Gerald Ford and the Swine flu panic of 1976
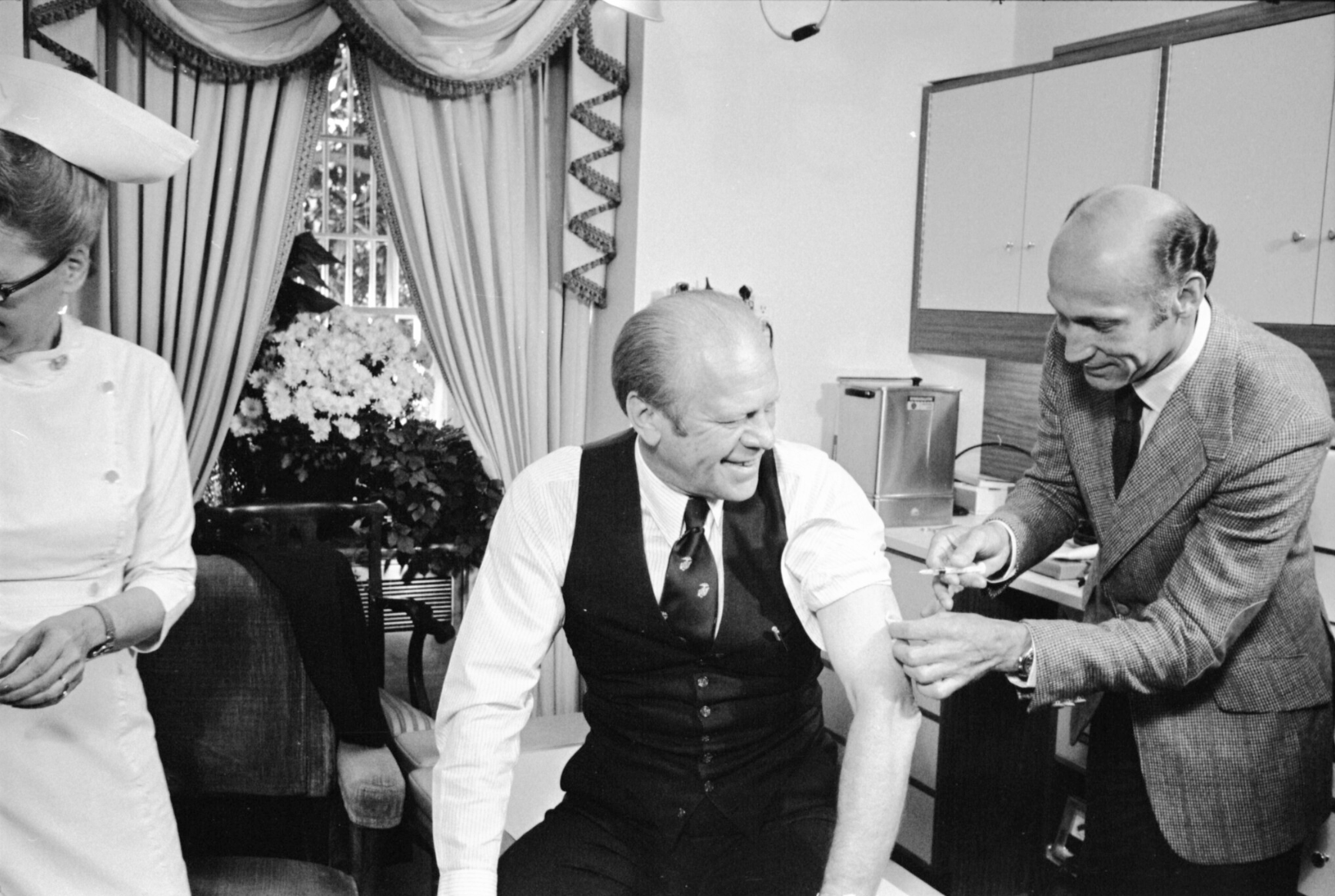
An Ordinary Man: The Surprising Life and Historic Presidency of Gerald R. Ford reminds us of the 1976 panic regarding a respiratory virus: a strain of influenza called “swine flu”. This was the genesis of the modern muscular CDC. Congress appropriated $500 million in pre-Carter/pre-Biden dollars. The CDC said that every American should get vaccinated (Republican Ford publicly accepted the sacrament; Democrat Jimmy Carter refused it). The vaccine was rushed to the market, greatly enriching four pharma companies who also were indemnified from any liability. This indemnification turned out to be useful. The vaccine was at least 10X more likely to cause Guillain-Barré Syndrome (paralysis) than it was to protect the injected person from death due to influenza (contemporary CDC page on the subject).
Abram Saperstein, who changed his name to Albert Sabin, was recruited to sell the idea of universal vaccination. Sabin was famous at the time for having created the oral polio vaccine. After a few months, however, Sabin concluded that the rushed-to-market swine flu vaccine was more likely to harm than help and that a 1918-style epidemic was unlikely.
Speaking of Jimmy Carter, the book notes that his campaign promises were similar to Javier “Chainsaw” Milei’s in Argentina. Candidate Carter promised to reduce the number of federal agencies from 1,900 to 200, for example. What did President Carter deliver? A brand new Cabinet-level Department of Education that kicked off decades of tuition inflation at American colleges and universities via subsidized student loans and grants.
Personal health anecdote: Following the example of Jimmy Carter, the greatest president in our nation’s history, I ignored CVS’s constant reminders of flu vaccine availability. In early January, embedded in Boston with the nation’s smartest and most assiduous mask and vaccine Karens, I got a truly horrible cough/flu. I cursed myself for ignoring CDC advice. After limping home on JetBlue (I actually wore a mask in hopes of protecting fellow passengers!) I went to a German-trained physician here in Palm Beach County and tested negative for both COVID and influenza.
Related:
- “The Effect of Influenza Vaccination for the Elderly on Hospitalization and Mortality” (Anderson, et al. 2020; Annals of Internal Medicine): “Turning 65 [the age at which people in the UK become eligible for flu vaccines from the NHS] was associated with a statistically and clinically significant increase in rate of seasonal influenza vaccination. However, no evidence indicated that vaccination reduced hospitalizations or mortality among elderly persons” (in other words, the flu shot might help some people avoid a brief illness, but it doesn’t reduce the chance of being killed by the flu)
- “Carter’s Flu‐Shot Plan For the Ill and Elderly Termed Short of Goal” (NYT, 1979): [the CDC director] also defended the program against criticism by Dr. Albert B. Sabin, who developed the oral vaccine for polio. Dr. Sabin, who is associated with the Medical University of South Carolina, said that he did not believe that the influenza vaccine would help many people because new virus strains kept cropping up. and required changes in immunization formulas. He said that vaccines containing major new strains became available only after the new strains already had their major impact.