“Boston is well known as ‘The Cradle of Liberty,’ and for nearly 400 years Boston has led the way in providing equal human rights for all of its citizens. Over 5 years ago, on May 5, 2010, The Boston City Council passed a Unanimous Resolution In Support of An Act Relative to Gender-Based Discrimination and Hate Crimes (S. 1687/H.1728). Because the Massachusetts Legislature has still not passed this important Human Rights Bill, Boston Mayor Marty Walsh is today taking a very courageous and important action by making two restrooms in Boston City Hall Transgender Inclusive. …
Boston mayor Michelle Wu announced Monday that the city will require proof of vaccination for indoor recreational activities and will tighten the vaccine mandate for city workers.
The moves are intended to tamp down the city’s winter surge of COVID-19 cases and the threat of the emerging omicron variant.
Beginning Jan. 15, people aged 12 and up looking to patronize venues like gyms, restaurants and museums will have to present proof of at least one vaccination dose for access. The following month, everyone aged 12 and up will need to present proof of vaccination through an app, a CDC vaccination card, or photo of a vaccination card, or other official immunization record.
Children ages 5-11 will be phased into the new requirements on a slightly extended schedule and won’t have to provide proof of first vaccination doses until March 1. Then, beginning in May, children will need to show proof of full vaccination.
“This is a response that is rooted in science and public health and we need to take every available action to protect our city’s residents, businesses and institutions,” Wu said of the testing elimination.
Where did the scientist learn #Science? According to Wikipedia, while majoring in economics as an undergrad. Where did the public health expert learn medicine? At law school. What about the paranoid conspiracy theories of the Deplorables that a cabal of elites are controlling every aspect of American life? Mx. Wu attended Harvard University for both bachelor’s and law school.
What does the manufacturer of the drug that will be required for children to leave the house say about this medicine? The label: “this unapproved product… which is not an FDA-approved vaccine.”
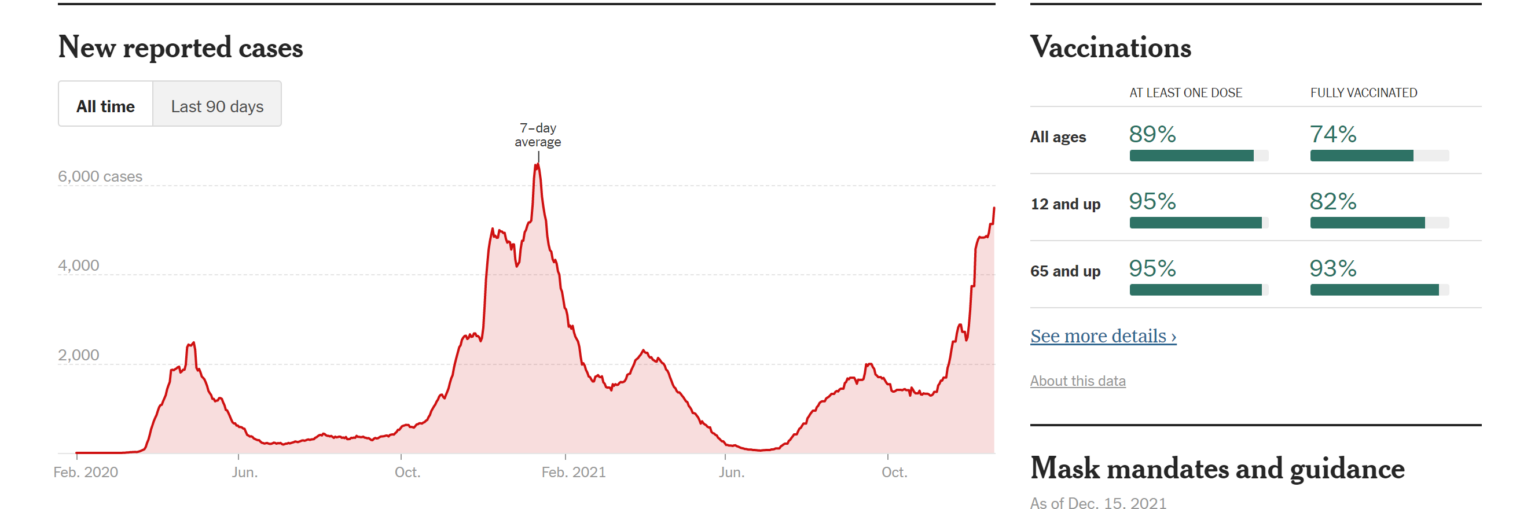
With 95 percent of subjects, age 12 and up, having received at least one shot, is SARS-CoV-2 giving up on life in the Cradle of Liberty? NYT:
SARS-CoV-2 is a sufficiently serious enemy that the Inglewood, California schools shut down completely for more than 400 days and, even after that, reopened only in a diluted “hybrid” form (source). Karen takes COVID-19 seriously enough to deprive children of an education (albeit not seriously enough to shut down the alcohol and essential marijuana stores for adults).
What’s Karen planning for February 2022? Super Bowl LVI, which will bring more than 100,000 ticket-holders together simultaneously in the (mostly enclosed) Inglewood, CA stadium (closer to 200,000 in and around the stadium and nearby hotels if we count support staff, hospitality workers, etc.?).
A free state such as Florida or South Dakota could host a Super Bowl without hypocrisy, but how can California in general or Los Angeles County in particular? COVID-19 was serious enough to warrant closing schools and imposing vaccine papers checkpoints on gathering places, but not serious enough to refrain from pulling 200,000 people from every corner of Planet Earth into close proximity? Even if they are righteously masked in the stadium (0-11% reduction in spread!), they’re inevitably going to be partying indoors and unmasked (#BecauseEatingAndDrinking) in big crowds before and after, no?
Separately, how could the National Football League have taken the risk of scheduling the game in California? What if the #Science-following Covidcrats decide that public health is more important than mere profits and shut down the event? A lot of $5,000 tickets will have to be refunded, no?
Day 1, evening: temperature down to 100. Friend in our chat group recommends monoclonal antibody treatment, available to anyone in Florida and to a subpopulation identified by technocrats in Massachusetts. The enthusiast for this emergency use authorized IV drug: “Make up a condition if you need to. Don’t risk dying.” I chime in: “I don’t think an IV drug is the right thing to do. Not unless it seems like it is getting worse. Most new medicines work a lot less well than initially claimed and have more risks than initially claimed.” Our mutual friend: “You have to get it right away! Don’t wait for it to get worse. Tomorrow!” We seek advice from a cardiologist mutual friend in a separate chat: “Nope. [Regeneron is] overused in Florida. No hard core data but people favor 30 days of aspirin. At least 81 mg. It’s thought to cause pro inflammatory, pro coagulatrice [?] state.”
Day 2, morning: Right now about 100F in each ear. Throat doesn’t hurt as much, coughing subsided. Although now that i wrote that it subsided i needed to cough. I can feel the vaccine working.
Day 2, afternoon: Gone. It was pretty much gone this morning.
One thing I learned: at least in Massachusetts, it is essentially impossible to figure out what to do with a K-12 child when a parent is sick. I visited the web site of the $25,000-per-student-per-year public school that my diseased friend’s kids attend. You’d have to spend at least 45 minutes pulling down disparate documents and reading through them to get a high-level understanding of the policies. At the end of this, however, you’d still be uncertain regarding what to do with children whose parents are on track for death via COVID. You’d think they would have a little web form asking “Are you vaccinated? Is the young scholar vaccinated? Is the young scholar symptomatic? …” and then a red or green answer appears via the miracle of JavaScript.
(It turns out that Day 2 of my friend’s Inexorable March Toward Death coincided with a TikTok panic regarding violence on 12/17 (see “Schools across US cancel classes over unconfirmed TikTok threats”) and, thus, kids all around the country spent the day learning from Professor Xbox.)
Since we all, I hope, #TrustScience and #ListenToDoctors, how about asking a doctor whether children of a COVID-positive parent should go to school? A physician friend copied/pasted this from one of her all-doc discussion groups:
I have had three pfizer doses, booster was in mid-September. My three kids were 14 days post pfizer #2 on Saturday. Today I watched one of my daughters compete at the state gymnastics championships, and I was wearing a kn95 the entire time, cursing all those around me who were blatantly disregarding the mask requirement. As we left the gym, I felt slightly sneezy. I thought it was just from wearing a tight mask for over three hours. I went to pick up one of my other kids who had spent the night with my mom and stepdad. We ate pizza together. Later in the evening, I felt a little sniffly, so I did a binax now and it was instantly positive🤬 My husband is also vaxxed and boosted, binax negative, and plans to go to work tomorrow. What do I do with my fully vaxxed kids this week? Must they quarantine if asymptomatic? I will get us all pcr tested tomorrow and plan on testing the kids/husband again in five days if negative. Can anyone give me any assurance that my mom and stepdad (both fully vaxxed and boosted with pfizer) will be okay if they get this from me? I am freaking out at the thought of them getting sick.
Note that this physician implies that the incubation time from exposure to symptoms is only a few hours. And the doc sends the husband out from the plague-infested house into the workplace where he/she/ze/they can infected dozens of others after what could easily be a false negative test. And the doc is just as confused as the rest of us regarding what should be done with the kids.
Speaking of COVID and symptoms such as brain fog, we removed the front license plate from our Honda minivan yesterday and discovered that the dealer had made two attempts to screw it into the plastic bumper, thus leaving six ugly holes. I had an email exchange with a company that specializes in paint-matched plugs for just this application. I sent the following photo:
The expert’s response: “Is the dealer tech who did this still alive? That’s insane.” But perhaps it was long COVID brain fog that can be blamed, rather than insanity? I could reinstall the bracket (a third set of holes?) to cover this ugliness. I asked The Google for “decorative front license plate”. Here’s the first non-ad result:
(How is it legal to sell a hate-filled license plate with inflammatory language, as shown above (i.e., shouldn’t that last one read “Boy Birthing Person”?))
I’m thinking a custom photo-printed plate with an image of Mindy the Crippler. Now that my friend’s brush with death seems to be over (until the next variant emerges), what do readers suggest for the nose of the minivan?
Insider spoke with nine leading experts, who took their best guesses about how long vaccine protection may last. Those predictions were quite a bit longer than what pharmaceutical companies suggest: Some experts said boosters probably won’t be necessary for another one to five years, while others questioned whether the general public will ever need another round of shots.
Early studies also suggest that the mRNA shots from Pfizer and Moderna offer more robust protection than natural immunity from an infection.
“Vaccines, actually, at least with regard to SARS-CoV-2, can do better than nature,” Dr. Anthony Fauci, the US’s leading infectious-disease expert, said in May.
“If I had to look at my crystal ball, it’s probably not sooner, hopefully, than a year after being vaccinated, for the average adult,” Dr. Peter Marks, director of the Food and Drug Administration’s biologics center, said during a recent webinar.
Other experts think protection may last far longer. Dr. Paul Offit, director of the Vaccine Education Center at Children’s Hospital of Philadelphia, estimates it could be three to five years. “I would predict that protection will last for a few years — protection as I define it, which is protection against severe to critical disease,” Offit told Insider last month.
Pfizer CEO Albert Bourla estimated in April that people would likely need booster shots within 12 months of getting fully vaccinated. That’d be as early as December for some in the US.
From University of Colorado, February 24, 2021, quoting the director of epidemiology for the Pandemic Response Office at CU Boulder:
… we know that the vaccine efficacy lasts at least eight to 10 months. But immune cell—called T-lymphocytes as well as B-lymphocytes—can stick around in the body for years, breaking into action quickly if the body ever encounters the same virus again. So, it’s likely that protection from severe disease and hospitalization could last for many years.
Two months after the vaccines were authorized for emergency use, in other words, scientists actually knew for certain that protection would last for 8-10 months.
Although no rigorous study has yet analyzed whether vaccinated people can spread the virus, it would be surprising if they did. “If there is an example of a vaccine in widespread clinical use that has this selective effect — prevents disease but not infection — I can’t think of one!” Dr. Paul Sax of Harvard has written in The New England Journal of Medicine. (And, no, exclamation points are not common in medical journals.) On Twitter, Dr. Monica Gandhi of the University of California, San Francisco, argued: “Please be assured that YOU ARE SAFE after vaccine from what matters — disease and spreading.”
Readers: Any favorite predictions from earlier in 2021 that you can find? One of the most interesting things about coronaplague is that Americans consider a discipline that is unable to make accurate predictions to be a “science”.
Kim Taylor, 73, of Wellesley, had been volunteering at Cultivate Care Farms when she was repeatedly rammed by a sheep on Saturday morning, according to NBC Boston, citing Bolton police.
According to police, all the livestock at Cultivate Care Farms are comfort animals and that the site assists people as part of an attempt to improve their mental health.
This post is not about the sad event, but about the choice of language.
Let’s consider a 79-year-old President of the United States? Not “elderly,” according to Newsweek (Google search for “joe biden elderly site:newsweek.com”).
How about a 73-year-old who dies with/from COVID-19? (9 years younger than the median age of a COVID-19 death in Maskachusetts) Would our media characterize this person as “elderly”? Or imply that he/she/ze/they would otherwise have looked forward to decades of health and vigor?
A friend woke up this morning with a 102-degree fever. He asked our chat group what the procedure was for getting a COVID-19 test in suburban Boston. Keep in mind that this is one of the epicenters of COVID-19 Karenhood. To minimize deaths tagged to COVID-19, no price is too high to pay in dollars, deaths due to shutdown non-COVID health care, inconvenience, and long-term deaths due to lockdown-related obesity, lack of education, poor mental health, etc. Healthy college and K-12 students are tested weekly, for example. Vaccine papers are checked in numerous situations, e.g., to attend college or a concert (folks say that preventing COVID-19 is their #1 priority and then crowd into a 2,700-person concert hall, relying on proven-ineffective cloth masks for protection). Schools in Boston were closed for more than a year. Certainly a big slice of the $10 trillion that the Feds have spent on coronapanic has been spent in Maskachusetts.
If we intersect the above two paragraphs, shouldn’t the result be a computer system that can tell a Massachusetts resident where to get a Covid test today? If not from the government (healthcare.gov was a rough development project!) then from a righteous private company?
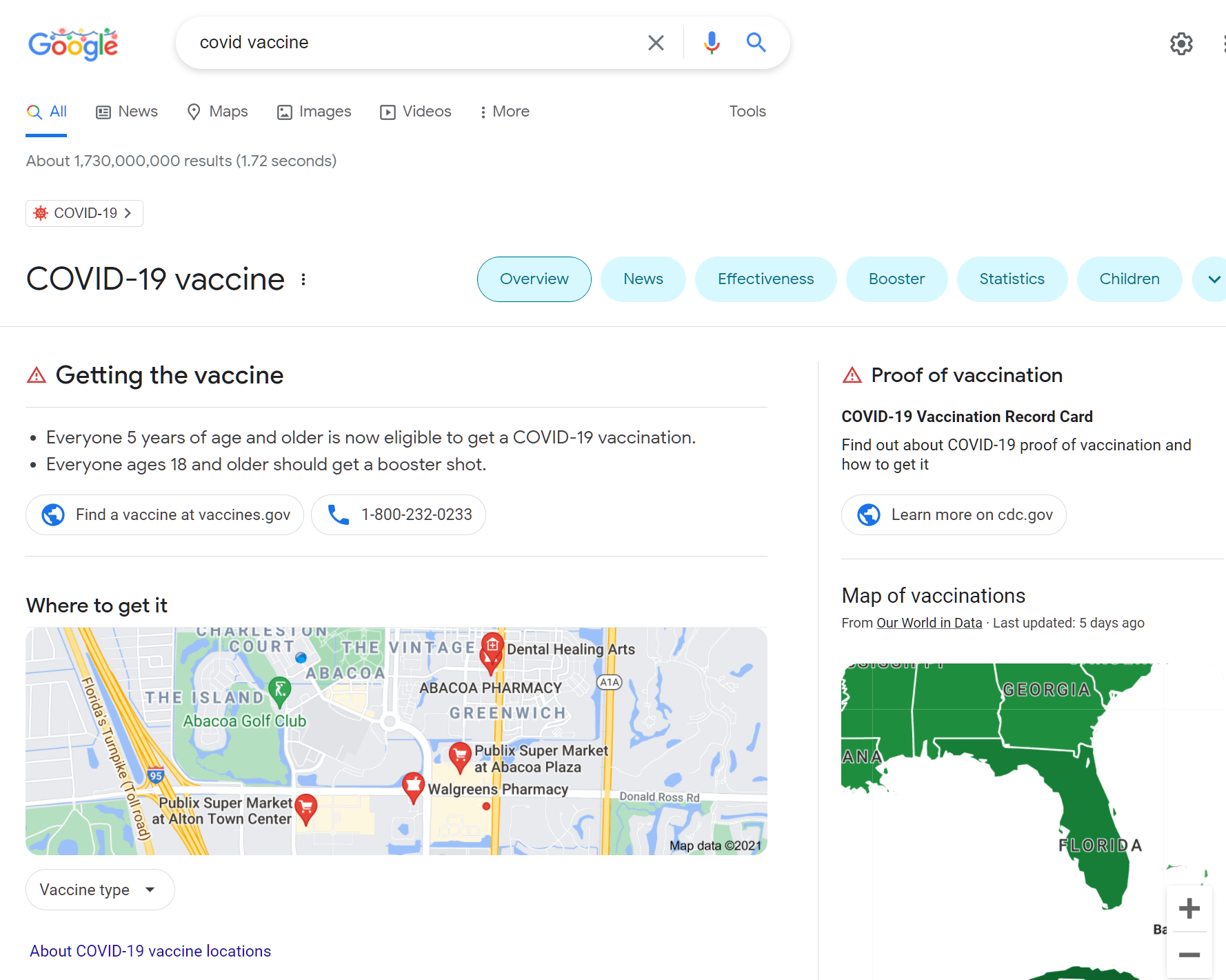
We’re now nearly 2 years into 14 days to flatten the curve. The health care industry is fully computerized. The Internet monopolies such as Google and Facebook devote considerable effort to Karen’s propaganda campaign. Searching for “covid vaccine” in The Google:
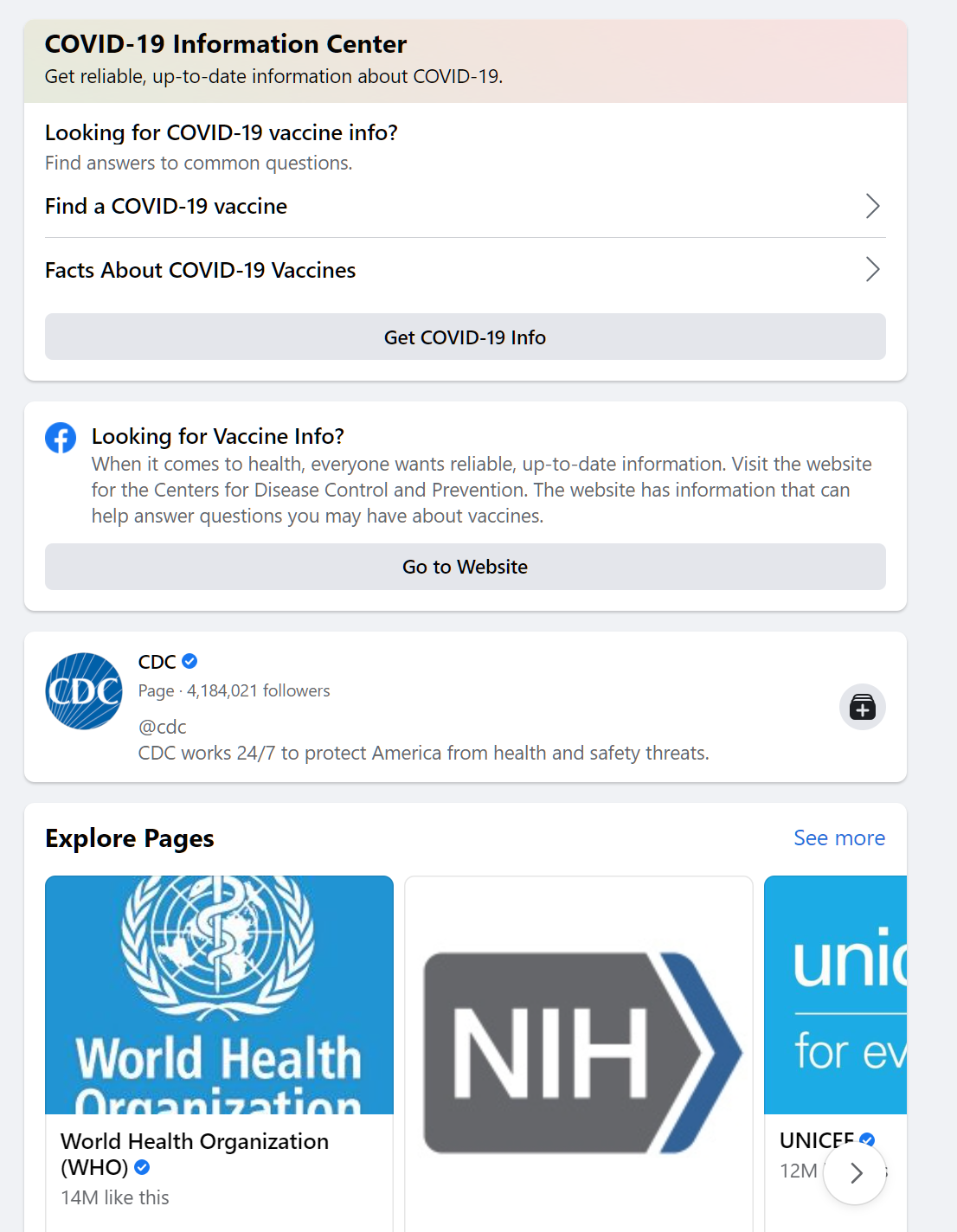
Searching for “vaccine” in Facebook:
Facebook corrects vaccine misinformation. A physician friend posted “Flu variants yearly warrant new vax; yet #CDC pushes Covid “booster” -retreads”. A pilot friend posted “Mengele is admitting that these vaccines are not working. He knows something is coming, and he tries to protect his ass.” over a video of Saint Fauci. A physicist posts European data: “I had more than a year ago posted a study by the Italian ISS, published in August 2019, on those recurring peaks of excessive mortality in the previous decade. It showed that the magnitude of excessive deaths, among the same statistical population (over 65) and in most cases even with geographical correlations (areas of northern Italy) were comparable with COVID mortality. In my view, whoever is intellectually honest will admit from these data that lockdowns, vaccine mandates, etcetera, were and are not justified by the numbers.” An attorney: “My wife is a nurse in a hospital here in the Boise area. Not only are they letting nurses go for not having the vax, and bringing in travelling nurses who are not vaxxed, but they are paying the travellers more than twice as much as their full-time nurses. It is freaking insanity”.
Underneath all of these Facebook adds the following:
What if you try to use these titans of information technology to find a Covid test? Searching for “covid test” in Facebook yields instructions to wear a mask and an ad for CVS. Search for “covid test” in Google Maps yields nearby facilities that might do tests, but with no information about whether they have availability, require appointments, charge money, etc.
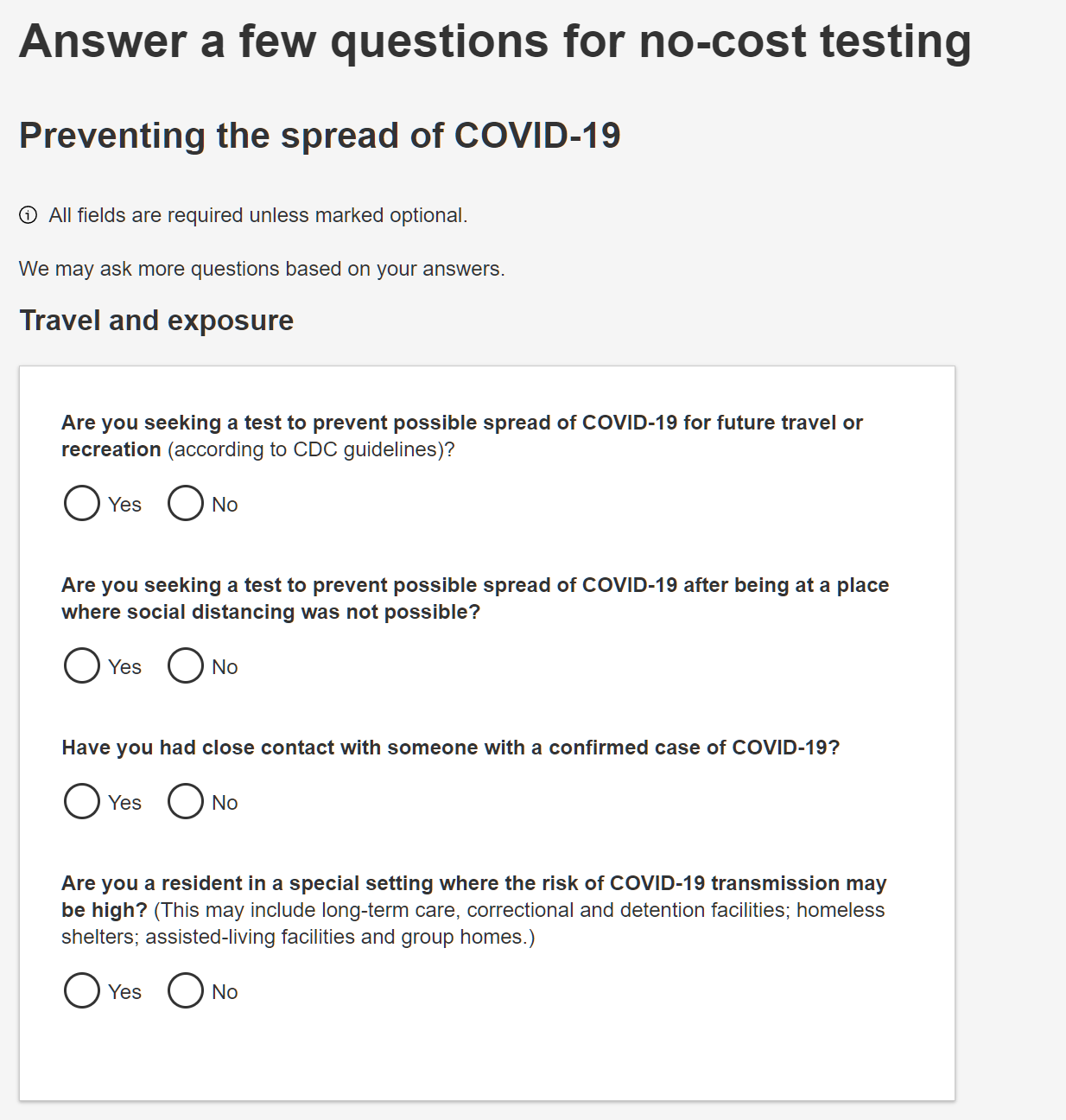
Since my friend isn’t feeling well, I tried to find him a test appointment. The various CVS stores are prominent in search results. When you follow the link from Google Maps it takes three clicks and typing in a ZIP code to get to a questionnaire:
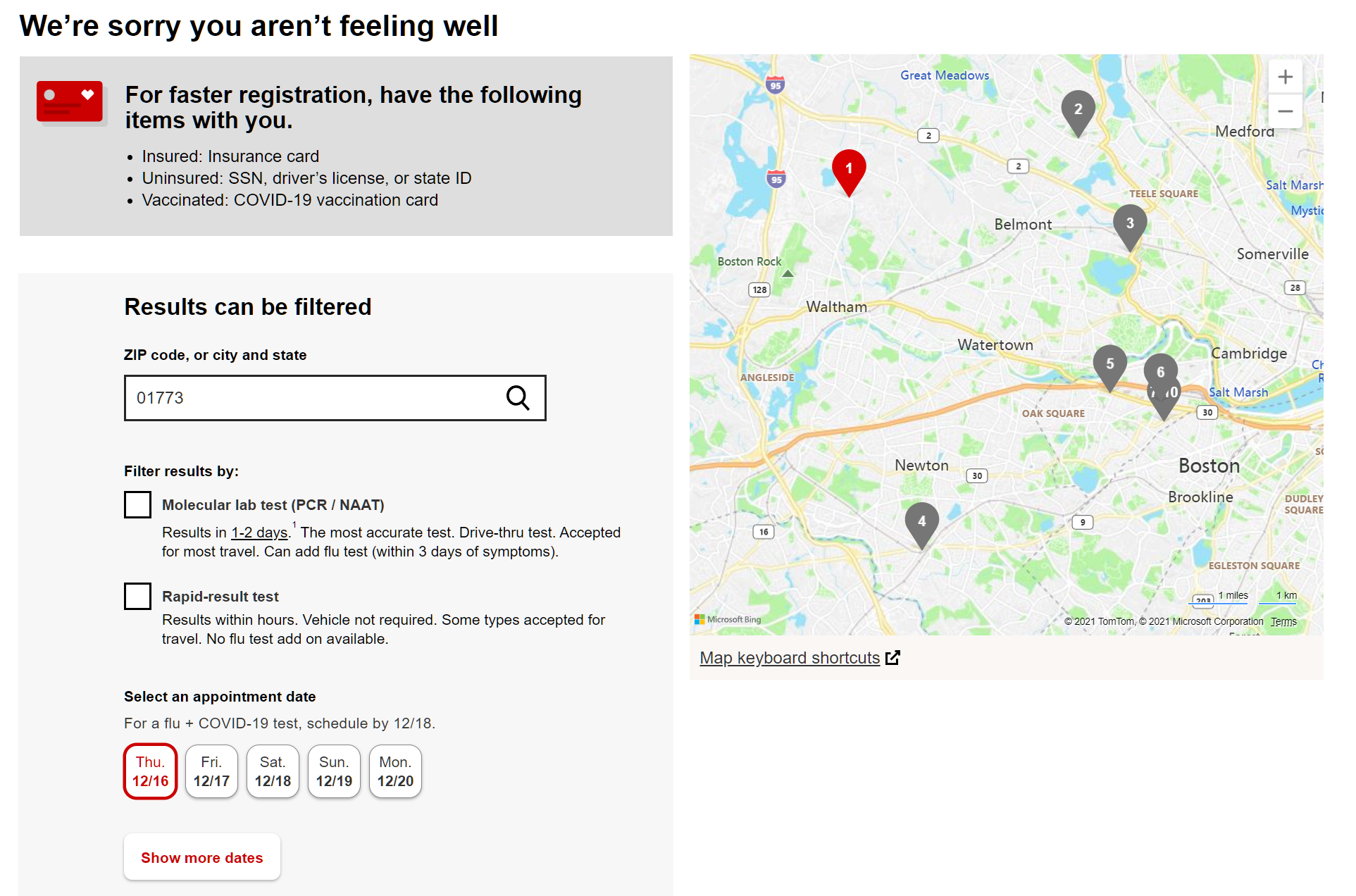
I type fairly fast, but it took me roughly 2 minutes to get to a page of available locations:
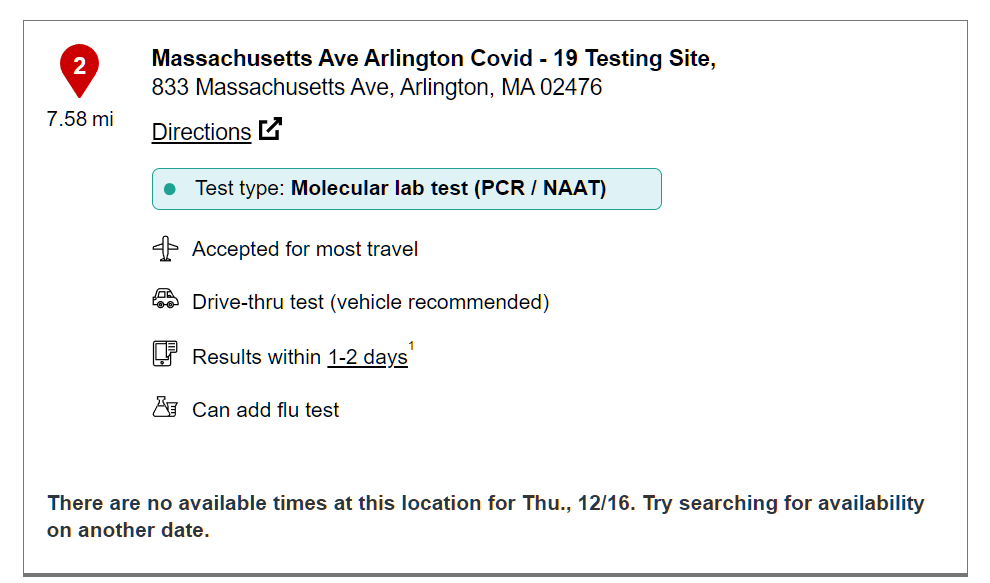
The CVS site showed availability for today at various stores, inviting me to click on “Check for available times” but the result of the click was always “no available times”:
In Florida, it should be a lot simpler for Google and Facebook. They can highlight the government-run drive-through free testing centers that never seem to have a line and that don’t require any appointments. Yet this isn’t done. Instead, Google Maps shows urgent care clinics, pharmacies, etc. that may require appointments, payment, etc.
After $10 trillion has been spent, why should a person with a 102-degree fever have to spend more than 2 minutes on the Web to find a reasonably close and convenient COVID testing option?
Update: After a full day of web-searching and driving around, my friend scored a Binax rapid test kit (one-hour round-trip drive). Verdict: POSITIVE. Another success story for Moderna! (second shot six months ago) I think it is safe to assume that, without the vaccine, my friend would now be dead.
Vito Corleone’s funeral (I asked, in the chat, “What size grave would you like us to dig for you?” and the feverish guy responded “I want a nice hardwood coffin with brass handles and a lot of flowers.”)
“Demand for COVID-19 testing, booster shots high as Christmas approaches” (WCVB (Boston), 12/16)): Near the Square One Mall in Saugus, a long line of cars snaked through a parking lot Thursday evening. The drivers and passengers were waiting for their chance to get tested in a scene reminiscent of the long lines seen last year before vaccines were widely available.
Maybe things are better in Maryland, close to the Vatican (St. Fauci’s office)? “COVID surge calls for more testing, but options are now more difficult to come by in Maryland” (Baltimore Sun, 12/14): As Maryland experiences the first signs of another winter surge, COVID-19 tests are now more difficult to come by. … The pharmacy chains also offer in-person test appointments, but scheduling one often has to be done days in advance to reserve a spot….
How about in New York, where Emmy Award-winner Andrew Cuomo’s wise decisions continue to keep people safe? “Testing Demand Has Doubled in NYC Over Omicron Fears” (New York, 12/15): With the Omicron variant expected to bring a surge of U.S. cases, socially distant lines snaked outside many coronavirus testing sites throughout the city this week. Anecdotes spilled in across the city of waiting hours to get swabbed.
Loyal readers will remember that, ever since January 2021, I’ve considered the Vietnam War to be the best analogy to American efforts in the fight against SARS-CoV-2 (see Lockdown is our Vietnam War so it will end gradually? and Vietnam War analogy for COVID-19 holding up?). As bad an idea as the Vietnam War might have been, from an economic point of view, this comparison is unfair to the folks who supported the Vietnam War for 15 years because coronapanic spending in the U.S. has been roughly 2X the cost of all U.S. wars combined and vastly more than what the U.S. spent on the Vietnam War (the spending on which was blamed for the massive inflation of the 1970s).
In the United States, during the Cold War, the missile gap was the perceived superiority of the number and power of the USSR’s missiles in comparison with those of the U.S. (a lack of military parity). The gap in the ballistic missile arsenals did not exist except in exaggerated estimates, made by the Gaither Committee in 1957 and in United States Air Force (USAF) figures. Even the contradictory CIA figures for the USSR’s weaponry, which showed a clear advantage for the US, were far above the actual count. Like the bomber gap of only a few years earlier, it was soon demonstrated that the gap was entirely fictional.
John F. Kennedy is credited with inventing the term in 1958 as part of the ongoing election campaign in which a primary plank of his rhetoric was that the Eisenhower administration was weak on defense. It was later learned that Kennedy was apprised of the actual situation during the campaign, which has led scholars to question what Kennedy knew and when he knew it. There has been some speculation that he was aware of the illusory nature of the missile gap from the start and that he was using it solely as a political tool, an example of policy by press release.
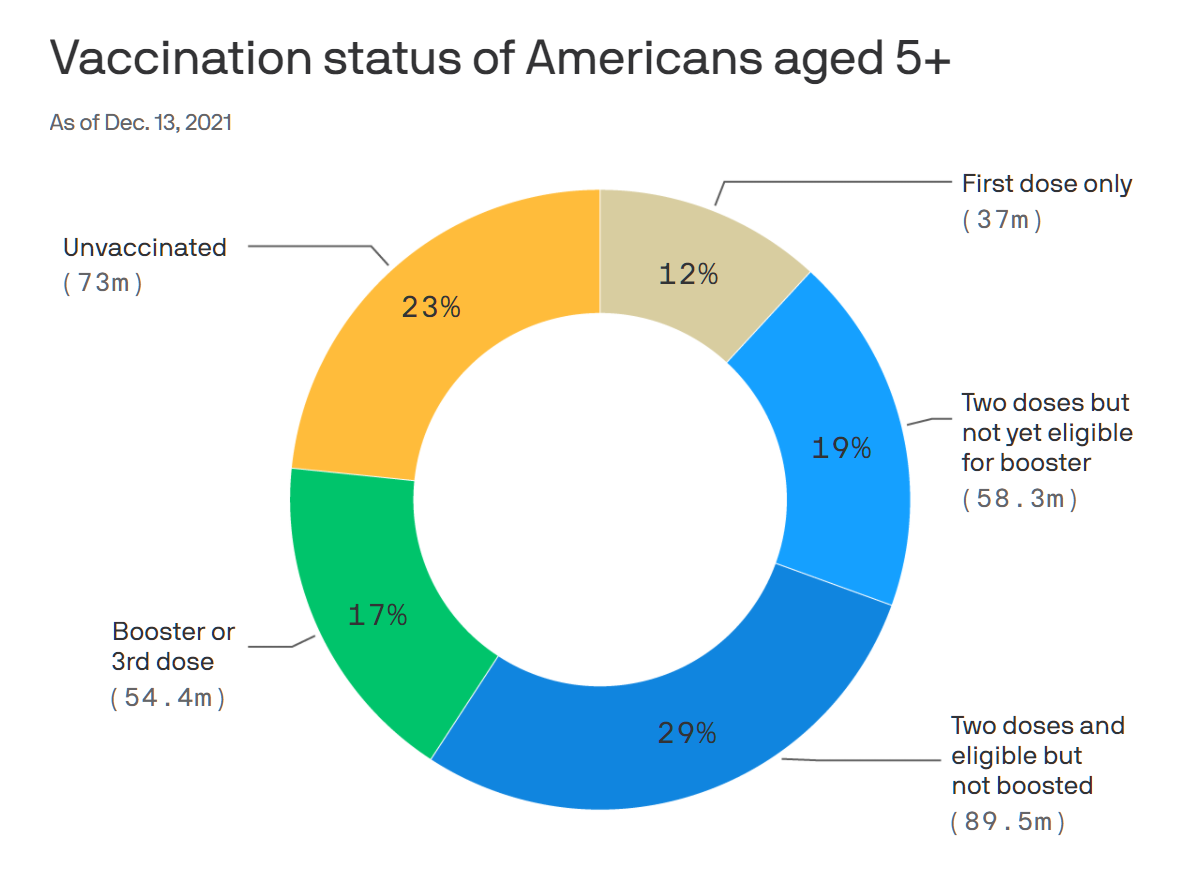
Look at the suffering reflected in the chart below. Fully 58 million of our brothers, sisters, and binary-resisters have had two vaccine shots, but are not eligible for the emergency use authorized sacrament of boosting.
The Axios article quotes someone who seems unsuited to leadership in the American public health priesthood:
“The question is, what is the goal of this vaccine?” said Paul Offit, director of the Vaccine Education Center at Children’s Hospital of Philadelphia.
We were invited to a birthday party for one of the kids in the neighborhood. A slender mom who appeared to be in her early thirties, on finding that we had moved from Massachusetts, said. “I have a close friend up there, but I haven’t been able to visit because she is afraid to be around anyone who is unvaccinated, even though I had Covid back in August.” It turned out that her Covid encounter was similar to what other unvaccinated friends experienced in 2020. She had a low fever, took a nap each day for a few hours, and had some body aches. Per standard, she tested negative several times before testing positive. Why hadn’t she been previously vaccinated? “Covid is not that big a deal and I didn’t trust that the immunity from the vaccine would be good enough or last long enough to be worth the risk of taking a new medicine.” She was not against older people choosing to get Covid vaccine shots, but she was against the government requiring it. #NotHerFrontDoor:
What was the anti-science Deplorable’s job? Nurse practitioner. Some Democrats explain the tendency of married women to vote Republican as due to brainwashing by husbands. Following the same logic, maybe a science-ignorant husband had controlled her mind? I asked about her husband’s job. “He’s an E-R physician,” she responded. “He got one shot and then decided it was mostly hype and never got the second one. I think all of us [in the family] have already had Covid at some point in the last two years.”
It turned out that the father of the birthday girl was a internal medicine doc and therefore more than half of the adults attending were doctors or nurses, all under age 50. Nearly all turned out to be anti-mask, anti-lockdown, anti-school closure, and anti-forced vaccination. They wanted to save lives, and in fact for most of them that was their day job, but they did not believe that salvation from SARS-CoV-2 infection was achievable via public health orders. (I.e., they might have been willing to fight a war against Covid if they believed that a war was winnable.)
None mentioned Donald Trump or any other political figure, so I don’t think that their Deplorable attitude toward Saint Fauci and the lockdowns, masks, and vaccines is driven by politics. In fact, the young nurse practitioner said, in response to my description of our old neighborhood with the political and social justice sign forest in front of most houses, “I have no interest in politics and these remote issues. I think about our kids, our jobs, and our friends.”
Separately, one attendee was from Martinique (an athletic coach, not a doctor). He talked about how the French government imposed the same rules on Martinique that apply back in France. “They’re supposed to check your vaccine passport and exclude you from a restaurant if you don’t have it,” he said, “but everyone in Martinique knows everyone. Are you going to exclude your brother-in-law from your restaurant? It never made sense because almost everything in Martinique is outdoors. They sent the military police in from France to enforce the rules. It is not a good place to be right now.” (see “France sends police reinforcements to Martinique to quell Covid unrest” from December 1)
Finally, what is the current #Science on immunity via infection versus immunity from vaccines? I personally know at least one person who became seriously ill with Covid 5.5 months into his Moderna protection period. I don’t know anyone who got Covid twice, though. And I haven’t read about people returning to the hospital for treatment of severe Covid 6 or 12 months after their first bad Covid experience. I asked some doctor friends “Do people get welcomed back to the ICU with a second case of Covid and doctors tell them ‘Here’s your old bed and ventilator”?” The answer was that it is vanishingly rare and essentially only the immunocompromised who have gotten Covid more than once.
Immunity from natural infection starts to decline after 6 to 8 months. We know that fully vaccinated people still have good immunity after a year—and probably longer.
(Just as 14 days to flatten the curve may take several years, good immunity for longer than a year runs out in 4-5 months.)
SARS-CoV-2-naïve vaccinees had a 13.06-fold (95% CI, 8.08 to 21.11) increased risk for breakthrough infection with the Delta variant compared to those previously infected, … This study demonstrated that natural immunity confers longer lasting and stronger protection against infection, symptomatic disease and hospitalization caused by the Delta variant of SARS-CoV-2, compared to the BNT162b2 two-dose vaccine-induced immunity.
In the U.S., in other words, #Science says that the vaccines are way better. In Israel, #Science says that natural infection is much better (previous infection results in 1/13th the reinfection rate compared to those who got vaccines).
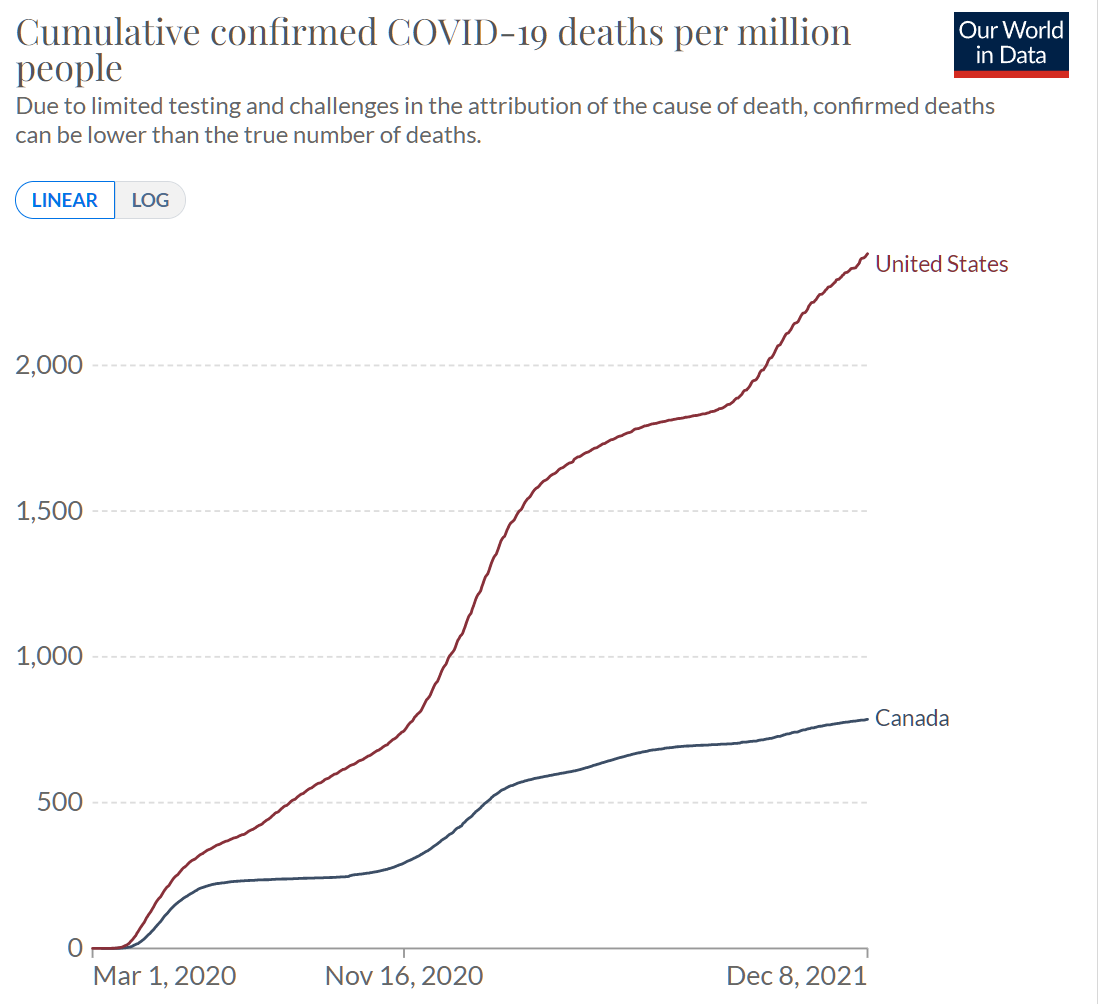
Canadian life and health insurers paid $154 million last year in individual and group life insurance claims from deaths related to Covid-19, an industry group says.
The latest statistics published on Tuesday by the Canadian Life and Health Insurance Association (CLHIA) include details about benefit payouts related to the pandemic, as well as premium growth in life insurance and annuities.
An additional $150 million in disability claims was paid in 2020 above projections to support recovering workers.
Overall, the insurers paid $14.3 billion in life insurance benefits in 2020, $36.6 billion in health insurance benefits, and $46.2 billion in retirement benefits, the report said.
What about the overall increase in payouts in Canada? The same publication says that 2019 payments were $12.1 billion. That’s an 18 percent increase and, therefore, payouts went up by 17 percent for non-Covid reasons in 2020. Perhaps simply due to a big sales push 40 or 50 years ago?
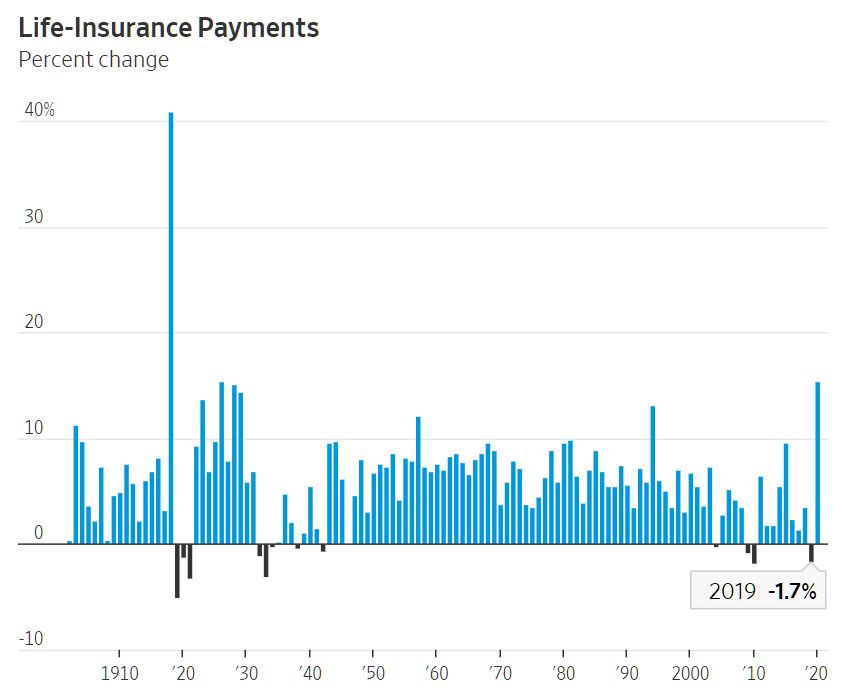
Death-benefit payments rose 15.4% in 2020 to $90.43 billion, mostly due to the pandemic, according to the American Council of Life Insurers. In 1918, payments surged 41%.
If we dig a little deeper, the article shows us year-to-year percentage changes. What happened in previous “surge years”? In 2015, payouts were up by 9.5%. In 1994, they were up by 13.1%. What was the great wave of death that swept the U.S. in 1994?
It looks as though 2019 was an unusually great year for life insurance companies (except those that sell a lot of annuities!). Payouts went down 1.7% despite population growth.
If we believe the Canadian data, adjusted for America’s higher Covid-tagged death rate, only about 2.5% percent of the 15.4% bump can be due to Covid. That would leave us with about 13% as the non-Covid increase, similar to the 1994 surge, and less than the 17% non-Covid increase that was experienced by Canadian life insurers.
As the Delta variant fuels hospitalizations in the U.S., health care systems struggle.
Health officials may be bracing for the Omicron variant to sweep through the country, but the Delta variant remains the more imminent threat as it continues to drive an increase in hospitalizations.
Health care workers said their situations had been worsened by staff shortages brought on by burnout, illnesses and resistance to vaccine mandates.
More than 55,000 coronavirus patients are hospitalized nationwide, far fewer than in September, but an increase of more than 15 percent over the past two weeks, according to a New York Times analysis. The United States is averaging about 121,300 coronavirus cases a day, an increase of about 27 percent from two weeks ago, and reported deaths are up 12 percent, to an average of about 1,275 per day.
Americans pay nearly 20 percent of GDP into the health care industry. 1 out of every 6055 Americans is hospitalized with/from Covid. That’s 0.017 percent of us. Nobody liked my April 2020 idea of building strip mall Covid care clinics like renal dialysis centers. Nobody likes the proven-to-work idea of home care for medium-sick Covid patients (NYT). So we’re apparently stuck with the model that everyone who needs supplemental oxygen will get it in a hospital bed (of which we have about 920,000). The NYT informs us that we don’t have enough capacity after paying 20 percent of GDP to the health care industry. So that leads to today’s question: how much would we have to pay in order to fund sufficient capacity?
(A friend is a business executive at a VA hospital. He said that the VA system set up some high-capacity Covid wards with appropriate ventilation systems to protect the rest of the hospital (filtering the exhaust air, unlike at private hospitals that dump Covid aerosols out into the environment!). He said that private hospitals won’t do this because Covid surges don’t happen often enough and therefore, profitable though it might be to treat an actual Covid patients, it wouldn’t be profitable to set up a big section that is usually idle.)
Note that Florida is edging out of the safe zone, according to CovidActNow. But, on the other hand, hardly anyone cares enough to talk about Covid, masks, vaccines, etc. From Marco Island, yesterday: