“Amy Coney Barrett meets Donald Trump’s two main litmus tests: She has made clear she would invalidate the A.C.A. and take health care away from millions of people and undermine a woman’s reproductive freedom,” said Nan Aron, the president of Alliance for Justice, a liberal group.
Judge Barrett and her husband, Jesse Barrett, a former federal prosecutor who is now in private practice, have seven children, all under 20, including two adopted from Haiti and a young son with Down syndrome, whom she would carry downstairs by piggyback in the morning. Judge Barrett is known for volunteering at her children’s grade school, and at age 48, she would be the youngest justice on the bench, poised to shape a generation of American law.
So she’s kind of busy. Does that stop her from working out?
Judge Barrett and other university faculty members have been known to work out together at a CrossFit-type program, sometimes with their former provost.
Seven children and a job as a Federal judge do not stop Amy Coney Barrett from going to the gym. What is stopping the rest of us?
Strolling by the smokers’ ghetto outside one of our local airport’s FBOs made me wonder when it will be time to abandon our fanaticism regarding the occasional whiff of tobacco smoke. We are certain that any of our fellow humans may kill us with a breath of coronavirus. Why do we worry about the unpleasantness of someone smoking a cigarette 5′ from an exterior door versus 20′? Do we still need Mini-Mike Bloomberg’s 2011 ban on smoking in various outdoor places, such as beaches and parks?
Do we have the energy to fight the anti-smoking battle at the same time as the anti-coronaplague battle? When do we admit that we’re not as capable as Adolph Hitler and his loyal Germans and even they had trouble fighting on multiple fronts?
I’m not a smoker, but I’m now ready to welcome my smoking brothers/sisters/binary resisters with a hearty “You could be exhaling a lot worse!”
I’ve been in a bunch of masked-up environments recently. People have their masks off to take a sip of a beverage or a bite of a sandwich. What would happen if someone took off the mask in order to sneeze and wipe his/her/zer/their nose? Pandemonium, panic, and violence?
One of the things that I have learned in meetings with a big health insurance company whose claims data we use in the classroom: emergency room (“ED”) visits are expensive. A long wait followed by a temperature and pulse ox test then advice to take two Tylenols will cost the employer who sponsors a health plan at least $1,000.
One idea that I came up with around a conference table with the insurance folks was to put a doctor and nurse in a motorhome crammed with all of the stuff that one would typically find in a primary care clinic. Tell folks enrolled in the plan “You can go to the hospital and wait two hours to be seen and pay a $125 co-pay. Or you can stay comfortably at home and the doctor will be there in four hours.”
This is plainly a bad idea because it is obvious and yet no insurance company is doing it. Maybe it is bad because the U.S. is so short of physicians that it is intolerably inefficient to have the physician idle when driving from one house to another. France has a lot of doctors per capita and they do still make house calls (see this 2009 article).
Perhaps the idea is a little less bad in the Covid-19 age. Do we want people congregating in hospital waiting areas now that we can be pretty sure that at least one of the waiting patients is plagued? If the patients are seen at home, at least there is no patient-to-patient contact/transmission.
We already have the technology and skills to build the motorhome-based clinics. Matthews Specialty Vehicles seems to have built a bunch, for example. Odulair in Wyoming has everything up to mobile CT and mobile MRI (these are perhaps overengineered for checking on a person who has flu-like symptoms). Laboit says that they can fit a primary care clinic with a single exam room into a 28 ft. Class C RV:
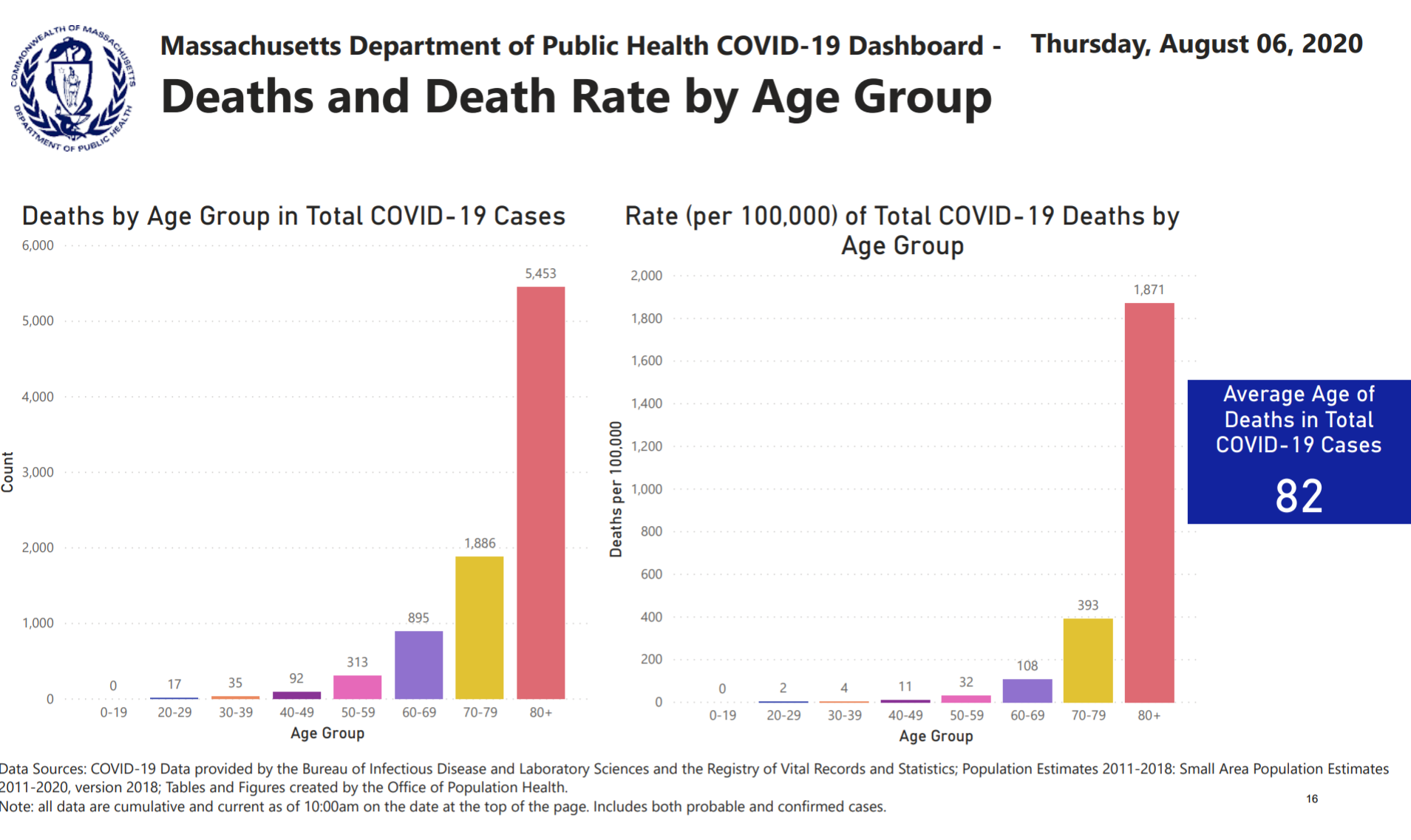
I spent some time recently with two Harvard undergraduates who are camped out in a Cambridge apartment. I’m the oldest person that they’ll have any contact with for the foreseeable future, yet these 20-year-olds behave as though they either worked or lived in a nursing home for 90-year-olds. Asked why they put so much effort into mask-wearing and deny themselves so many social opportunities that they would previous have jumped at, they say that they are personally afraid of getting coronavirus. They’re not obese or chronically ill, so their statistical risk of being felled by Covid-19 is low (see
from mass.gov, statistics that have now been removed), but they seem to perceive Covid-19 as the main risk to their lives and health. They won’t take off their masks, for example, even when outside in mostly-deserted Cambridge. After talking to and observing them, I concluded that, at least for young Americans, Covid-19 is now primarily a disease of the mind. Support for my theory: “We’ve Hit a Pandemic Wall” (NYT, August 5)?
New data show that Americans are suffering from record levels of mental distress.
Let’s start with the numbers. According to the National Center for Health Statistics, roughly one in 12 American adults reported symptoms of an anxiety disorder at this time last year; now it’s more than one in three. Last week, the Kaiser Family Foundation released a tracking poll showing that for the first time, a majority of American adults — 53 percent — believes that the pandemic is taking a toll on their mental health.
This number climbs to 68 percent if you look solely at African-Americans. The disproportionate toll the pandemic has taken on Black lives and livelihoods — made possible by centuries of structural disparities, compounded by the corrosive psychological effect of everyday racism — is appearing, starkly, in our mental health data.
Turns out the extra ten extra pounds around my middle have moved in and unpacked, though I’d initially hoped they were on a month-to-month lease.
The newspaper that has been cheerleading for Shutdown now is surprised that there are some negative consequences? How did the coastal elites not figure out that not everyone’s shutdown experience would be positive? A friend in the Boston suburbs, who was a work-from-home consultant long before the Age of Shutdown, was telling me that his 8th grader hadn’t minded being at home for three months with minimal instruction being provided by the lavishly funded public school. Therefore, he concluded, shutdown was not a big deal, and if the school shutdown lasted another year that was okay too. His son would do fine practicing on the grand piano, learning from Ph.D. Dad and super smart stay-at-home Mom, etc.
I pointed out that not every American child lived in a 6,000 square foot $2 million house with two biological parents who get along at least reasonably well. Would he acknowledge that an inner-city child crammed into a two-bedroom public housing unit with mom, a step-sibling, and mom’s latest boyfriend might have a less favorable view of school shutdown? (he did!)
This is like the Twin Towers imploding all over again – except this time, one story collapses each day, and there is no ground floor.
The pandemic in and of itself is stressful but then add the stress of Trump’s daily tweets. The thought that he might get re-elected makes the stress almost unbearable.
What I think has caused the national stress-out, Ms. Senior, is that America now knows that it’s on its own. We don’t have a president who actually understands and cares about us.
I stress over the corrupt Republican leadership, so unconcerned for 99.9% of Americans that they let a a spoiled child throw our health, education, and welfare out the window, …
A coworker yesterday confided that about 15 of her relatives are COVID positive after a big family graduation party 10 days ago. I couldn’t hide my disgust. She is a very highly paid executive. We work for a research university health system!!! My neighbors just had a 40-person party for their 9-year-old. And seemed miffed and befuddled that many of us on the block declined to attend. They were all crammed under a tent shoulder to shoulder. Nary a mask in sight.
Maria from Maryland: The thing is, a lot of us are coming to the conclusion that all our problems are the same problem. Botched coronavirus response? Republicans. Insisting on doing things that spread the disease? Same. Economic deprivation? Republicans again. Two generations of failing to address racial issues? Again. Two generations of banging our heads against the same gender barriers? You guessed it. Failure to deal with climate change? Do you need to ask? Guns? Infrastructure? Science? Arts? They’ve been at it my whole adults life, ruining everything. And at their apex, they produced the very worst man in the world. There will be a vaccine for the virus, but what about the humans who are ruining our lives?
Coronaplague wouldn’t bother them at all, apparently, if Joe Biden were the Great Father in Washington right now!
Coronaplague obviously is a real problem for the elderly/vulnerable. And in societies where it is allowed to run wild, e.g., Sweden, it will kill approximately 0.05 percent of the population within a few painful months. But will readers agree with me that if young people are afraid of getting the disease personally, despite having no actual or planned contact with the old/vulnerable, then coronavirus has mutated into something whose main effect is mental illness?
If you want to know how much profit there is in the non-profit world… a friend who works at Partners told me that the enterprise will be spending more than $100 million to rebrand back to what is essentially their old names: “Mass General Brigham” (combination of Massachusetts General Hospital, a.k.a., “the Massive Genital”, and Brigham and Women’s Hospital). That’s confirmed by this article.
I had to take a class yesterday on “Racial and Community Violence” in order to renew my license to practice. There were only three articles used as curric[ulum].
(1) The first was regarding the mystery of why ordinary Americans support Trump. It said among other things, “Trump is an insult clown….and he is “A gold-plated buffoon who draws the enthusiastic endorsement of racists across the spectrum of intolerance, a gorgeous mosaic of haters, each of them quivering excitedly at the prospect of keeping a real, honest-to-god bigot in the White House. The Trump movement is a one-note phenomenon, a vast surge of race-hate. Its partisans are not only incomprehensible, they are not really worth comprehending.” (maybe from The Guardian?)
The second article was titled “Ferguson Isn’t about Black Rage Against Cops. It’s About White Rage Against Progress.” (Washington Post?)
The last article was titled, “The Decline and Fall of White America: Inside the Study that Shocked the Public-Health Community” (Slate?)
I got my CEUs [continuing education units?]. The class was produced and offered by The American Psychological Association. I paid them $80 for it. It is 3 hours to meet my multicultural requirement.
In September 2009, I wrote “Health Care Reform”. Essentially the government would take the $trillions being spent on Medicare and Medicaid and put it into buying every American a reasonably good HMO policy.
each resident will be given a voucher good for signing up at the clinic or HMO of his or her choice; the amount of the voucher will depend on the resident’s age and sex (the weighted average of all vouchers will equal $2,000 or whatever we’ve decided we want to spend)
a clinic or HMO that wishes to get any revenue from the federal government will be required to take any person who submits a voucher, regardless of preexisting conditions
a resident of the U.S. can switch clinics annually, let’s say on May 1.
the clinic is responsible to pay for the resident’s emergency medical care at another facility
A note:
One likely side effect of this reform is the return to centrality of the primary care physician. Joe Medicare Patient often does not have any doctor who understands much less coordinates his care. If Joe has seen six specialists, he may be on drugs that are working at cross purposes. If Joe is in the ICU at a typical hospital, the multiple doctors treating him may never talk to each other. Each one knows what tests and procedures he or she has ordered, but, except by looking at the patient’s chart, has no idea what the other doctors are investigating. One primary care doctor who reviewed this proposal said “The first item I address with new patients in my office is to try to get them off as many drugs as possible; when a 70-year-old is on 11 meds you better believe there are many unintended interactions.”
How has this aged and what would be different during coronaplague?
Most of all, Trump is the man who doesn’t care. He doesn’t feel your pain. He doesn’t mourn the dead, comfort the grieving, or support the struggling. He doesn’t consider his words or worry that they could have consequences. He doesn’t listen to experts or ponder his options.
Congress is almost finished with its “work” for this session. If the Republicans want to win in November, why not make Americans feel that the they are loved and cared for? We don’t care about money anymore, right? We are happy to spend 100 percent of our accumulated wealth hiding from coronaplague if that is what it takes to cut the death toll slightly. We are happy to print and borrow trillions. A universal HMO policy for every resident of the U.S. wouldn’t have to cost any more than the current bleeding for Medicaid and Medicare plus whatever employers pay for mid-range coverage.
Will anyone, other than folks in the industry, miss the current system? A couple of recent news items:
At least to judge by my Facebook feed, Americans are convinced that, despite the lack of any effective therapy for Covid-19 and despite the fact that the Feds pick up the tab when the uninsured are treated for Covid-19, universal health insurance would hugely cut the number of Covid-19 deaths.
Readers: What do you think? Could Trump and the Republicans take most of the wind out of the Democrats’ sails with one big health care hand-out? (of course, all of the money for this would just come from taxpayers themselves, but somehow Americans never seem to consider that they will ultimately have to work for whatever the government “gives’ them)
Bonus pictures of the house that Medicaid and Medicare built, in Nome, Alaska, from September 2019. This single building is likely worth more than all of the rest of the houses and commercial real estate in the city.
In the first 10 days after the World Health Organization’s March 11 declaration that COVID-19 was officially a global pandemic, smartphone users worldwide showed a 5.5% decrease in mean daily steps (287 fewer steps).
In the first 30 days, mean daily steps dropped 27.3% (1,432 fewer steps), reported the group led by Geoffrey Tison, MD, MPH, of the University of California San Francisco. Their paper was published online in the Annals of Internal Medicine.
For example, people in Italy had a 48.7% maximal decrease in daily steps, whereas those in Sweden showed only a 6.9% maximal reduction in steps. The difference may have stemmed from government responses, as Italy issued a lockdown on March 9, whereas Sweden has yet to implement such a measure.
(I like the last part. There is still hope among the righteous for saving Swedish souls by converting them to the Church of Shutdown.)
“This is an interesting natural experiment that has health implications for global and regional populations, and especially those with underlying chronic health conditions who are particularly vulnerable to COVID-19-related morbidity and mortality and who may depend on routine physical activity as a preventive measure,” according to Messiah.
i.e., it will be interesting for a “scientist” (named “Messiah”! As someone who evaluates coronaplague “science” from a comparative religion point of view, this is my dream fulfilled!) to watch fat people die.
From the Newport Jazz Festival, 2005 (canceled until a hardier breed of Americans can be produced?):
The author of Medical School 2020 said that he was going to be taking “bystander training.” I responded with “So you’ll know what to do if you see a car accident, like Tom Cruise?” It turned out to be something different:
We are excited to bring Bystander Training to [the school]. This program was built by [a person with a female-typical first name and degrees in psychology and women’s studies] and designed to train citizens to safely intercede when they see another individual at risk of sexual harassment and/or sexual assault. This evidence-based program is regarded highly as one avenue through which sexual harassment and sexual assault can be successful combatted.
This training will prove helpful not only in your interpersonal interactions privately, but also in your interpersonal interactions professionally. Unfortunately, sexual harassment and sexual assault are found in every setting. Learning how to navigate extremely challenging moments in time can prove invaluable to everyone involved.
This training is required for all M1, M2, and M3 students.
[signature from an administrator with a female-typical first name]