The problem with socialism is that it was never given a fair chance or a proper technocratic implementation, e.g., in the Soviet Union. Once President Harris or President AOC appoints properly credentialed agency heads, American Democratic Socialism will serve as a City on a Hill-style demonstration to countries around the world.
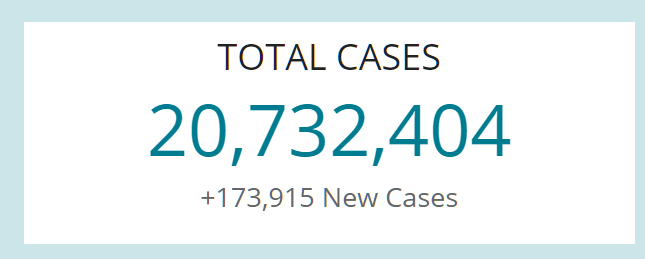
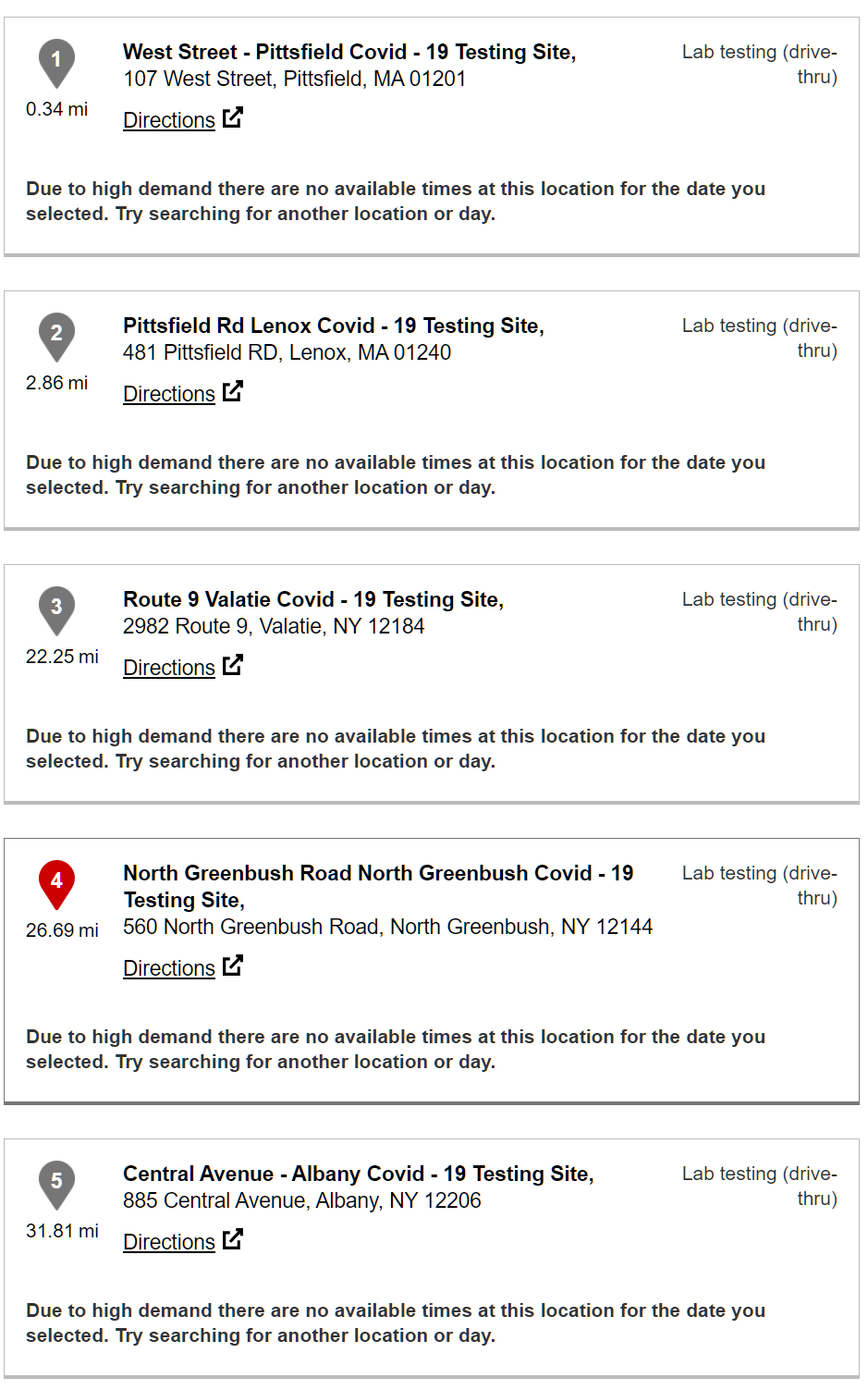
My Facebook feed is alive today with Bigger Government enthusiasts decrying the fact that state health departments (New York’s has more funding than the entire Russian military, but our media characterizes these departments as “chronically underfunded”) are not managing to distribute the vaccines that the Feds shipped to them. Presidents Biden and Harris will fix the problem starting on January 20, according to my friends, but we are still left with three weeks of what is, in their view, incompetent and slow distribution (at current injection rates, the U.S. is on track to lose 40% of the paid-for vaccines to expiration).
Stats from the NYT:
(Note that New York and New Jersey collect more in state/local taxes, as a percentage of residents’ income, than 47 other states, but they’re still on track to have expired vaccine doses.)
An interesting aspect of this is that the failure of central planning for vaccine distribution has not dimmed anyone’s enthusiasm for more central planning in other parts of the economy. The solution for dealing with scarcity is not a market and prices, but rather more and better technocrats.
Separately, I’m wondering how anyone who has recently gotten a flu shot in the U.S. thought that this would go quickly. From Do they still line up kids at school and give them shots? (2018):
The other day I was waiting for a friend at CVS so decided to use the time to get my “free” (i.e., included in my $10,000/year Obamacare policy) flu shot. Ten minutes later my friend showed up. It took roughly another ten minutes before the shot was “ready.” It turned out that three health care professionals had to process various forms on a computer screen, get a one-page questionnaire from me, and finally deliver the shot with a simple needle (less than one minute). A licensed pharmacist was required as part of the paperwork pipeline.
I wonder if something more like a market economy could have done this better. The bureaucrats can send free vaccine doses to hospitals, medical and dental offices, and nursing homes. Whatever is left over goes to whatever clinic or facility bids the highest. The bidding process is necessary to ensure that clinics that have the most streamlined and efficient procedures are the ones who will get the vaccine and also to ensure that clinics won’t let doses get spoiled or expire.
The auction-winning clinics and facilities can then use conventional web-based services to let people book slots and pay for vaccines at whatever prices they want to charge. Presumably the people who are at highest risk will recognize their risk and be willing to pay the most.
The obvious objection to the above is fairness. Rich people who aren’t scared of the barely tested vaccines will happily offer their Platinum cards. But maybe this is actually good from an epidemiological and economic point of view. Rich people tend to travel a lot (via private jet, of course, and including internationally throughout all of 2020) and, if the vaccines do stop transmission, vaccinating them will slow down the pandemic. Those rich people who are vulnerable and/or especially fearful and who have therefore been hiding in oceanfront bunkers will go out and spend a lot more money once vaccinated.
We could deal with the unfairness by simply sending out money to the people whom we want to get vaccinated. Use payroll data to send out checks to essential workers. Use Social Security data to send our checks to old people. Use insurance claim (including Medicaid and Medicare) databases to send out checks to those with BMIs over 30 (goal!) or other health conditions. The check recipients could decide whether to stay bunkered, N95-masked, bathed in hand sanitizer or to use the check to pay the going rate for the vaccine.
At least to judge by my Facebook feed, there are a lot of suburban white and Asian Americans who feel that the cost of lockdown is negligible. They’re happy to work from home (4,000 to 6,000 square feet), order deliveries, refrain from socializing in person. These folks don’t need a vaccine because if the government recommends that they stay home for the next 5 years they will cheerfully comply. But, on the other hand, there is no central database of the Happily Shutdown. Thus, the market would be the best way to keep these folks from clogging up the vaccine line. They know that they’ll be home for another year or two, so why should they pay $500 for a shot? They’ll wait for the price to come down to $100.
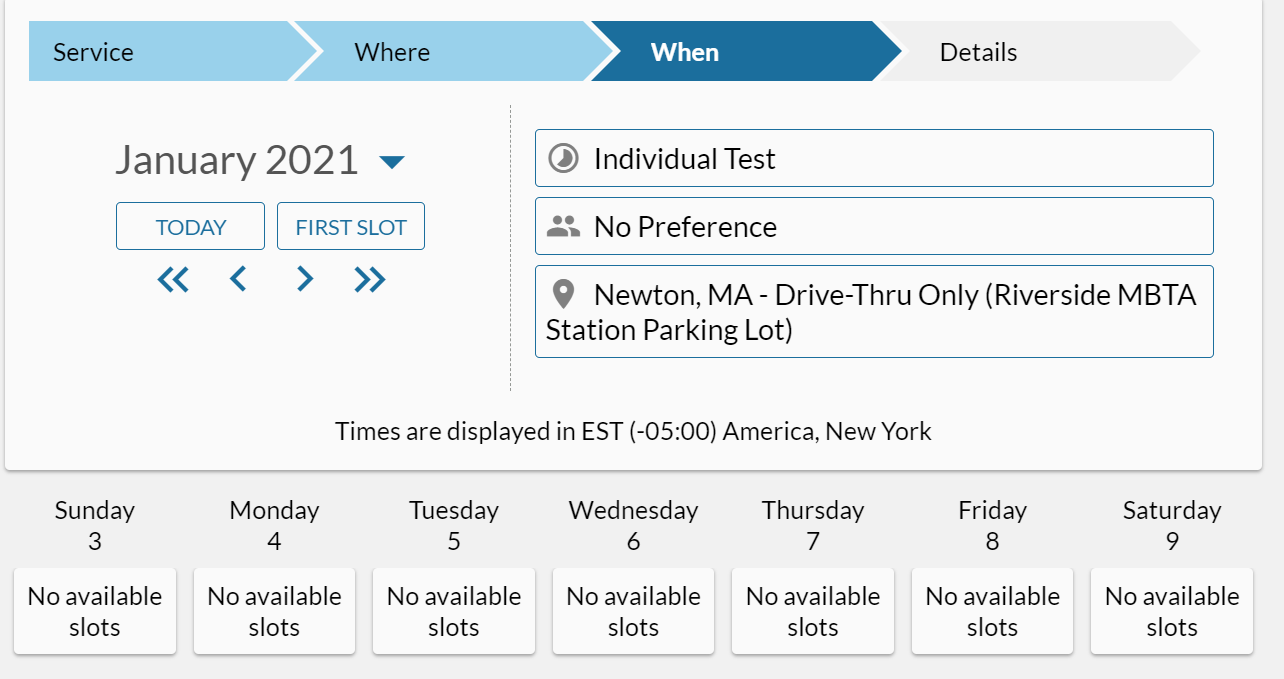
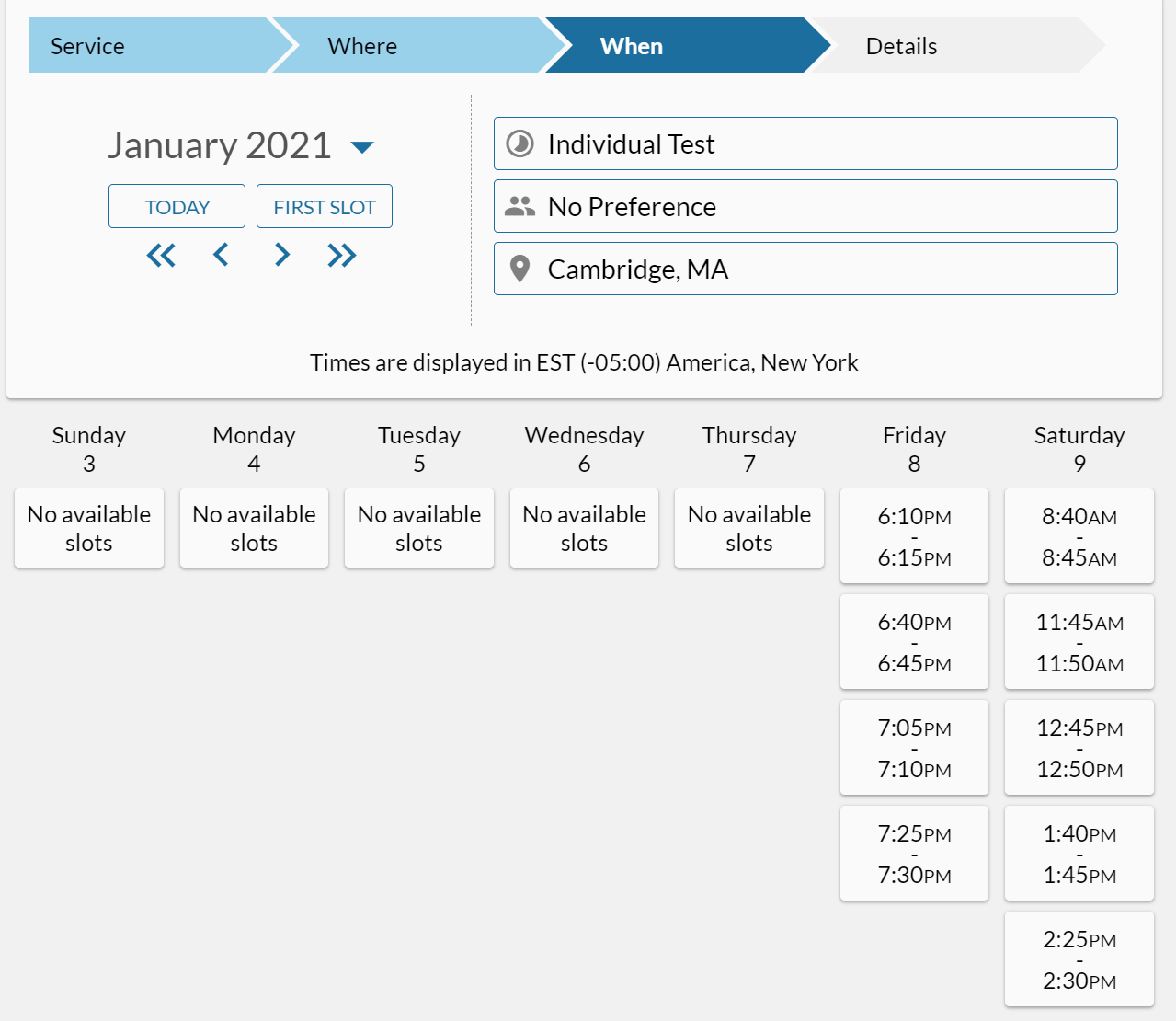
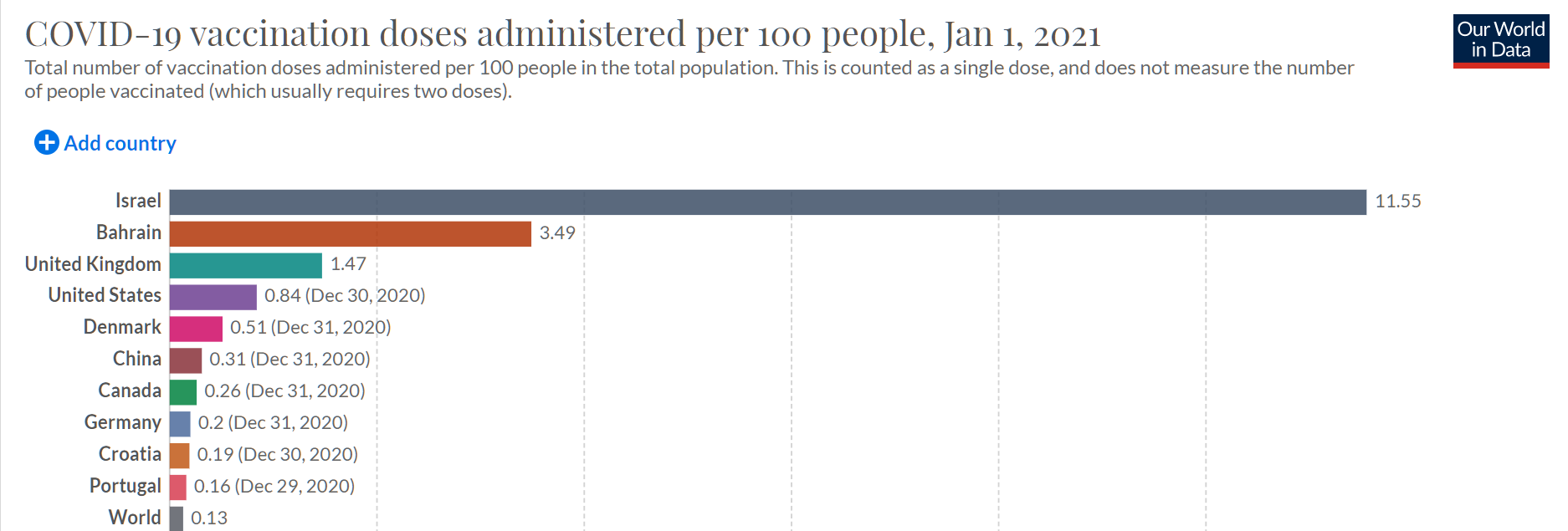
Update… We can watch the needle sticks unfold in real time:
Universal health care is plainly way better than whatever we want to call our system, since Israel, Bahrain, and the UK are well ahead of us. Also, universal health care is plainly way worse than the U.S. system: Denmark, Canada, Germany, Italy, and France are way behind us.
Second Update: We could also run this as a bounty-based system. The government gives away the vaccines to existing state-licensed clinics, such as CVS MinuteClinic, etc. Then the government says “You get $500 for every person over 80 whom you inject, $250 for every person over 70, and $100 for anyone else. There is a bonus of $200 for every shot in a person with a BMI over 40 and $100 for everyone with a BMI over 30.” Would we have vaccines expiring in freezers? The FAA did this with pilot briefings back in the 1980s. They let two contractors compete to offer computer-based weather information to pilots so as to discourage pilots from calling human briefers. The two contractors ran advertisements, enhanced systems, built web versions at around the same time as Amazon launched, etc. Other than writing checks, the FAA never had to do anything to get people to switch to briefing via computer system other than open up an API on their mainframes.
Related:
- “Here’s Why Distribution of the Vaccine Is Taking Longer Than Expected” (NYT): Health officials and hospitals are struggling with a lack of resources. [18% of GDP is not sufficient to run a health care system] In Puerto Rico, last week’s vaccine shipments did not arrive until the workers who would have administered them had left for the Christmas holiday. [Coronaplague is an emergency, but not such a serious one that people should work through traditional vacation periods] In one notable blunder, forty-two people in Boone County, W.Va., who were scheduled to receive the coronavirus vaccine on Wednesday instead were mistakenly injected with an experimental monoclonal antibody treatment. [18% of GDP is not sufficient to run a system in which people get the intended shots]
- Roughly half of the front-line health care workers whom the central planners targeted for #1 priority don’t want to be early adopters of these vaccines and are refusing to be injected: NBC
- Update: a reader pointed me to “Free Market Vaccines”, a December 7, 2020 post by the always interesting John Cochrane: economics should start with “to the highest bidder,” and come up with some well documented market failure, and a public allocation system that mimics the highest bidder allocation. … In India, meanwhile, that bastion of… informal.. if not free markets, it appears you can sign up to buy the vaccine, for about $8.”
Full post, including comments