outcomes of Covid.
Many young adults are relatively healthy, and they often have work, school and young children to worry about. Getting vaccinated does not always register as a top priority, experts and young adults said.
My comment:
“healthy 20-somethings who know they are less likely to face the severest outcomes of Covid”
shows that the risk of death to an 18-29-year-old is 1/610th the risk faced by an elderly American (85+)
A slender 20-year-old is more likely to be killed in a car accident driving to/from the vaccine clinic than he/she/ze/they would be likely to be killed by COVID-19 if he/she/ze/they did not get vaccinated. If we’re confused regarding why such a person does not want to spend the time and effort to get vaccinated maybe we should question our own intelligence, not the intelligence of the young person.
I guess what is most interesting about this is that the technocrats who are now in charge of the economy and society couldn’t have figured this out 6-12 months ago and come up with a plan, e.g., to pay healthy young people for undergoing a procedure that has no benefit to them. It was already apparent then that COVID-19 was a killer of the elderly (median age of a COVID-19-tagged death here in Maskachusetts: 82). And it was certainly known as of December 2020 that the vaccines wouldn’t be FDA-approved, but only authorized for emergency use. It was entirely predictable that the side effects of the vaccines, e.g., a few days of flu-like symptoms and worse, would be rationally perceived as outweighing the benefits to slender healthy young people.
From Jun 25, St. Petersburg, Florida, part of a crowd of 10,000+ packing into the bars and clubs of Central Avenue just after 11:00 pm:
(I got out my handy bullhorn and told the young people to cease their covidiocy and disperse. I tried to get a chant going where I would say “Stay Home” and they would respond by shouting “Save Lives”, but was unsuccessful.)
Keeping a child from attending public school is a crime. Parents can be arrested and imprisoned for obstructing a child’s access. See, for example, “The Story Behind Kamala Harris’ Truancy Program” (NPR):
In 2019, HuffPost reporter Molly Redden wrote about the families affected by this truancy program, including a Black mother named Cheree Peoples, who was arrested in April of 2013. She came on the show to help explain why this program, which initially launched without much criticism, ended up becoming so controversial, and why it disproportionately affected families of color. Here’s the extended cut of our conversation, which has been edited and condensed for clarity.
Cheree is a mother in California, and her daughter has a chronic illness. Her name is Shayla, and she has sickle cell anemia, a really painful genetic disease that causes lots of complications. It’s pretty typical for people who live with this disability to miss a lot of school if they’re children. As her daughter missed a lot of school for valid medical reasons, Cheree and the school were in a dispute about how to accommodate and account for those absences.
She was in her house one morning, and the police showed up and handcuffed her. She had time to put on a jacket over her pajamas. And when she was walked by the police out of her apartment where she lived with her daughter, there were news cameras waiting, and she was booked by the police. What she said to me was that she was shocked. She was really floored. And she said to me, “You’d swear I’d killed somebody.” It felt to her like a really excessive show of force for what was essentially a misunderstanding between her and her child’s school.
[Harris] fought for this law, which raised the financial penalty and made it a criminal misdemeanor for parents, up to a year in jail, when their children missed at least 10 percent of school time.
Here in Lincoln, Massachusetts, soon to be home to the nation’s most expensive (per student) public school building, the school bureaucrats decided that students could be excluded from the building (i.e., suspended) if they went away for a Saturday overnight in another state, e.g., neighboring New Hampshire or Vermont, and did not have a negative PCR COVID-19 test result to show. As with the former state governor’s order (one of 69), the test had to be taken within 72 hours of returning to Maskachusetts. So, in a twist that only students of the absurd can appreciate, it was legal to be tested for COVID-19 on Thursday evening in MA as a way of determining if someone was going to acquire COVID by traveling on Saturday morning and returning Sunday evening.
Although the school had a fully remote option, a student kicked out of school for quarantine could not transition into the fully remote option for the period of suspension.
The governor’s order was eventually dropped, replaced by an “advisory”. The school, however, continued with their requirement that, essentially, students be tested prior to departure for weekend excursions. They’d been running a “pool testing” program at the school as well, but the pool test could not be used to meet the travel requirement. So a student who was going to go to Vermont for the weekend would end up needing two COVID-19 tests in the week prior (to see if the student acquired COVID-19 in Vermont?).
Not every family can get organized for these tests nor afford them (we spent a month without insurance and we got billed $750 per child for a test at a “doc in a box” urgent care center). Perhaps a test goes awry and a result is never returned. For whatever reason, a child may end up over the border into another state (almost any of which actually have experienced far less COVID-19 than Maskachusetts; Florida, for example, adjusted for population over 65 is at roughly 1/3rd the MA death rate) and later have no test result to show. Why is it legal to deny this child an education for a two-week quarantine period?
#BecausePublicHealth? Maybe that was a good answer when the governor’s travel order was still in place. Now that the technocrats have rescinded their order, however, what is the school’s justification for denying education to children, a criminal offense if parents had done it?