The evolving science of herd immunity from coronaplague
Back in March, the best scientists, including one with a Ph.D. in physics who happens to run Germany (see “60% to 70% of the German population will be infected by the coronavirus, Merkel says”) believed that the majority of a population would have to become infected with coronaplague before herd immunity would would kick in.
“The progress of the COVID-19 epidemic in Sweden: an analysis” does a region-by-region analysis of Sweden, in which plague mitigation efforts among the non-elderly have been minimal, and concludes that when 6 percent test positive for antibodies, herd immunity may be reached among a population that is taking only voluntary precautions:
Notwithstanding that a month ago antibodies were only detected in 6.3% of the Swedish population, the declining death rate since mid-May strongly suggests that the herd immunity threshold had been surpassed in the three largest regions, and in Sweden as a whole, by the end of April. … The herd immunity threshold is likely lower at present than it would be if people were behaving completely normally; it may also be seasonally lower.
Here’s a June 30 article from Quanta, “The Tricky Math of Herd Immunity for COVID-19”:
But on a larger scale, heterogeneity typically lowers the herd immunity threshold. At first the virus infects people who are more susceptible and spreads quickly. But to keep spreading, the virus has to move on to people who are less susceptible. This makes it harder for the virus to spread, so the epidemic grows more slowly than you might have anticipated based on its initial rate of growth.
The above paragraph could have come from a 100-year-old epidemiology text. Thus, it is a example of one of the few bright spots in my coronaplague experience, i.e., seeing how Americans pitch the near-universal failure of “scientists” (except for the MD/PhDs who work for the Swedish government) to predict the likely trajectory and death rate of the epidemic as a success for “science”: Yes, we got everything wrong by a factor of 5-40X, but that just proves how quickly progress can be made in Science with sufficient funding and the right leadership in the White House.
Now that the plague has run its course (for at least Wave #1) here in Maskachusetts, my Facebook feed is packed with people congratulating themselves:
Tremendous achievement in Massachusetts. Not easy. And not free of tremendous costs. But it works and is saving lives ! [over “Mass. Reports 0 New Coronavirus Deaths — and Its Death Toll Drops in Data Cleanup”, regarding a day in which state workers apparently decided to take a mini vacation and not report any deaths]
(A self-proclaimed “data scientist” also posted this as evidence of a grand achievement. The next day, at which point the reported deaths were back to the trend, I ingenuously asked “What happened today? Were there zero deaths again?” He defriended me, thus contributing to my effort to be the most defriended person in the history of Facebook.)
Some data: the July 2 report from MA, population 7 million, with 51 reported deaths. From Texas, population 29 million, 44 reported deaths for the same day:

Florida, population 21 million, suffered 67 deaths on July 2, according to the failing New York Times:
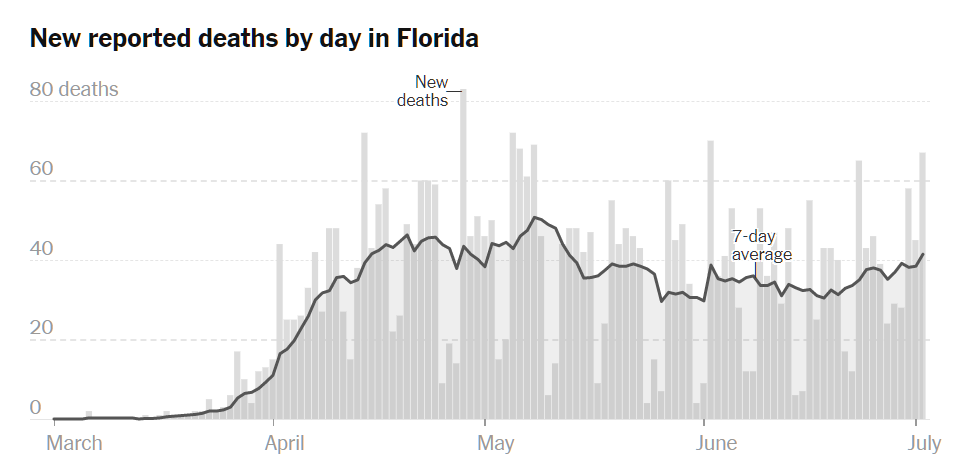
So my friends here in Maskachusetts were celebrating the triumph of humans over a virus despite a death rate vastly higher than the states they explicitly describe as “disasters” and a death rate vastly higher than Belarus, for example, which did not bother to shut down schools, mass gatherings, or anything else. It is a little strange to me, since every year the influenza epidemic winds down and we don’t, every year, celebrate our success in making influenza go away. Example from the CDC of human triumph over the influenza virus:
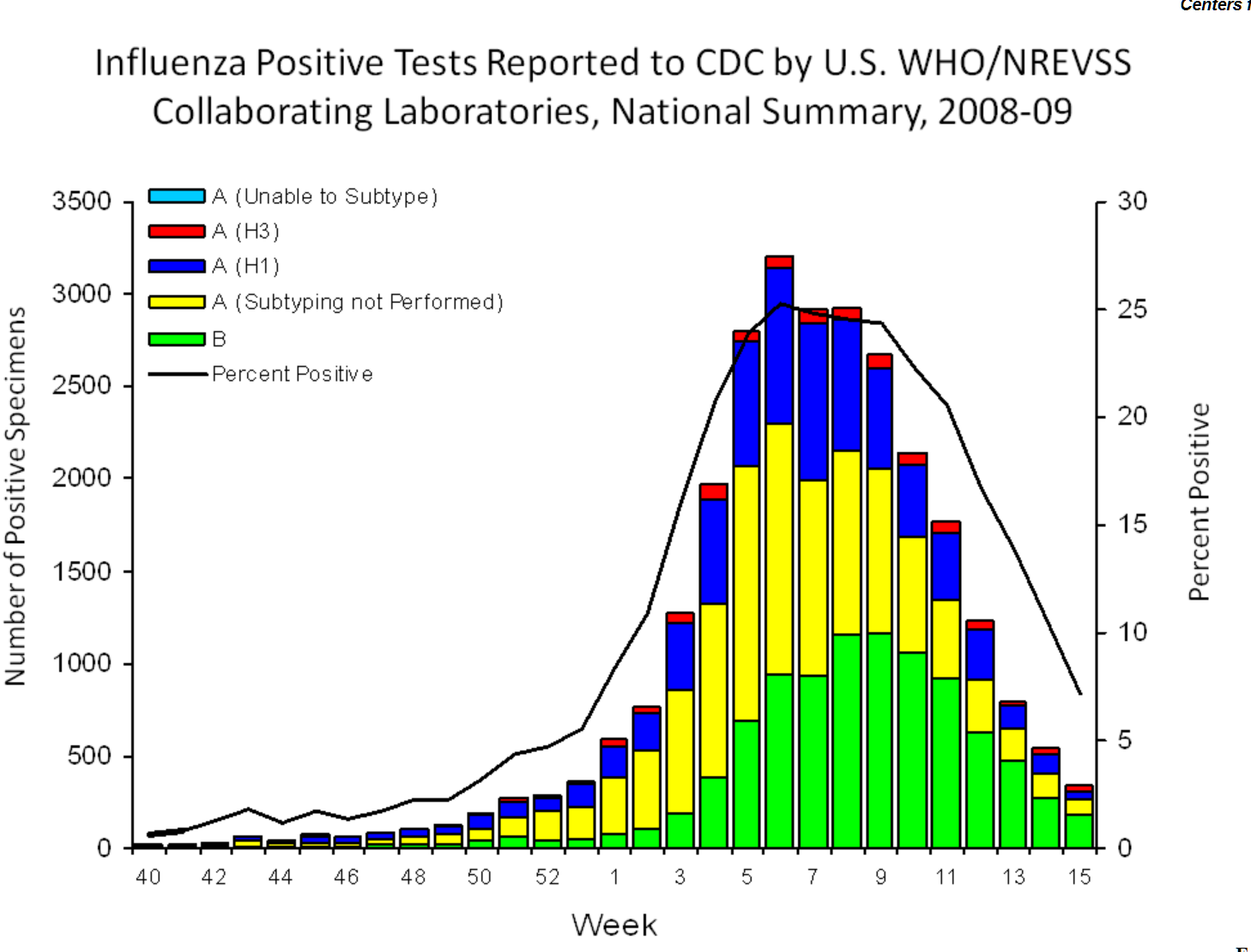
The smart American humans wiped this virus out back in 2009 (thanks to excellent leadership from President Obama?)!
I wonder if the Facebook and media celebration of a zero-death data anomaly in Maskachusetts is a guide to how Americans will process their months (or years?) of shutdown when coronaplague does finally burn itself out. They will simply assert that the sacrifices that they made prevented the virus from killing millions of people, just as the Flagellants believed that they ended the Black Death. And then there will be a twist in which people will assert that things being taught in epidemiology skool back in the 1800s (e.g., Farr’s law) were newly discovered by heroic “scientists” in mid-2020.
Full post, including comments