How is the wage-price spiral going?
The smartest people in the U.S. say that a wage-price spiral cannot occur. “Giving Workers a Raise Is Not Going to Make Inflation Worse” (New York Times, October 2):
At the moment, wages are rising faster than inflation, which means that “real,” or inflation-adjusted wages, are rising.
“There is almost no evidence” that wage increases lead to inflation, Rosenberg wrote. His firm conducted a statistical test (called Granger causality) that found inflation causes wage increases, but not the other way around. He predicted that rather than passing along higher wage costs to customers, companies would be forced to swallow them and accept lower profits.
In other words, the Science of Rosenberg and Granger proves that cars and bicycles sell for the same amount because higher costs for producers don’t shift the supply curve and change the equilibrium price.
Here’s the latest from our local schools:
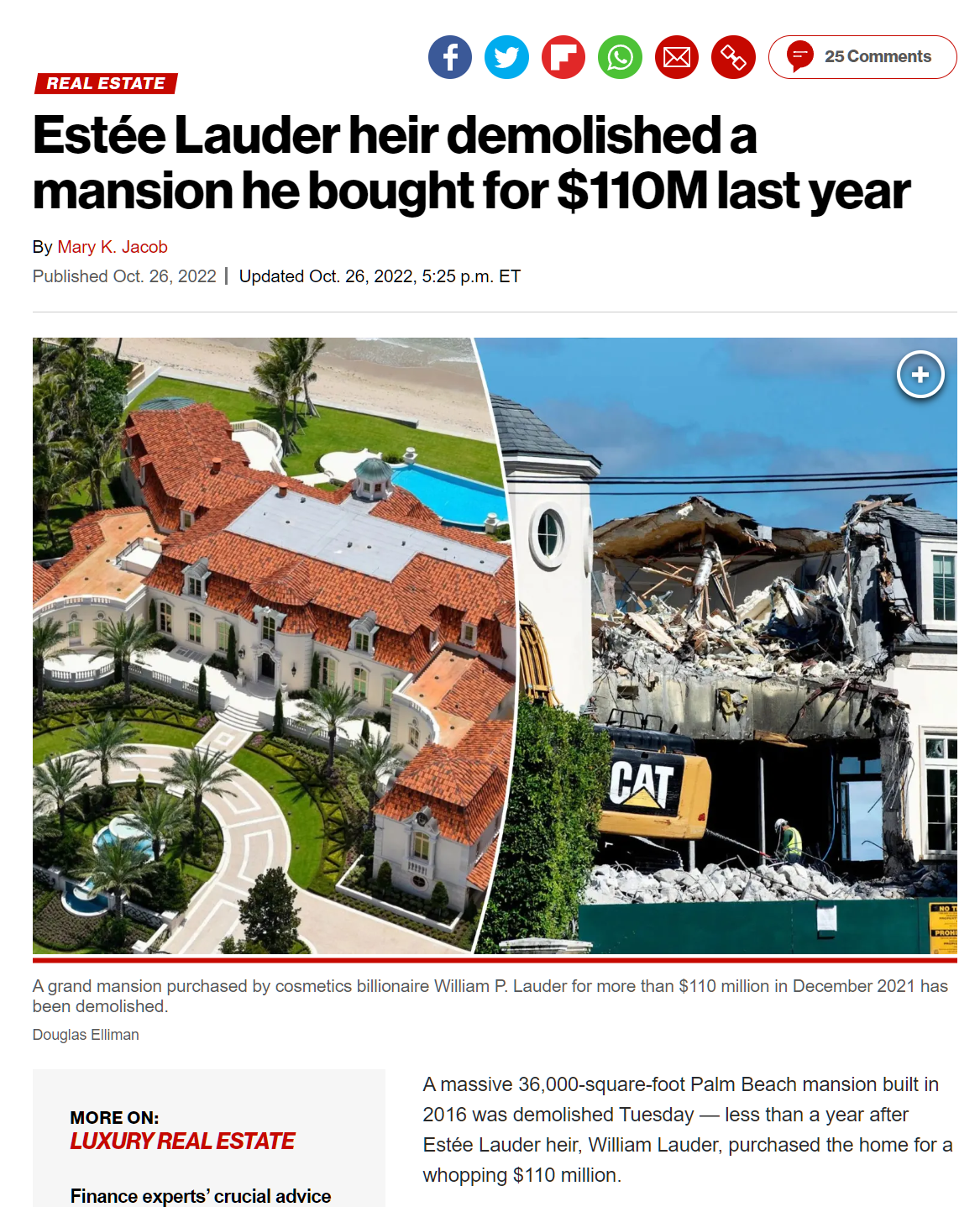
The School District of Palm Beach County reached an agreement with the Palm Beach County Classroom Teachers Association (CTA) that will give an average 7% pay increase and one-time 3% bonus to instructional employees. The agreement was approved by the School Board during its Special Meeting on October 4, 2023. The significant raise demonstrates the District’s commitment to fairly compensating teachers for their hard work and dedication to students.
There is no possibility of the price of property tax going up to pay for this, according to the New York Times.
September 2023: Hollywood agrees on a new, higher-paying, contract with writers; “an 18 percent pay bump and a 26 percent increase in the base rate with which residual payments are calculated” (Washington Post)
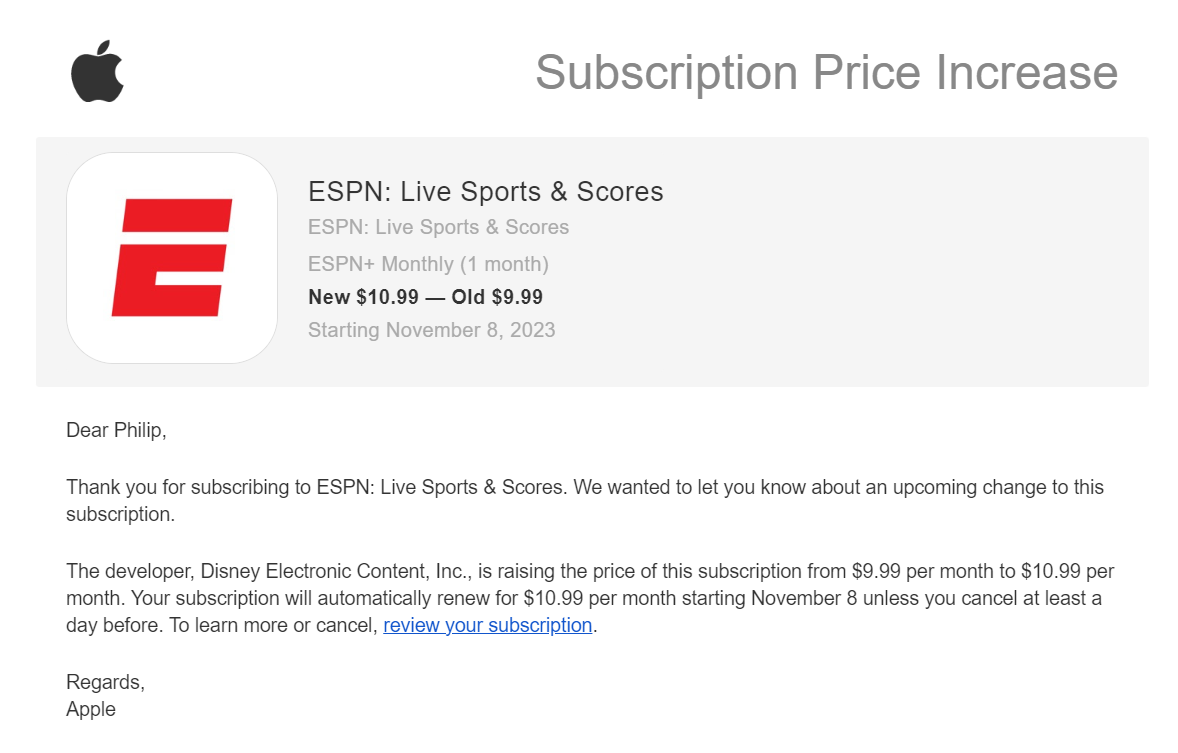
October 2023: “Streaming services keep getting more expensive: all the latest price increases” (The Verge).
Received October 10, 2023, regarding the supply for our 10-year-old crack addict:
Also from October: “Ford Already Covering UAW Wage Increases With Huge 2024 F-150 Price Hikes”.
July 2023: “Disneyland Workers Could Get Nearly $20 an Hour Following Appeals Court Ruling”.
October 2023: “On the most popular days, though, Disneyland is raising prices by more than 8% to $194. For a five-day ticket, Disneyland raised prices by nearly 16% to $480. The park also raised the price of various add-ons. Disneyland’s Genie+ product, which gives customers access to shorter lines, will now cost $30 a person, up by $5. For five-day tickets, the price for Park Hopper, which lets customers go between Disneyland and Disney California Adventure Park on the same day, also rose by 25% to $75. Disneyland also raised the price for parking and other products, including its Magic Key annual passes.” (Wall Street Journal)
Readers: What else have you seen that could be considered evidence for my discredited theory that a wage-price spiral could occur?
The good news: if your own income isn’t keeping up with inflation, you can save money by shopping at Costco. On a September 25, 2023 visit, they were offering a bottle of Champagne for $4,500, including a free glass.