The Brits don’t love the world’s best health care system
From a bookstore in Kensington:
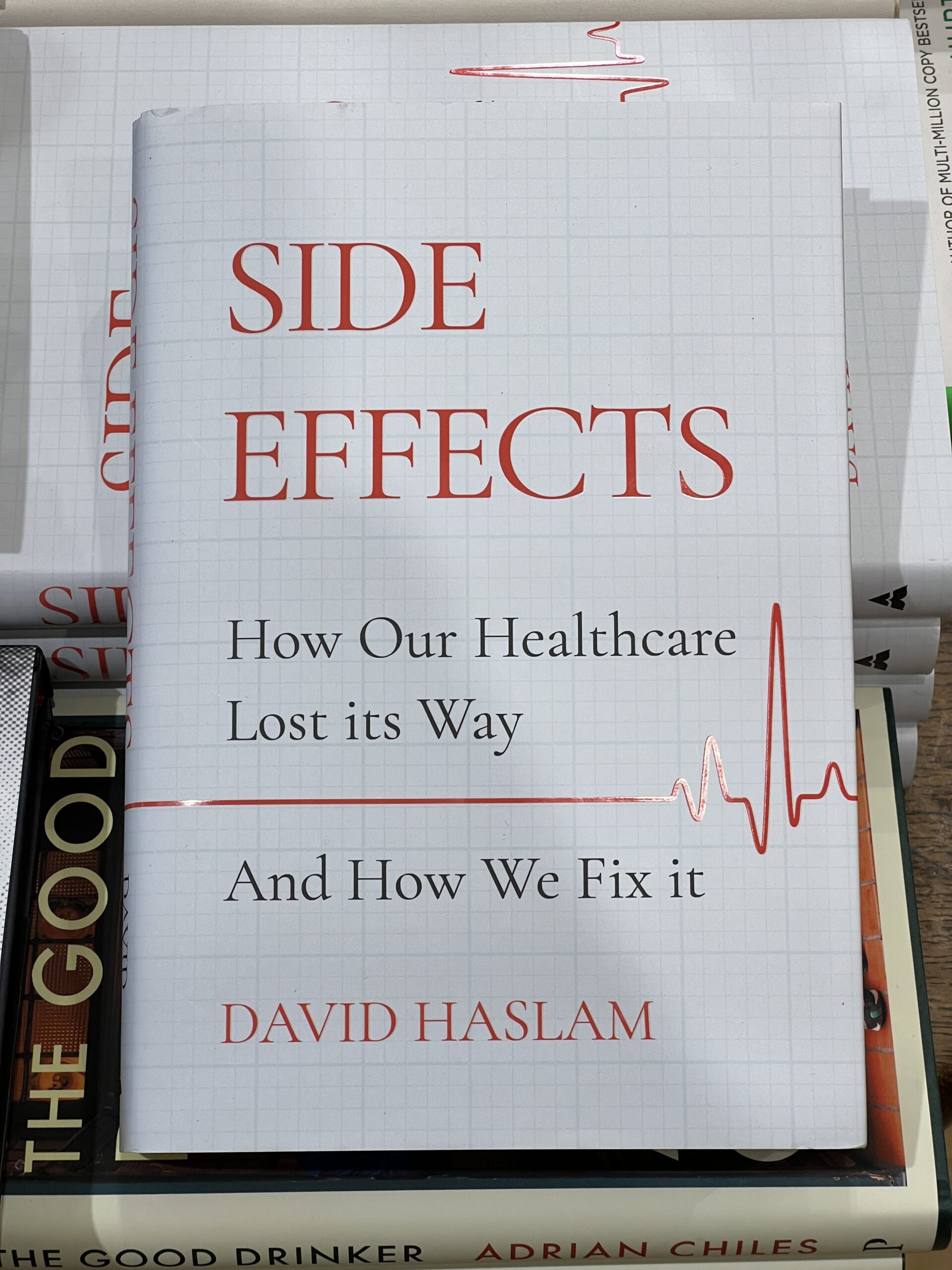
A Guardian review says it is all about the death panels:
Side Effects forces us to face up to – rather than ignore or deny – the realities of balancing the vast sums that can be spent on a single, seriously ill patient against the “distressing conditions in which many frail and elderly people live out their final years, often as a result of lack of adequate funding”. It is all too tempting, Haslam recognises, to dismiss as abhorrent the act of attaching a price tag to a person – as though their worth can be measured in pounds and pence. A human life, surely, is priceless? No amount of mere money or stuff comes close? But anyone who is actually involved in the real, messy world of healthcare knows full well this is nothing but rhetorical posturing.
Later that afternoon I was talking to a guy who is married to an emergency medicine doc in London. With the cost of living adjustment, she can expect to earn 80,000 pounds per year (i.e., $80,000!) after 15 years of slavery for the NHS (age 40). “A train driver will earn more,” he noted, “because their union is actually effective.”
Who is smarter than the Brits for running a universal health care system that doesn’t bankrupt everyone? Africans! “Middle class Nigerians who need any kind of advanced medical treatment will come here on a tourist visa,” my friend explained, and go straight from Heathrow to an NHS hospital. Once they’re in the system they get treated just like anyone else. After consuming what might be hundreds of thousands of pounds in services and recovering, they go back to Nigeria.”
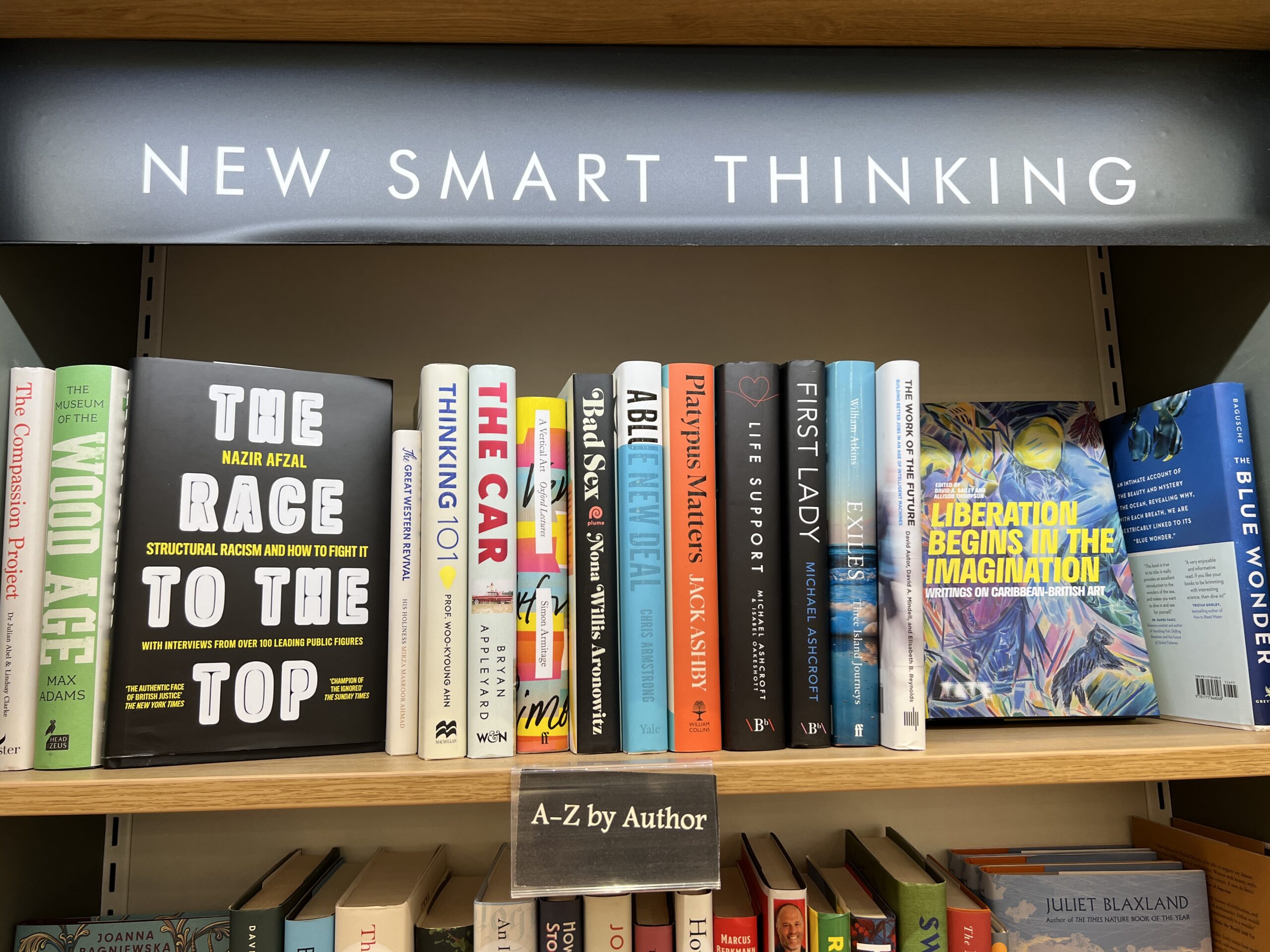
What else did they have in the bookstore? It’s “smart thinking” to fight structural racism:
An American hero who inspires Biden voters can also inspire the British:
Although the age of consent in the UK is 16 (e.g., a 16-year-old could consent to have sex with a rich guy after a Gulfstream flight to somewhere luxurious) and prostitution is a legal career for an 18-year-old, the British are apparently shocked about what Jeffrey Epstein was allegedly up to:
Anyone who isn’t a cisgender heterosexual white male is in trouble:




England was saved from German invasion by women of color who were willing to risk their lives in combat while white men relaxed in the safety of their country homes:
Despite the fact that some heroines exist, the entire Earth is, literally, toast because of those who Deny the Science (i.e., unlike World War II, this is not a war that can be won by women alone):
An entire section of the front of the bookstore was devoted to a personage who by right should have been King of England and was denied this position purely on account of her gender ID:

Circling back to the British health care system… if we aren’t willing to use death panels or at least a quality-adjusted life year calculation the way that the Brits do, how are we going to keep health care from growing to consume 25 percent of American GDP (a shrinking quantity in the aggregate and, since the population continues to grow via immigration, an even more dramatically shrinking quantity on a per-capita basis)?
Full post, including comments