Coronaplague in the Seychelles proves Dr. Jeff Goldblum’s theories?
From Coronaplague in India proves Dr. Jeff Goldblum’s theories?:
I wonder if this proves what Dr. Jill Biden, M.D.’s colleague Dr. Jeff Goldblum said: “Life Finds a Way.” The non-Chinese Wuhan-edition coronavirus was perhaps not a good fit for hosts in India, which is why, adjusted for population size, not much happened during Coronawave #1 (TIME: “health experts had predicted that India, with a population more than four times the size of the U.S., would quickly become the world’s worst-hit country”). But now the virus, with approximately 30,000 base pairs, has evolved.
From Wednesday, “Island paradise with highest vaccination rate reports world’s biggest COVID surge” (Yahoo News UK):
The Seychelles has suffered the world’s biggest surge in coronavirus cases – despite nearly 70% of its population having received a vaccine.
On Monday, the latest date for which figures are available, the archipelago’s seven-day case rate per one million people was 1,480, the highest in the world. It compares to the Maldives, the second highest, with 827 cases per million.
This comes despite 69.19% of people on Seychelles having at least one dose of a vaccine.
Health minister Peggy Vidot said: “Despite all the exceptional efforts we are making, the COVID-19 situation in our country is critical right now with many daily cases reported last week.”
Seychelles, with a population of about 98,000, currently has 1,068 active cases.
The BBC has reported the country’s news agency as saying a third of those active cases are among people who have received two vaccines.
Why is this interesting to those of us who aren’t planning to visit the Seychelles? I think it is a good window into what life in the Shutdown States (e.g., Maskachusetts, New York, California) will be like this coming winter. Everyone will be vaccinated and therefore the successful strain of SARS-CoV-2 will be whichever one can work its way around a vaccine-stimulated immune system.
Speaking of India, it does look as though the trend is following Farr’s laws (bell curve) and that the curve is flattening (either through heroic government and human efforts, if you think humans are smarter than viruses, or because this is how viral infections have worked for the past 3.5 billion years):
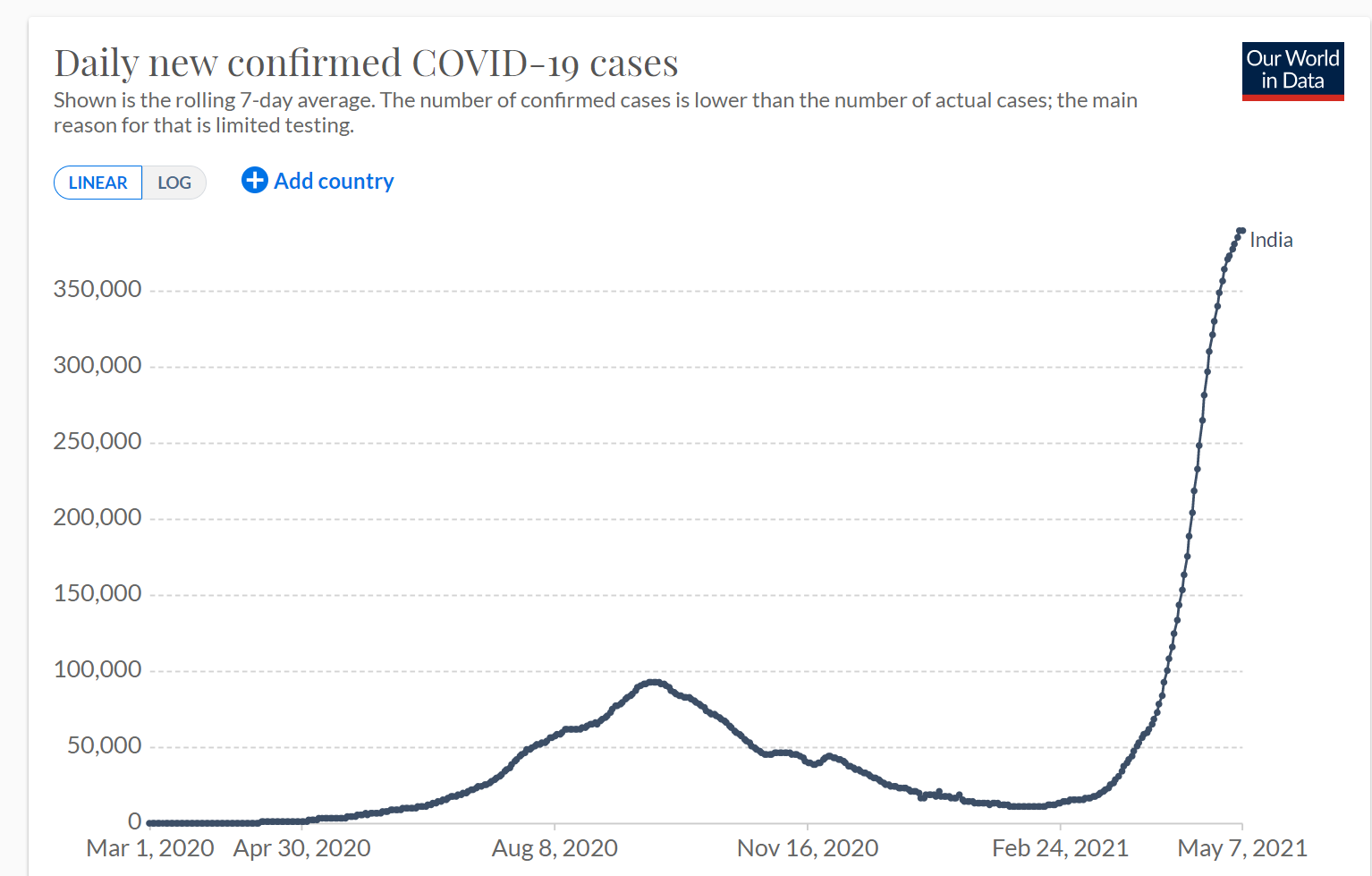
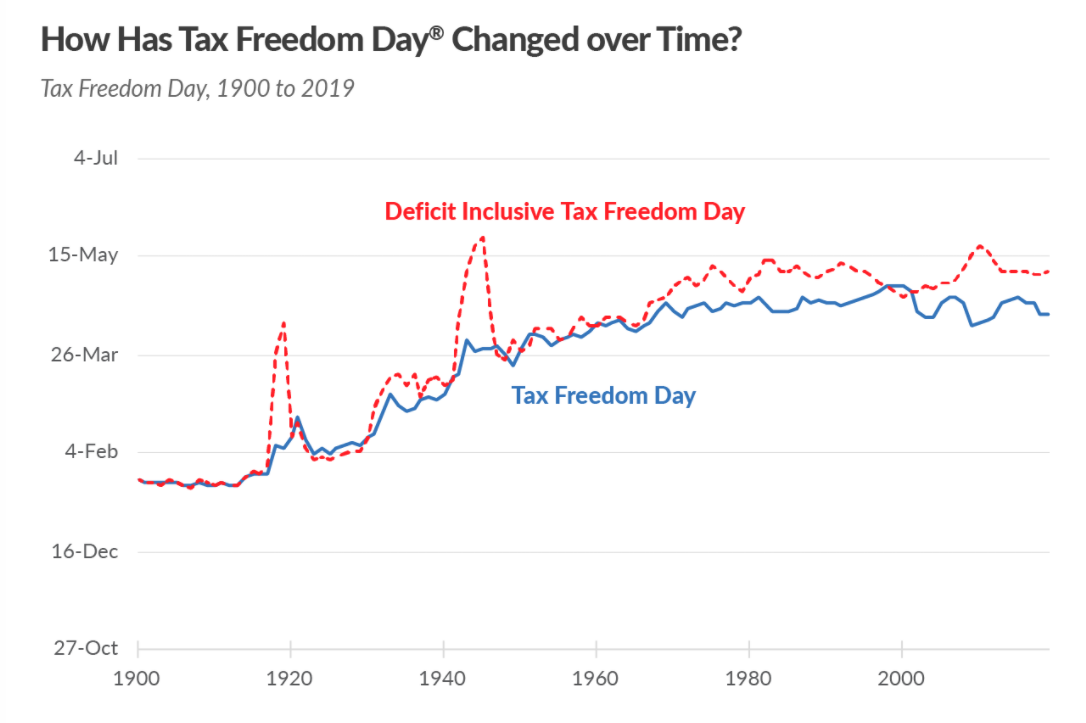
My latest thinking about coronaplague is that the Vietnam Wars, viewed from the American perspective, continues to be the best analogy. Technocrats in public health bureaucracies and state governors (except in FL and SD!) assure us with facts, figures, and charts that victory is within reach. We can be a few months away from victory for 10-15 years.
Full post, including comments