Who is the fink in Lebanon? And why didn’t Hezbollah leaders leave their bunker after the apartment buildings were cleared?
Hezbollah has been having some difficulties lately in Lebanon, a country that should be a near-ideal host for an anti-Israel organization (almost as good an ideological fit as within Harvard University, Columbia, Dearborn, Michigan, or Minneapolis). Lebanon declared war on Israel in 1948, never accepted a peace treaty (unlike Egypt and Jordan), and never recognized the state of Israel. 80 percent of Lebanese polled were happy about the October 7 attack by Hamas, UNRWA, and Palestinian Islamic Jihad on Israel. In theory, almost everyone in Lebanon hates Israel and Israelis and wants to stay at war with Israel. Yet… someone inside Lebanon has apparently been feeding helpful information to the IDF. Without finks inside Lebanon, how is Israel able to identify Hezbollah-affiliated structures suitable for its precision bombs? Are the informers Lebanese Christians (a shrinking minority, gradually being replaced by Palestinian immigrants)? Lebanese Sunni Muslims who don’t want to be ruled by the Shiites within Hezbollah? Junior Hezbollah members who want all of the senior leadership to be killed so that they can advance within the org chart?
The second big question… Israel recently blew up an underground bunker in which Hassan Nasrallah and colleagues were working. The bunker was underneath six substantial size apartment buildings in a neighborhood where, supposedly, everyone loves and supports Hezbollah. The apartment buildings were destroyed, yet hardly any residents were killed. Supposedly, the building residents were told to evacuate just prior to the 2,000 lb. bombs being dropped. If true, why didn’t the Hezbollah commanders underneath the apartments learn that everyone was fleeing and go somewhere else? (as Hamas has apparently done in Gaza) Did they overestimate the survivability of their bunker?
A related question is what happens to Hezbollah now. The organization has the support of the United Nations. Here’s the Secretary General saying that Israel needs to give Hezbollah time to regroup and rebuild:
Hezbollah also has the support of whoever is running the United States (Kamala Harris and Joe Biden?). Here’s the official whitehouse.gov statement, a couple of days before Mr. Nasrallah met his 72 virgins, in which the Biden-Harris administration officially called for a 21-day ceasefire during which Hezbollah could regroup and rearm:
we call for an immediate 21 day ceasefire across the Lebanon-Israel border to provide space for diplomacy towards the conclusion of a diplomatic settlement
“diplomatic settlement” presumably meant that Hezbollah would remain in power indefinitely. Are there any rival Lebanese groups, e.g., organized by Sunnis or Christians, that are powerful enough to disarm Hezbollah and take over governance of southern Lebanon (where the $500 million/year UNIFIL in theory guarantees that no organization like Hezbollah can thrive)?
Here are the locals mourning a lesser Hezbollah leader early this month (source):

Photos like these, in which the entire neighborhood turns out to support Hezbollah, leads me to the final question of this post… why doesn’t Israel simply destroy all of Dahiyeh, the portion of Beirut from which Hezbollah draws its support? Lebanon is in a declared state of war with Israel so it wouldn’t be a violation of any “international law” to bomb part of Lebanon (just as, apparently, nobody at the UN ever said that it violated any law for the Lebanese to be firing rockets and missiles at Israel for the past year). If the neighborhood that is the core of Hezbollah support were gone, the folks who live there would have to resettle in parts of Lebanon where overt support for Hezbollah might not be as popular.
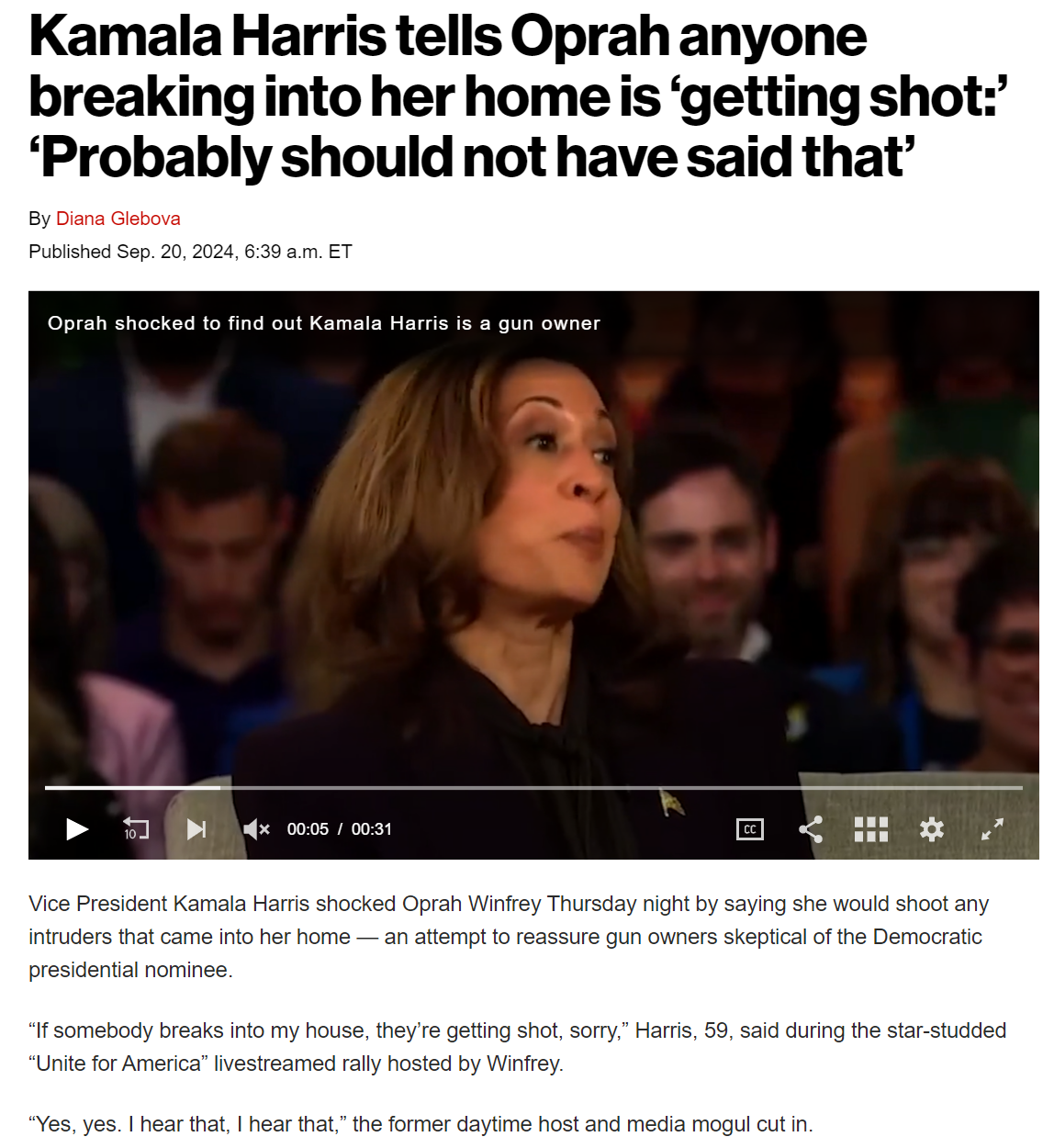
On the intersection between Hezbollah and Kamala Harris: