Back in 2016, I wrote “Reintroduce Prohibition for the U.S.?”, pointing out various advantages for American society if we could reduce alcohol consumption. This proposal was not well-received!
What about in the Age of Corona? Technocrats are gearing up for a massive testing and tracing operation. Example: “Here’s A Way To Contain Covid-19 And Reopen The Economy In As Little As One Month” (Forbes, by a Boston University econ professor). Excerpts:
The solution is PCR group-household testing of all American households every week. … If a household tests negative, each household member would be notified to go to their local pharmacy to receive a green wristband coated to change to red after one week.
This system is voluntary. But if you choose to have your household tested and receive your green wristband, you’ll be permitted by your employer to return to work, by your teachers and professors to return to school, and by proprietors to enter their restaurants, shops, cafes, etc. You’ll also be allowed to frequent the beach, attend concerts, go to the movies, …
Any household that tests positive will be required by the local board of health to quarantine in place for two weeks and then be re-tested. Households that don’t voluntarily get tested will be free to come and go as they wish. But without their green bracelets, they will have a hard time entering into workplaces and other establishments. Employers who hired the untested could face legal liability. The same holds for any business serving the public who lets someone onto their premises without a green bracelet.
My Dutch friend: “This will be just like it was for Jews after the Nuremberg Laws and similar. They were perfectly free, but couldn’t run a business, buy a movie ticket, or go to school.”
Electronic bracelets can also work: “People-tracking wristbands tested to enforce lockdown” (BBC). See also “US, Israel, South Korea, and China look at intrusive surveillance solutions for tracking COVID-19” (zdnet)
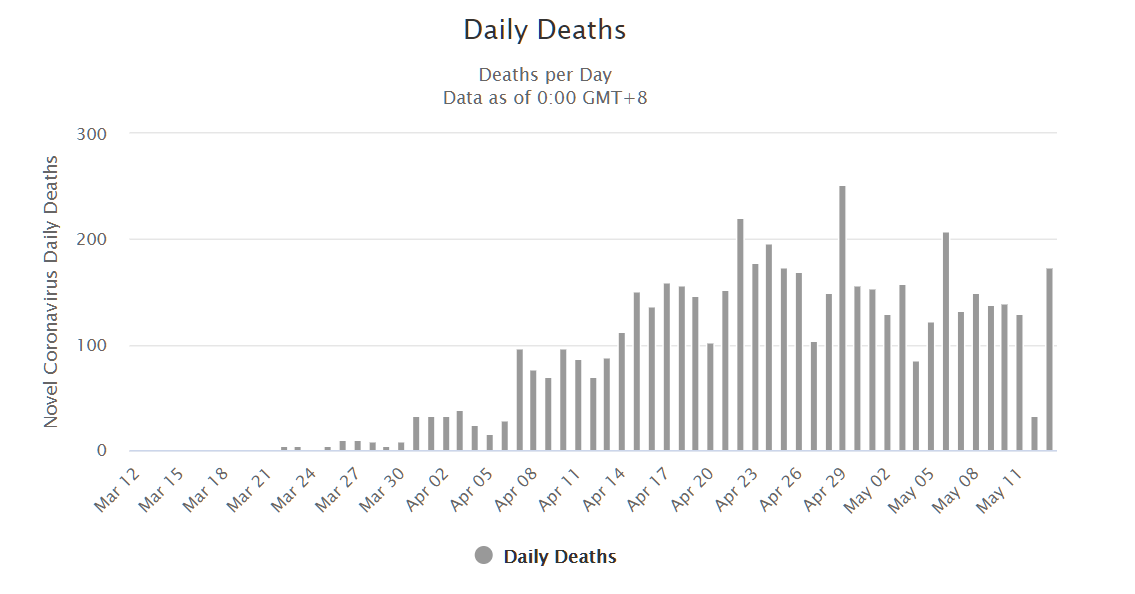
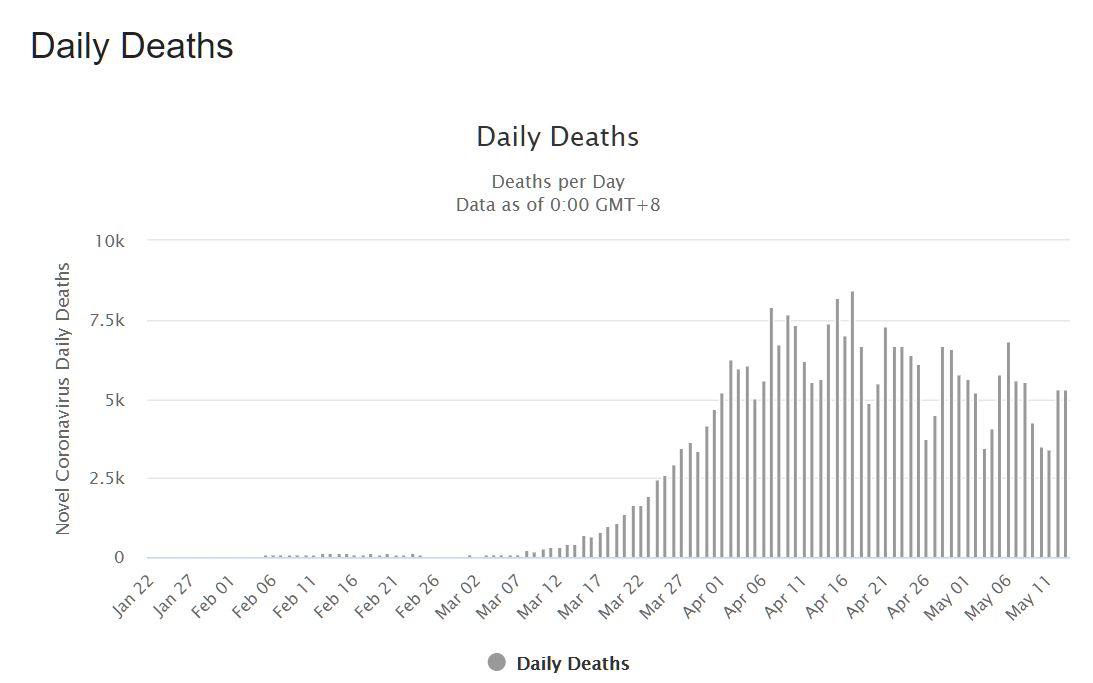
Covid-19 is a pernicious disease. It has killed nearly 300,000 people worldwide so far. But what if we could use the above technology and infrastructure to stop a much more destructive killer: alcohol. WHO says that 3 million deaths worldwide are attributed to alcohol. The average age of a death with/from Covid-19 in Massachusetts is 82 and more than 98 percent of those who died had “underlying conditions.” Alcohol often kills people who could have lived for another 40-100 years. In terms of life-years, therefore, we could save many more by discouraging alcohol consumption.
(Is Covid-19 different because an alcohol-related problem is due to a failure of personal responsibility? Consider the child of an alcoholic or a passenger in a car struck by a drunk driver.)
Given that people can brew their own beer or distill their own vodka, presumably it is not possible to achieve a 100 percent reduction in alcohol consumption. But if restaurants, bars, and airlines (to the extent any are left) were not offering alcohol to every customer and there were no convenient liquor stores (“essential”!), wouldn’t it be fair to expect at least a 10 or 20 percent reduction in alcohol-related deaths? (marijuana consumption increased following legalization in Washington State; shouldn’t we expect alcohol use to be reduced following prohibition?)
Since Americans have now decided that “saving lives” is more important than what used to be considered individual rights… If we succeed with alcohol prohibition using test/trace tech, why not use the same technology to attack HIV/AIDS, which has killed more than 700,000 Americans? (Covid-19 would have to kill 7 million Americans to take away a comparable number of life-years, due to the much younger age at which HIV/AIDS victims perish.) There continue to be 6,000 deaths annually here in the U.S., which is roughly comparable to the life-years lost from 60,000 Covid-19 deaths.
None of these public health interventions were doable in the 20th century. Epidemiologists predicted that HIV/AIDS would spread beyond the LGBTQIA+ community and kill millions of Americans. White upper-middle-class single Americans were terrified in the 1980s by this disease that merited cover stories of TIME magazine multiple times. Nobody would have tolerated the criminalization of sex outside of marriage in order to “save lives”. Today, however, there is no limit on the power of the government when there is a public health goal. (Maybe outlaw all sexual activity? If people want children they can be imported via immigration and/or produced locally and without HIV risk via IVF.)
Full post, including comments