On the effectiveness of the Anti-Defamation League
The Anti-Defamation League (ADL) claims expertise in eliminating hatred. When they started, they were experts in getting American haters to love Jews. In their own opinion, at least, they were so good at this that they expanded. Here’s just their civil rights section:
They want to make sure that low-skill Americans have plenty of competition from low-skill immigrants:
ADL fights tirelessly for immigrants and refugees seeking safety and a better life in the U.S. Through legislative advocacy, amicus briefs, and public awareness efforts, we have promoted just and humane immigration and refugee protection policies throughout the decades.
The ADL will make haters realize that #LoveWins:
ADL has long fought in the U.S. and abroad to advance LGBTQ+ equity, encouraging legislation that protects individuals’ rights and providing education resources that make schools, workplaces and communities more welcoming and inclusive.
What have we seen in the past few weeks? Muslim immigrants to the U.S., whose right to settle here was pushed by the ADL, rallying and pointing out that the Islamic Resistance Movement (“Hamas”) is not a terrorist organization, but the Israeli government and all supporters of Israel are (video). Twitter and Facebook jammed with anti-Israel content. A young woman in a hijab in NYC and her friend giving the finger to a billboard truck advocating for the return of hostages held by Hamas (video). Depending on your political point of view, you might agree with these anti-Israel positions, but I think that everyone can agree this is not what the ADL was trying to accomplish.
Maybe the ADL could be more effective with people if they would spend more time soaking up the ADL message? From the New York Post:
One of the NYU students who brazenly ripped down posters of Israeli hostages is an activist “extremely passionate about fighting racial profiling” who blamed her behavior on misplaced anger.
Yazmeen Deyhimi — a junior at the top university who once worked for the Anti-Defamation League — admitted to tearing apart banners that were plastered outside NYU’s Tisch Hall, in a shameless act that was caught on video.
“I have found it increasingly difficult to know my place as a biracial brown woman, especially during these highly volatile times,” she wrote.
According to her LinkedIn profile, Deyhimi is an advocate against Muslim bigotry and spent a summer working with the ADL as a CSC education intern when she was just 15 years old.
“After review, we can confirm that one of the participants was part of an ADL high school level summer internship in 2019,” a spokesperson for the organization told The Post.
The ADL had a whole summer to convince this young person that Jews are lovable!
If the ADL has failed spectacularly at its original mission, at least the Ministry of Truth is working effectively there:
The ADL has since taken down a blog post announcing the Long Island native as one of the 12 student leaders joining the program, describing Deyhimi as “extremely passionate about fighting racial profiling and championing gender equality.”
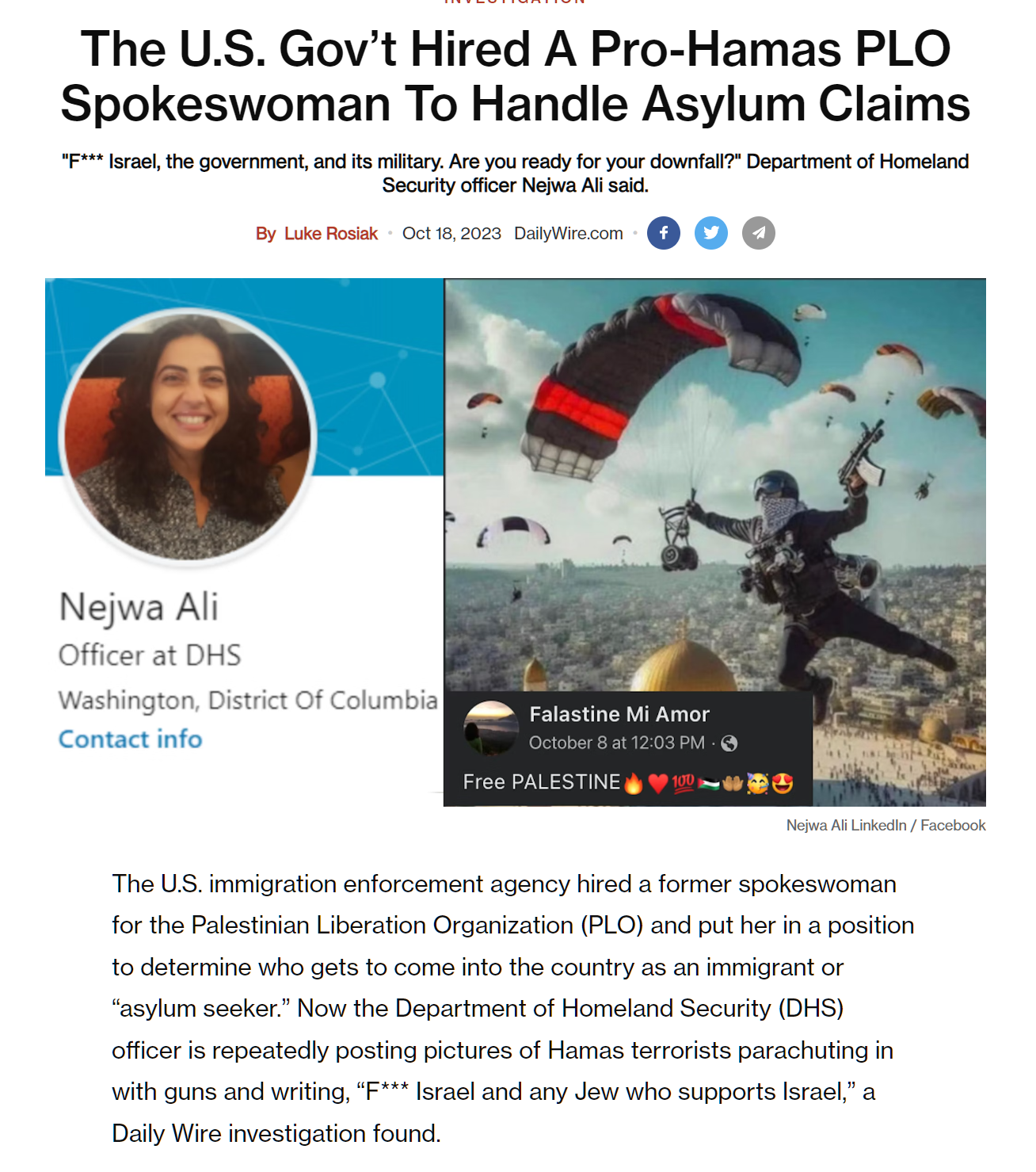
Does supporting Hamas impair a migrant’s claim for asylum in the U.S.? Not according to the Deplorables at the Daily Wire… “The U.S. Gov’t Hired A Pro-Hamas PLO Spokeswoman To Handle Asylum Claims”:
Speaking of Deplorable, what does Ron DeSantis have to say about the ADL’s passions for Islamic immigration and using propaganda to eliminate hatred? From Twitter:
No Gaza refugees, period.
It’s a fools errand to think we can separate a terrorist from a ‘freedom lover’ in Gaza.
Related:
- the College Terror List, which was disappeared by the Ministries of Truth at Google, archive.org, DuckDuckGo, and all of the other righteous folks. This page contains various statements by elite college students who don’t seem to have been reached by the ADL’s message about the wonderfulness of Jews. Harvard: “We … hold the Israeli regime entirely responsible for all unfolding violence”; Stanford: “while Palestinian resistance is legal under international law, Israel’s breathtakingly violent actions are illegal collective punishment under the Geneva Convention”; Swarthmore: “Since early Saturday morning, Palestinians in Gaza and the West Bank have valiantly confronted the imperial apparatus that has constricted their livelihoods…”; George Mason: “Every Palestinian is a civilian even if they hold arms. A settler is an aggressor, a soldier, and an occupier even if they are lounging on our occupied beaches.” (preserved by Ghostarchive; the only way to find it is with the Kagi search engine (see below))