One of the things that Western do-gooders scolded India for was its lack of public restrooms, a hazard to public health. What was the first thing that we did in response to coronaplague? Close our public restrooms!
At the Cape Cod National Seashore in May, for example, the beach was open but the restrooms were closed. From the web site:
(They have $110 million for a building for 440 town-resident students, but can’t figure out how to keep an outdoor pool’s restrooms clean/safe? Why are porta-potties better? Because only one person will go in at a time?)
Speaking of the pool… “Face coverings should NOT be worn in the water” and “Patrons should not bring water (or land) toys of any kind with them to the facility, as they increase the risk of contact transmission.” (but didn’t we decide that the “science was settled” and people were not getting coronaplague from surface contamination?)
On the YouTube site, the company says “Doritos is taking meaningful action in the push for real change.”
(How many tens of thousands of pounds have black Americans gained from eating Doritos while locked into their apartments and houses for 4+ months during coronapanic? Maybe the “real change” Frito-Lay is talking about is transitioning from obesity to morbid obesity?)
From the slender friend who sent this to me: “I’ll do a 180 on social justice warriors if they get Doritos cancelled. So gross. Cool ranch Doritos are an abomination.” (she also coined the term “coronapudge”)
Rev. Daniel Moloney, MIT’s Catholic chaplain, resigned June 9, according to a statement by the Archdiocese of Boston. The Archdiocese asked the chaplain to resign after Moloney sent an email to the Tech Catholic Community (TCC) in response to the killing of George Floyd and the subsequent protests.
Moloney wrote in the email that while Floyd should not have been killed by a police officer, Floyd’s killing was not necessarily “an act of racism.” Moloney added that “people have claimed that racism” is a “major problem in police forces. I don’t think we know that.” He wrote that the police officer had “acted wrongly” and that “it is right that he has been arrested and will be prosecuted.”
Moloney also wrote that Floyd “had not lived a virtuous life,” stating that Floyd had committed sins, “but we do not kill such people” and instead “root for sinners to change their lives and convert to the Gospel.”
Suzy Nelson, vice president and dean for student life, wrote in an email to student and faculty leaders June 12 that MIT senior leaders and the Bias Response Team had received reports about Moloney’s email. Nelson wrote that Moloney’s message “contradicted the Institute’s values” and “was deeply disturbing.”
According to Nelson’s email, all MIT chaplains sign the Office of Religious, Spiritual, and Ethical Life’s “Relationship with Affiliated Organizations and Representatives” agreement, which states that chaplains should demonstrate “respect for the dignity and worth of all people and a sensitivity to the beliefs and cultural commitments of others” and that “actions or statements that diminish the value of individuals or groups of people are prohibited.” Nelson wrote that Moloney’s email did not “live up to these expectations.”
We still have the First Amendment, sort of (not the right for healthy young people to assemble, for example). Is it fair to say that, from a functional perspective, we still have the First Amendment right to freedom of religion in the same sense as subjects of the Roman Empire? Conquered people could keep their religion and continue to worship their gods so long as they also respected and worships the Roman gods. Maybe this is why almost every nominally Christian church in Massachusetts has a BLM banner and a rainbow flag.
U.S. travelers won’t be among those allowed to visit the European Union when the bloc begins opening its external borders on July 1. EU ambassadors endorsed a list of 15 travel partners on Tuesday, including South Korea, Japan and, with a caveat, China. Those countries were hit early by the pandemic but have been able to bring the coronavirus under control.
The U.S. was seen as a long shot to make the travel list, which requires that only those countries with epidemiological situations — taking into account both the infection rate and current trends — that are equal to or better than the EU’s can send tourists and other nonessential visitors to the open-border region.
My dumb question for today: If tests work, why can’t airlines test Americans before allowing them to get on the plane to plague-free Europe? If tests don’t work, why do Americans want to pay for millions of tests every day?
Readers: After six months of coronaplague and the genius-level work of Kary Mullis at our disposal, why can’t we credibly promise the Europeans that we won’t send them the Covid-19-ridden?
(from last summer, children playing on a monster trampoline near Copenhagen, no grown-ups within 100 yards)
Feminism is the movement to liberate women from patriarchy. We stand up for the rights of women to control our own bodies as individuals and to control women-only spaces as a class.
Women are adult human females. We do not believe that men can become women by ‘feeling’ like women. We do not condone the erasure of females and female-only spaces, the silencing of critical thinking, the denial of biological reality and of sex-based oppression. We oppose the ‘cotton ceiling’ and the pressure on lesbians to have sex with men. We resist efforts to limit women’s reproductive autonomy. We condemn the men who exploit and abuse women in prostitution and pornography.
“Women do not decide at some point in adulthood that they would like other people to understand them to be women, because being a woman is not an ‘identity.’ Women’s experience does not resemble that of men who adopt the ‘gender identity’ of being female or being women in any respect. The idea of ‘gender identity’ disappears biology and all the experiences that those with female biology have of being reared in a caste system based on sex.” – Sheila Jeffreys, Gender Hurts
Reddit has deleted nearly seven years of content by this community. I asked a friend who considers herself a TERF whether this forum was, in fact, hate-filled. Her answer:
No, the mods were exacting about following the rules. Couldn’t call people trannies, etc. Purely political decision. They still left all the porn subreddits up so it clearly wasn’t about anything other than clamping down on terfs.
The archive.org server grabbed the front page of the forum, but not the actual content. So those of us who were not participants in the community can never know whether they were haters or not. Some of the older threads do seem to be available. Samples:
“gilded” (posts that others liked a lot?), which contains “Transgenderism seems completely innocuous on first glance, but if you look closer at it has many, many grievous harms. Harms that are so large, they are almost difficult to wrap one’s mind around. It basically spells the end of women being able to name and organize around our oppression, which almost certainly spells the end of our having even nominal rights. We will be pushed out of public life and back into the home in many ways.”
Transgenderism does seem to be winning the war, if indeed there was anyone other than a few terfs to fight against. Walking into a Target recently, for example, the very first display for all shoppers is of LGBTQIA+-themed products:
(the gender critical feminists might not be pleased to learn that a trans woman is more “authentic” than a cisgender woman!)
Near the pharmacy, Johnson & Johnson talks about its “championing” of all matters LGBTQIA (but not “plus”!) and offers rainbow-wrapped Listerine, sunscreen, etc.:
Companies usually like to avoid actual political controversy. Why lose nearly half your customers by saying “We at GreedCo prefer Candidate X”? There are some dramatic differences between Joe Biden and Donald Trump, for example, but how many Fortune 500 companies have endorsed either one? The only time that a company would be willing to alienate customers is on an issue where there are hardly any people who strongly oppose the position being taken. From this, therefore, it seems reasonable to infer that, at least since 2011 when Johnson & Johnson decided it was safe to come out of the closet, there is no significant opposition to LGBTQIA advocacy.
I wonder if this sanitizing of the Internet by Reddit, Facebook, Twitter, et al. will actually work against those who advocate for the causes that are now held sacred and to which no opposition can be voiced. Once all of the terfs are silenced, for example, and there is no record that they ever existed because old content is in a memory hole, wouldn’t that cause people to ask an advocate for transgenderism “Who exactly are you fighting against?”
NASA Administrator Jim Bridenstine announced Wednesday the agency’s headquarters building in Washington, D.C., will be named after Mary W. Jackson, the first African American female engineer at NASA.
“Mary W. Jackson was part of a group of very important women who helped NASA succeed in getting American astronauts into space. Mary never accepted the status quo, she helped break barriers and open opportunities for African Americans and women in the field of engineering and technology,” said Bridenstine. “Today, we proudly announce the Mary W. Jackson NASA Headquarters building. It appropriately sits on ‘Hidden Figures Way,’ a reminder that Mary is one of many incredible and talented professionals in NASA’s history who contributed to this agency’s success. Hidden no more, we will continue to recognize the contributions of women, African Americans, and people of all backgrounds who have made NASA’s successful history of exploration possible.”
After two years in the computing pool, Jackson received an offer to work in the 4-foot by 4-foot Supersonic Pressure Tunnel, a 60,000 horsepower wind tunnel capable of blasting models with winds approaching twice the speed of sound. There, she received hands-on experience conducting experiments. Her supervisor eventually suggested she enter a training program that would allow Jackson to earn a promotion from mathematician to engineer. Because the classes were held at then-segregated Hampton High School, Jackson needed special permission to join her white peers in the classroom.
Jackson completed the courses, earned the promotion, and in 1958 became NASA’s first Black female engineer. For nearly two decades during her engineering career, she authored or co-authored research numerous reports, most focused on the behavior of the boundary layer of air around airplanes. In 1979, she joined Langley’s Federal Women’s Program, where she worked hard to address the hiring and promotion of the next generation of female mathematicians, engineers and scientists. Mary retired from Langley in 1985.
As a math undergrad who learned that an SB in mathematics does not make one a “mathematician” and who later studied EECS, I am thrilled to see “a promotion from mathematician to engineer”! I don’t expect to see this again in my lifetime, though.
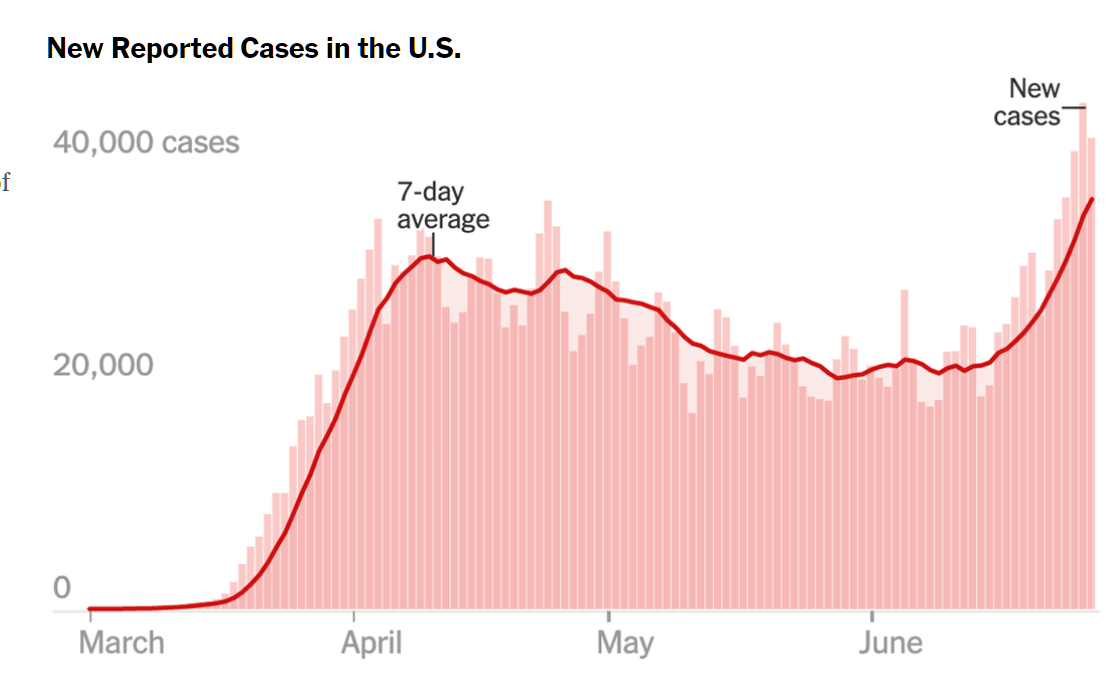
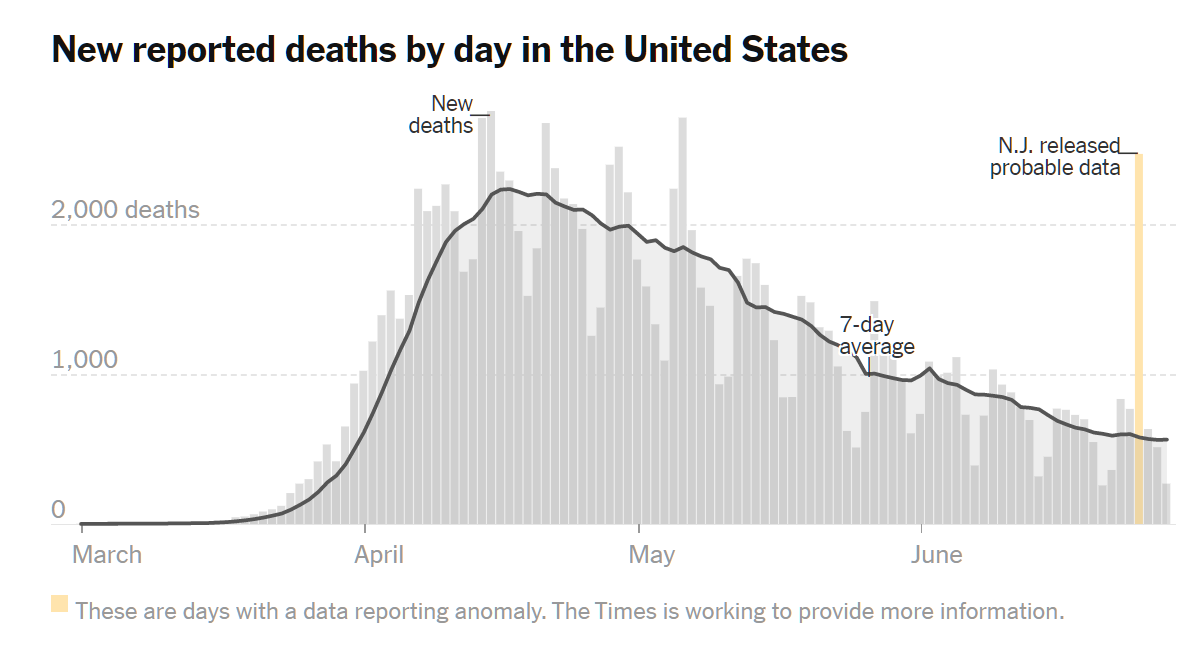
On a recent WhatsApp video call, a friend in Ireland expressed concern over the disastrous wave of deaths washing over the United States. He’d scanned newspaper headlines and had processed that coronaplague infections were at an all-time high in the U.S. He inferred from this that Americans must be dying in larger numbers than back in April, for example.
I checked the front page of the New York Times while we were chatting. Sure enough, plague is worse than ever here:
Unlike my righteous neighbors in Maskachusetts, he does not pretend to care about all humanity. So he hadn’t clicked down and scrolled through five screens to get to the following chart:
I.e., if this chart were on the front page, we might think that the plague was on its way out! (and we would, I hope, attribute this to our faith in the Church of Shutdown and the Sacrament of Masks!)
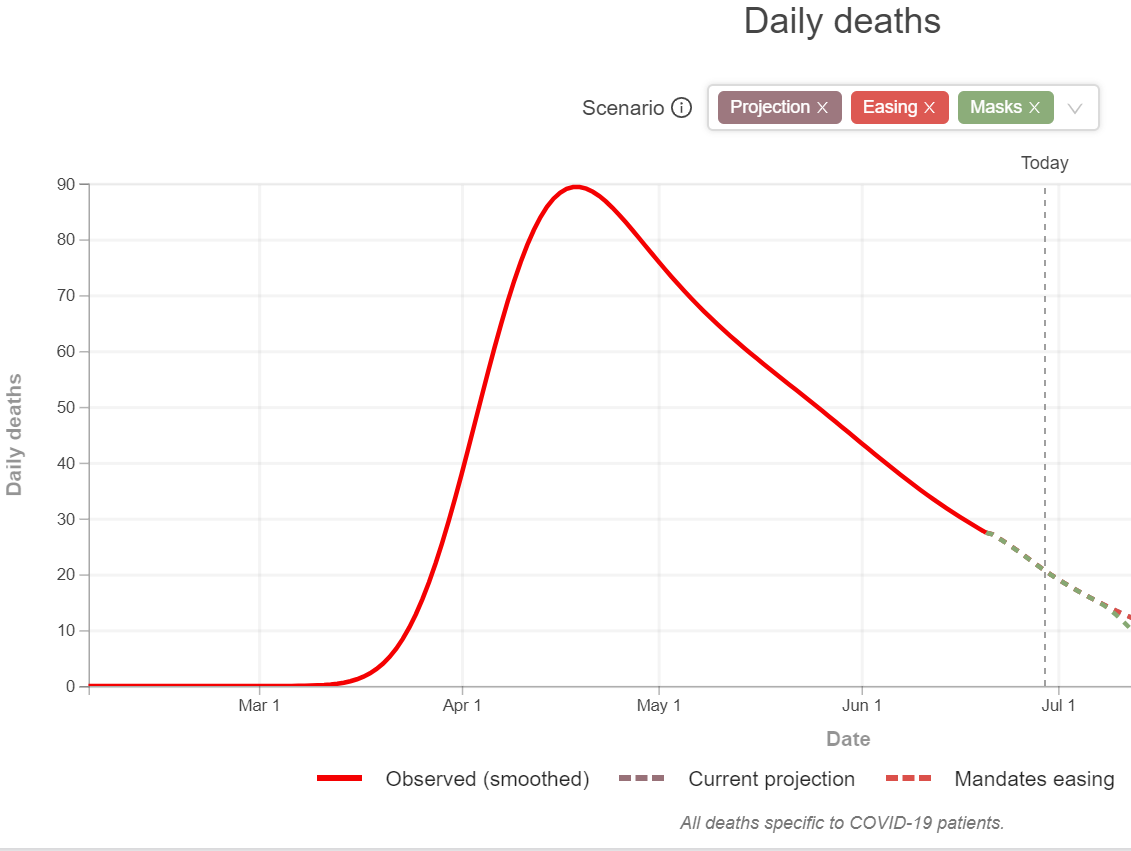
[For reference, a similar curve for never-shut never-masked Sweden (from the prophets at IHME):
]
It was interesting to learn what kind of impression our media leaves in a reader’s mind when the reader is not carefully focused on drilling down into the details.
Separately, in today’s coronasteria, the front page of the New York Times screams “Global Coronavirus Death Toll Surpasses Half a Million”. Drilling down into the story, the reader will find no comparisons to what other causes of death might afflict the world’s 7.8 billion humans (none of whom are “illegal”!). He/she/ze/they will not learn that, for example, “Up to 650 000 people die of respiratory diseases linked to seasonal flu each year” (WHO).
Related:
Politifact rates Donald Trump’s tweet “As of June 23, the COVID-19 death rate is ‘way down.'” “mostly true” (i.e., it is “partly false” to say that a downward trend is “down”)
One interesting tidbit: When Genghis Khan wanted to take over a big fortified city, he would attack surrounding small villages and drive the inhabitants as migrants and refugees to the big city. Swelled with a larger-than-usual population, the big fortified city would collapse from within, its resources (such as food) exhausted. This saved Temüjin, the Great Khan, the effort of a traditional Greek/Roman-style siege and catapult attack on a walled city.
Do you send out one email every Monday morning and then host a couple of group video chats later in the week? You’re a hero!
Educators will continue their heroic efforts from this spring and will work hard to make our schools ready for our students this fall. Educators, through their unions and in collaboration with students and families, must play a central decision-making role in the return-to-school plan, district by district. Ultimately, we will decide if these directives have been met by the state and the districts.
Everywhere that the schools previously had a rainbow there will now be a double rainbow:
We cannot go back to the status quo, which was actively harming many of our youth, families, and educators of color, as well as people from other marginalized groups, including our LGBTQ+ students. We must instead be bold and create free and equitable schools where education liberates and empowers our youth so a brighter future is possible for all of us.
[among the “Key Directives”] Curriculum must reflect and affirm our LGBTQ+ students.
This is a bit odd when you think about it. LGBTQIA+ students weren’t being reflected and affirmed previously. I am sure that we will all agree that this was a terrible situation. But who created that situation if not the very unionized teachers who now say that the situation must end? What was stopping them from reflecting and affirming LGBTQIA+ students six hours per day every day?
There is one Key Directive that is worth putting in bold:
Eliminate MCAS and reevaluate the ways our public schools are assessed.
In other words, the only objective test of student learning has to be tossed out. (Admittedly, the raw MCAS does not measure school performance that well since the children of well-educated parents tend to score highly even if their teachers don’t teach anything.)
Teachers should be hired and promoted based on skin color:
We must prioritize hiring, retaining and promoting educators of color.
But will the older white teachers resign or subject themselves to firing in the event of poor performance in order to make room for educators of color?
Here’s a principle that I can support wholeheartedly:
Every student — and every educator — deserves access to the basic tools of a modern society: a computer and reliable internet access.
Would someone please tell this to Comcast?
As soon as the first person anywhere in the state gets a fever in November and a positive coronavirus test, the teachers will go back home to their pets and gardens:
Educators must be supported with … effective practices for crisis learning remotely.
Districts must provide support … if we are again forced to return to crisis learning remotely.
One fact that I learned about a private school was that they have already wired up every classroom with video cameras so that students who need to stay home for any reason can participate remotely and see what is going on in the physical class.
The MTA is a union of 116,000 educators … We are entering a dangerous and unknown peak period of this pandemic. … We present these demands of local and state officials …
Keep schools closed statewide for as long as necessary to ensure the health of students, faculty, and staff. No educator should be required to come to work when schools are closed for students. Any vulnerable staff should be able to stay home with no loss of pay or benefits.
All educators – full-time, part-time, hourly and per-diem workers, including teachers, secretaries, paraprofessionals, cafeteria workers, bus drivers, and substitute teachers – must be fully paid during this time,
Guarantee that pay and pensions are not affected by the pandemic.
Declare a moratorium on all educator evaluations
Based on the above, I don’t think my friend is going to get that property tax refund he had been expecting based on the fact that his middle schoolers did not receive any education after mid March.
[Our own town of Lincoln, Massachusetts will presumably be one of the last to reopen its schools due to the fact that the square footage is going to be dramatically reduced via a $110 million construction project that moves children into cramped trailers with minimal windows and doors from 2020 through 2023:
They couldn’t find a place to build a new building on the 70-acre campus (above) while continuing to use the old building.]
State reopening guidance (June 25): “Schools do not appear to have played a major role in COVID-19 transmission. … Students in grade 2 and above are required to wear a mask/face covering that covers their nose and mouth. Students in kindergarten and grade 1 should be encouraged to wear a mask/face covering. … Mask breaks should occur throughout the day. Breaks should occur when students can be six feet apart and ideally outside or at least with the windows open. … aim for desks to be spaced six feet apart (but no fewer than three feet apart)” (in other words, elementary school children do not spread coronaplague, but let’s make them wear masks anyway)
“Research Shows Students Falling Months Behind During Virus Disruptions” (nytimes, June 5): The average student could begin the next school year having lost as much as a third of the expected progress from the previous year in reading and half of the expected progress in math… A separate analysis of 800,000 students from researchers at Brown and Harvard looked at how Zearn, an online math program, was used both before and after schools closed in March. It found that through late April, student progress in math decreased by about half in classrooms located in low-income ZIP codes, by a third in classrooms in middle-income ZIP codes and not at all in classrooms in high-income ZIP codes. When all of the impacts are taken into account, the average student could fall seven months behind academically, while black and Hispanic students could experience even greater learning losses, equivalent to 10 months for black children and nine months for Latinos, according to an analysis from McKinsey & Company, the consulting group. … The disparities in educational progress do not appear to be caused by any lack of effort on the part of families. The poorest parents spent about the same amount of time during school closures assisting their children with learning — 13 hours per week — as those making over $200,000 per year, according to a May Census Bureau survey of households with children.
A couple of mathematically sophisticated friends were debating Sweden’s policy with respect to Covid-19. One argued from the assumption that the death rate in Sweden was higher than in some nearby European countries (also true for Massachusetts and nearby states such as Vermont (photo below), New Hampshire, and Maine, despite similar policies).
Me:
How do you know how many people died in these respective countries? What if the shutdown in Finland and Norway, for example, made people depressed, fatter, out of shape (gyms closed), etc. and they’ll be more likely to die in the next few years from these ailments? A huge number of people in the U.S. will die from the shutdown of regular health care. Because we are obsessively focused on a single number (Covid-19 death rate) as a measure of the success of a society, we will probably never bother to add these up. (see NEJM)
You aren’t asking how many lives are lost when children can’t go to school and don’t get the education to which they were formerly entitled. People with less education tend not to live as long. Swedish children continued their education. Children in most European countries had a couple of months denied to them. Children in the U.S. are shut out of school for 6 months minimum!
Looking at this one number for a society is a lot like the way the American medical system evaluates itself. A patient who is on a ventilator for three years and is in a coma is considered a success. “We saved him,” the doctors will say. They look at one number: the heartbeat. They don’t look at the bigger picture of human health.
Math Expert:
Show me the math.
Me:
There is no “math” because nobody knows what will happen for the next few years. The countries that locked down created the ideal population for a coronaplague! If you make everyone in a society 5-10 lbs. fatter and in worse cardiovascular health because of 3 months of forced inactivity, you set them up for a massive wave of death from whatever virus comes along next (maybe just Wave #2 of coronaplague). My cardiologist friends mostly stopped working for months. Unless you think that cardiology is not important, you should expect plenty of extra deaths from heart disease over the next few years.
My friend’s 8th graders didn’t leave their suburban house for 3 months. That is not a normal life for a child. They are the subjects of an experiment that has never previously been tried. Maybe they will survive pretty well because my friends are well educated, the house is big/comfortable, and there is no domestic violence within their household. If you were to head into Newark and go to a public housing complex to find some 8th graders locked into a 2BR apartment the story might be different.
(The majority of my med school professor and physician friends, incidentally, believe that the shutdown was a mistake in terms of “saving lives”. They think that far more Americans will be killed from the shutdown of health care, from shutdown-induced obesity, and from shutdown-induced social ills than could have been saved by a shutdown (even if a shutdown had cut the number of Covid deaths to 0))
You are entitled to your opinion that the Swedes did the wrong thing in giving priority to children being able to go school, adults being able to socialize, work, and go to the gym. But you can’t prove that you’re right with “math”, any more than my med school professor and physician friends can prove that they’re right about Sweden having done the right thing.
Math expert:
It seems likely to me that the shutdowns bought enough time to save hundreds of thousands of lives, and if you can show me a real economic argument that indicates that the toll from the economic damage was comparable to that, go right ahead.
Me:
Maybe the effective Chinese shutdowns prevented a lot of Covid-19 deaths, at least until Wave #2 hits. But I don’t see how you can say that the U.S. shutdowns prevented a significant number of Covid-19 deaths given that the death rate from Covid-19 is pretty close to never-shut Sweden’s (maybe about the same if you adjust for urbanization; Sweden overall is more urbanized than the U.S.). The U.S. has experienced a death rate so far that is about 30% lower than Sweden’s [update: now forecast to be the same]. Is that worth all of the lives destroyed by shutdown, all of the education lost by children, and all of the cities destroyed by riots? Those aren’t questions that can be answered by a mathematician (even if we want to count up life-years lost we don’t have the data on how many we killed via our shutdown, as noted above).
After this discussion burned itself out (like the virus in NYC?), I realized that what I was trying to say was neatly summarized by the old expression: “An economist is someone who knows the price of everything and the value of nothing.” The Europeans who reopened their schools after a couple of months seem to understand this better than Americans do. A Covid-19 epidemiologist can tell you how many Covid-19 deaths your society has suffered and, perhaps, some things that you can do to reduce Covid-19 deaths going forward. But the Covid-19 epidemiologist can’t tell you whether Intervention A against Covid-19 is actually worth implementing because (a) the Covid-19 epidemiologist is ignoring deaths from all other causes, and (b) epidemiologists in general can’t tell us what human activities are worth accepting some risk of death. How many lives are we willing to sacrifice in order that our children can go to school? Obviously we are willing to sacrifice some, because all of the driving of children, teachers, and administrators to and from school causes some deaths. But the threshold number at which schools should be shut down is not something that any epidemiologist can give us.
Consider some 85-year-olds in a retirement home. Their life expectancy is 6 years (SSA). Suppose that they have a 3 percent risk of dying from Covid-19 if infected. Is it better for them to stay locked down for two years, until an effective vaccine is developed (we hope!), or resume their ordinary lives, which will carry a higher risk of coronavirus infection? The lockdown will take away more than half of the things that they enjoy in life, thus surely robbing them of 16-33 percent of their remaining life. Covid-19 could rob them of all of their remaining life (by killing them), but the probability of that even is fairly low. Can an expert decide for these 85-year-olds which option is actually better? No! The answer depends on whether the 85-year-old mostly enjoys Internet and TV, in which case maybe the lockdown is preferable, or mostly enjoys socializing with other humans, in which case running the risk of Covid-19 is preferable.
Readers: Is asking an epidemiologist whether to keep schools and playgrounds open like asking your accountant whether you should buy a dog? Yes, the expert can give you a bit of insight (“my other clients with dogs spend $4,000 per year on vet, food, and grooming”), but not a life-optimizing answer.