The centuries-old struggle of humanism versus traditional religion hasn’t resulted in total victory for humanism, even in thoroughly debauched Western societies. Until March 2020, for example, a lot of Americans would shut down their casual sex apps and drive past the billboards for recreational marijuana on Sunday mornings to attend church.
What if humanists could make traditional religious believers afraid of going to church? Or make churches uncomfortable to attend? Enter the public health battalion in the Army of Humanism!
A friend in Newton, Maskachusetts attends an orthodox synagogue. Attendance In October 2021 was about half what it was pre-coronapanic. “The biggest drop off is among the women,” he said, “for whom going to shul is optional.” Christian churches nationwide seem to have experienced a similar drop in attendance.
Now that most of the COVID-vulnerable are either dead or vaccinated (Maskachusetts would be on page 1 of countries ranked by COVID-19 death rate if it were its own country), why wouldn’t the synagogue be full? Mask-wearing is required by the righteous secular #science-following bureaucrats and politicians who run the City of Newton. This makes sitting together for hours unpleasant for no obvious personal health benefit. If the masks do work their 11 percent magic (closer to 0 percent for cloth masks), all of us remain doomed to eventual infection.
The slave states have managed to shut down churches and other houses of worship entirely and/or make attending uncomfortable via mask orders. What about in the free states, such as Florida and South Dakota? In those places, the national and local media, generally run by non-believers, can work to instill fear of COVID-19 that will keep people away from church.
Regardless of whether the fight is happening in a slave state or a free state, is it fair to say that SARS-CoV-2 is the best thing that ever happened to humanism? Religion relies heavily on in-person gathering, which people will refrain from doing, either voluntarily or involuntarily, once convinced that avoiding COVID-19 should be their primary life goal.
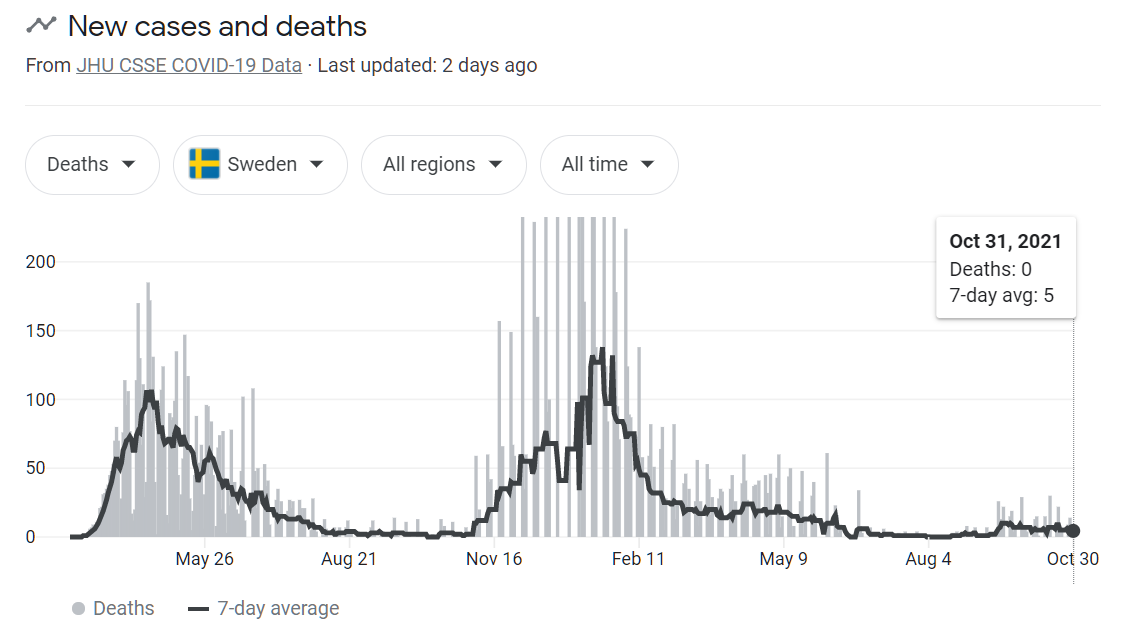
Separately, as long as we’re talking about religion, here’s the curve of deaths, including the summer Delta variant surge, for the infidels following the Church of Sweden:
(Cumulatively, Sweden has suffered about half the COVID-19 death rate compared to Maskachusetts. On the COVID-19 death rate leaderboard, the give-the-finger-to-the-virus country sits right next to Greece, celebrated by technocrats for its victory over the virus: “Greece has responded swiftly and effectively to the Covid-19 pandemic and has so far managed to contain the spread of infections, but the economy has been hit hard, adding to long-standing challenges, according to a new OECD report.” (oecd.org); “The key to Greece’s success, analysts say, was the government’s early steps to contain the virus ahead of most of Europe.” (TIME); “How Greece is beating coronavirus despite a decade of debt” (Guardian))
Full post, including comments