Karen has COVID-19 (California current case rate surpasses South Dakota’s)
California can legitimately claim to be the Land of Karen. No group of Americans has ever been more active in proclaiming their own superiority on a wide range of political issues. When coronaplague hit, therefore, it was only natural that California Karens dominated Facebook with tales of their superior shutdown and greater vigilance regarding masks. Their heroic and intelligent human action kept the virus from doing what it had done in other states.
When Californians weren’t celebrating their own achievements in prevailing in their self-declared war on coronavirus, they would spend a lot of time gleefully highlighting the high rate of plague in South Dakota, whose governor dared to deny their most cherished belief, i.e., that humans are in charge of the virus and can decide how prevalent infection will be. While the plague raged in South Dakota, the Media of the Church of Shutdown was packed with articles about the stupidity of South Dakotans, Republicans in general, and Kristi Noem in particular.
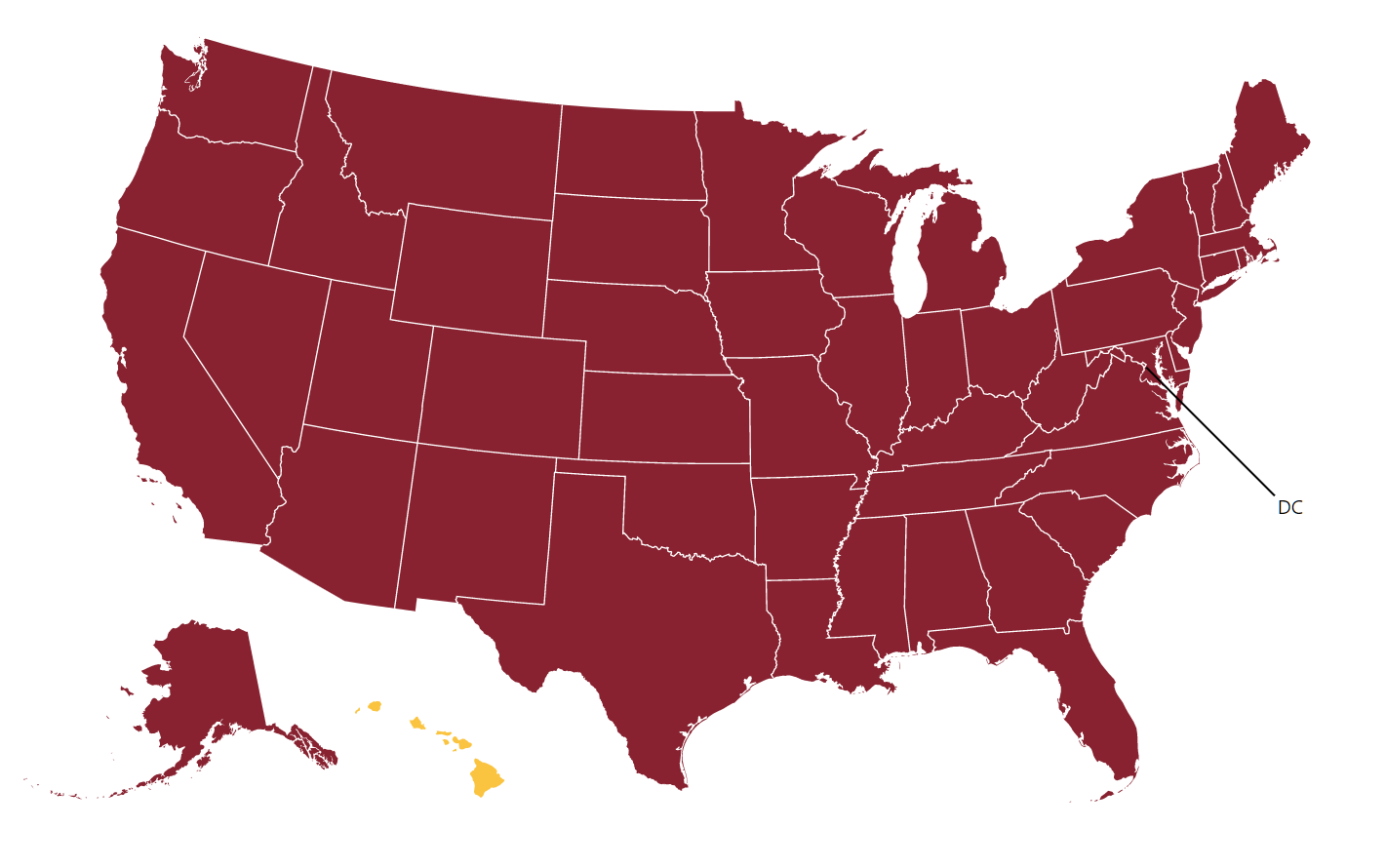
Today’s plague map from the CDC (cases within the preceding week/100,000 population):

The righteous of California were the 4th most plagued Americans, with 101 daily cases per 100,000 (averaged over the preceding 7 days). Wicked mask-denying never-shut South Dakotans? 66/100k. Righteous masked-and-shut folks in Maskachusetts? 68/100,000. Trump voters in Florida? 50 cases per 100,000.
Californians, in other words, are proving the Swedish MD/PhDS right, i.e., continental non-Asian countries can shut down if they want, but they probably won’t be special when the final stats are tabulated.
Who wants to bet on the number of U.S. media articles that will point out that the California current case rate, despite more than half a year of masks, exceeds that of no-mask-order South Dakota or that of no-masks-at-all Sweden?
Related:
- states ranked by COVID-19 death rate (cumulative), showing that California still has a long way to go to catch up to champions New Jersey, New York, and Massachusetts
- Silicon Valley Shutdown Karens move into bigger houses
- speaking of Sweden, they’re still on track to have a similar death rate for 2020 compared to 2010 (slightly more deaths; somewhat larger population in the denominator), thus proving the Swedish MD/PhDs correct when they said most deaths tagged to COVID-19 were among those already likely to die in 2020