Talking with a pro-Hamas college student
All of my attempts at humor fall flat, as a general rule. In January, for example, I jokingly asked a friend who had visited family in Madrid over Christmas if he’d had to navigate around pro-Hamas protests. He took it as a straight question and gave me a detailed straight answer about the various protests and the parts of the city they’d blocked and what he had done to try to get where he was going.
I needed to talk to a friend’s son regarding an unrelated topic. He’s an avid videogamer and an engineering major at a college in a Rust Belt city whose last period of sustained job growth was during the administration of Gerald Ford. It’s not in Michigan or anywhere else where Islam is the primary religion. He lost years of high school and social life to coronapanic (and, despite diligent masking and meek acceptance of lockdowns, of course got COVID several times). One might imagine that he and his cohorts would have other issues on their minds than the suffering of the noble Gazans… and one would be wrong. I jokingly asked how the pro-Hamas encampments have been at his university. It turned out that he was a regularly attendee at said protests/encampments. “It’s got a really good vibe,” he said, “though only about 50 people actually sleep there every night.”
He took issue with my characterization of the demonstrators as “pro-Hamas”. He said that their goal was to “stop the killing of children.” He agreed that the death of bystanders was inevitable in war and said that he did not think Israel should be allowed to pursue any military activities in Gaza due to the risk that additional children would die. Essentially, the IDF would have to withdraw. I asked “Since Hamas is the elected and popular government of Gaza, doesn’t that mean that Hamas would resume their rule over the territory?” He said “yes” but disagreed that demanding an action that would inevitably ensure continued Hamas rule could be considered a “pro-Hamas” position.
The punchline to the above conversation is that the young man is… Jewish! His mother is Israeli, in fact. She’s an elite wealthy multiple passport European-heritage Netanyahu-hating Israeli, but nowhere near ready to surrender to Hamas as her son is. (Netanyahu’s core support comes from the plurality of Israelis whose ancestors were expelled from majority-Muslim countries, such as Iraq, Iran, Yemen, etc., after 1948. The European-heritage Jews who arrived prior to 1948 are generally much richer if for no other reason than they bought real estate in Tel Aviv before the population grew so dramatically.)
I tried to get him to see that his philosophy, if applied equally to all nations, meant that any army that can surround itself with children becomes invulnerable. Russia could conquer Ukraine, for example, if they just brought some children along to ride in their military vehicles. He more or less admitted that, but stuck to his position that “too many” children had been killed in the recent Gaza battles and, therefore, Israel had to accept defeat and withdraw. (Palestinians themselves do not seem to think that whatever has happened recently is bad enough that they would be willing to abandon any of their military goals. One never hears of Palestinians who say “war is too costly so we will have to compromise for peace and recognize Israel within her current borders.” Instead, they say that they are willing to wage war forever if that’s what it takes to liberate Al-Quds, destroy the Zionist entity, and enjoy a river-to-the-sea Hamas-ruled nation. (cue UNRWA to pay for food, health care, education, etc. until this glorious day arrives))
His siblings also went to public schools in an all-Democrat city and he says that they’re fully aligned with him on the Israel/Gaza issue. My text to his parents: “I would have thought with all of his shooter game experience that he’d believe that sometimes a nation does have to use its military to do military stuff.”
That’s my dive into the wisdom of today’s best-educated youth!
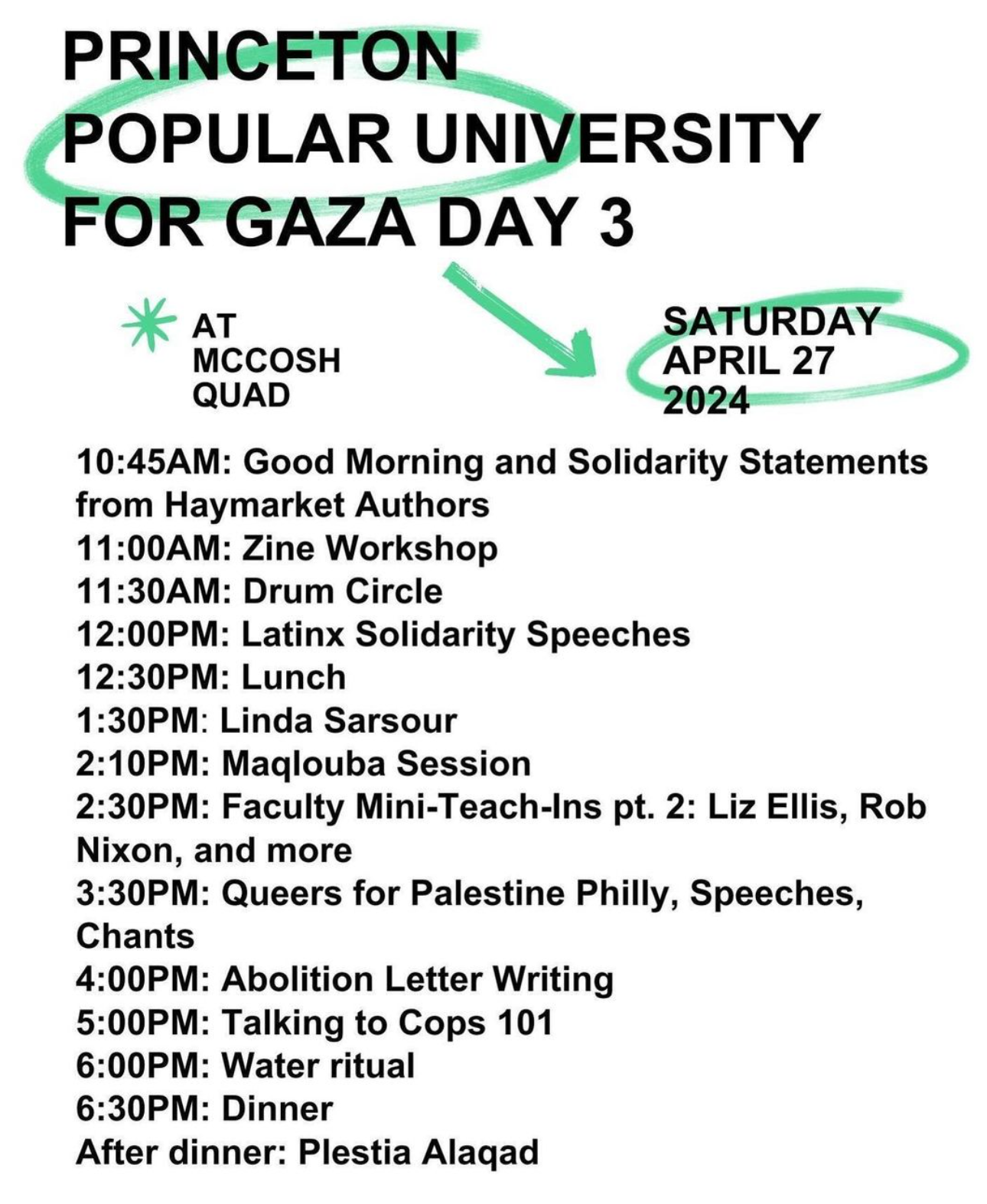
Here’s an example Rust Belt encampment (Syracuse, New York):
Related:
- “The Adults Are Still in Charge at the University of Florida” (WSJ; Ben Sasse, formerly U.S. Senator from Nebraska and current president at UF): Higher education isn’t daycare. … Higher education has for years faced a slow-burning crisis of public trust. Mob rule at some of America’s most prestigious universities in recent weeks has thrown gasoline on the fire. Pro-Hamas agitators have fought police, barricaded themselves in university buildings, shut down classes, forced commencement cancellations, and physically impeded Jewish students from attending lectures. … universities must distinguish between speech and action. Speech is central to education … The heckler gets no veto. The best arguments deserve the best counterarguments. … we draw a hard line at unlawful action. Speech isn’t violence. Silence isn’t violence. Violence is violence. … universities make things worse with halfhearted appeals to abide by existing policies and then immediately negotiating with 20-year-old toddlers. Appeasing mobs emboldens agitators elsewhere. … universities need to recommit themselves to real education. Rather than engage a wide range of ideas with curiosity and intellectual humility, many academic disciplines have capitulated to a dogmatic view of identity politics. Students are taught to divide the world into immutable categories of oppressors and oppressed, and to make sweeping judgements accordingly. With little regard for historical complexity, personal agency or individual dignity, much of what passes for sophisticated thought is quasireligious fanaticism. … Young men and women with little grasp of geography or history—even recent events like the Palestinians’ rejection of President Clinton’s offer of a two-state solution—wade into geopolitics with bumper-sticker slogans they don’t understand.