A new COVID-19 vaccination clinic in the Fruitvale neighborhood is offering interpreter services for the Latin Mam or Mayan-speaking community.
This month, La Clinica de La Raza began offering the community-targeted vaccination service at 32 locations across the Bay Area, including ASCEND Elementary School on East 12th Street, where Latinos who speak Mam, K’iche ‘and Q’eqchi’ can get translation help from appointment to inoculation on Thursdays.
The article is illustrated with a photo of a guy who has apparently adapted completely to prevailing American cultural norms (he’s wearing a “WEED; Keep it lit” T-shirt).
Now that the U.S. border is effectively open, especially to those who can credibly claim to be under 18, I wonder if this suggests a good career path for young people: medical interpreter for Mayan and similarly unpopular languages. If folks didn’t learn Spanish when they lived in a predominantly Spanish-speaking nation, why expect them to learn English now that they’re Americans? They’ll be entitled to interpreters whenever they’re taking advantage of public housing, Medicaid, food stamps (SNAP/EBT), etc. At least for some of these jobs, certification is required and therefore immigrants themselves may not be able to perform them (also those immigrants may be undocumented and unable to work a W-2 job at a hospital or clinic).
What do folks think? Is learning an obscure language a good career in what is likely to be a growth industry?
(Also, does “Latinos who speak Mam, K’iche ‘and Q’eqchi’” make sense (leaving aside the issue that it should be “Latinx who speak”)? If a person doesn’t speak any language with Latin or Indo-European roots, is he/she/ze/they “Latino” or “Latinx”?
I’ve long been an advocate for universities shutting down dormitories. Why take responsibility for what 18-22-year-olds do when they’re not in class? Build shared spaces for students to work together, not spaces for students to sleep together, party, etc. This goes double for the Age of Coronapanic. In addition to purporting to be students’ educators, universities have taken it on themselves to become students’ jailers (see College Today: Exercise by going to your twice-weekly COVID-19 test).
A Los Angeles County Superior Court approved a deal Thursday that would give 710 women who alleged that they were abused by Tyndall an $852 million settlement. That is in addition to a $215 million settlement that was given final approval last year as part of a different federal class action lawsuit.
In a letter to students and alumni, the president of the university Carol L. Folt said, “These events have been devastating for our entire community.”
Dr. Folt also said the university would fund the settlement over two years through a combination of “litigation reserves, insurance proceeds, deferred capital spending, sale of nonessential assets, and careful management of nonessential expenses.” She added that no philanthropic gifts, endowment funds or tuition would be redirected to pay the costs.
This makes as much sense as saying “I didn’t use our household funds to pay for that case of booze; I used money that I won from a scratch-off lottery ticket.”
Readers: What is the upside for a university or college in running its own clinic? Given that academic administrators are selected for their skill at harvesting tax dollars (tuition subsidies, student loans, research grants), how could anyone ever have expected them to properly supervise something complex such as health care delivery? If the goal is to have convenient primary care available, wouldn’t it make more sense to offer low-cost leases to unaffiliated providers?
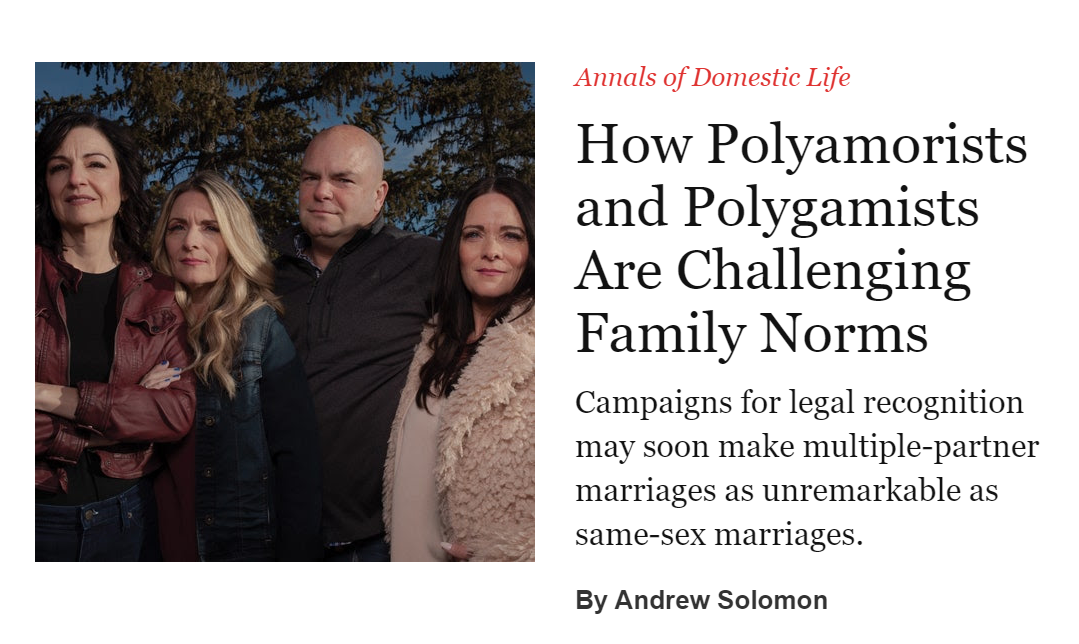
Back when same-sex marriage was the subject of referenda (eventually rendered irrelevant by the Supreme Court), the haters said that same-sex marriage was the camel nose under the tent for polygamy. This was an outrageous calumny. See “Polygamy Is Not Next” (TIME, 2015), for example and “No, Polygamy Isn’t the Next Gay Marriage” (Politico, 2015): “Opposing the legalization of plural marriage should not be my burden, because gay marriage and polygamy are opposites, not equivalents.”
This isn’t news, actually, but we’re just hearing about it now…
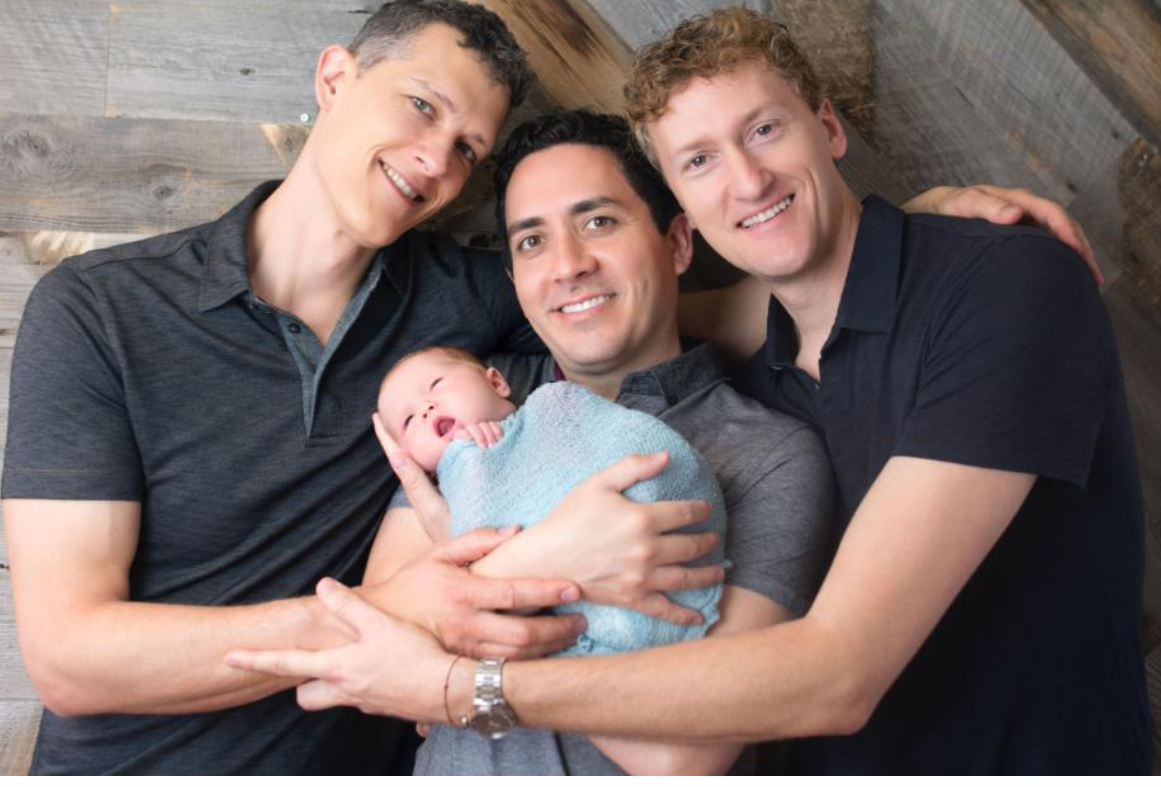
The judge ruled in their favor before their daughter Piper was born in 2017. Jenkins believes they are the first polyamorous family in California, and possibly the country, to be named as the legal parents of a child.
The journalists want us to know how much better this is than when there are two squabbling opposite-sex parents:
The dads and their children share a bustling house with two Goldendoodles named Otis and Hazel.
“We’ve had zero negative feedback from coworkers and friends. Everyone seems to just be delighted about the arrangement and that’s because they know us,” Jenkins says. “I think some people will look at this and say like, ‘Oh, this is exotic. It’s going to harm the child.’ But people who know us know that we have been taking care of these kids as best as we possibly can.”
That however hopeless things may seem as a young gay man struggling to fit in, the world is changing. And that he’ll someday find more love under one roof than he ever imagined.
The next year, in an online forum, they saw a post from a woman in her early thirties named Julie Halcomb that said, “I’m a single mom, I’ve got a two-year-old daughter, and I’d like to learn more.” Rich wrote, “If you want to know more, ask my wives.” Angela had opposed adding a third wife, but when she got off her first call with Julie she said, “O.K., when is she moving in?” Julie visited, mostly to make sure that the kids would get along, and joined the household permanently a week later.
Their living arrangements attracted other unwelcome attention. Neighbors called the police, and Child Protective Services interviewed the children. Since there was only one marriage certificate, the police couldn’t file bigamy charges. “They said, ‘We don’t like it, but there’s nothing we can do,’ ” Julie recalled. “But we had them at our door constantly. One of the kids would have an accident at school—we’d have them there again. They were constantly trying to find signs of abuse.”
At the family’s largest, Rich had four wives, but when I met him, a couple of years ago, he and Angela were divorcing, and another woman, April, had come and gone. Rich, Brandy, and Julie were living with their kids—six, including Rich’s and Julie’s from earlier relationships—and saw Angela’s two every other weekend.
The Austins would like one day to enjoy the legal benefits that married couples take for granted. Brandy and Julie take heart from the success of the gay-marriage movement. “I’ve got a wedding invitation on the way from a friend who’s transitioning from female to male,” Julie said. “I’ve got classmates that came out almost twenty years ago. They’ve been lucky enough to get married. I wish people would be as accepting with us as we try to be of everyone else.”
We already have functional polygamy in the U.S. An American doesn’t need to settle for the highest-earning partner whom he/she/ze/they can find for a long-term marriage. He/she/ze/they can have sex once with an already-married high-income defendant and earn more via child support (see Hunter Biden’s plaintiff) than by getting married to a mediocre earner and enduring his/her/zer/their presence in the apartment 24/7. Soon we can have de jure polygamy?
This is based on a March 2021 trip to Savannah, Georgia.
Residents of and visitors to Savannah are constantly reminded to wear masks and that COVID-19 is likely to kill them. The city hall, festooned with a “MASK UP: Mandatory Mask Order” banner:
The order itself is Maskachusetts-grade in that people are required to wear masks when walking down the sidewalk, even if nobody else is nearby.
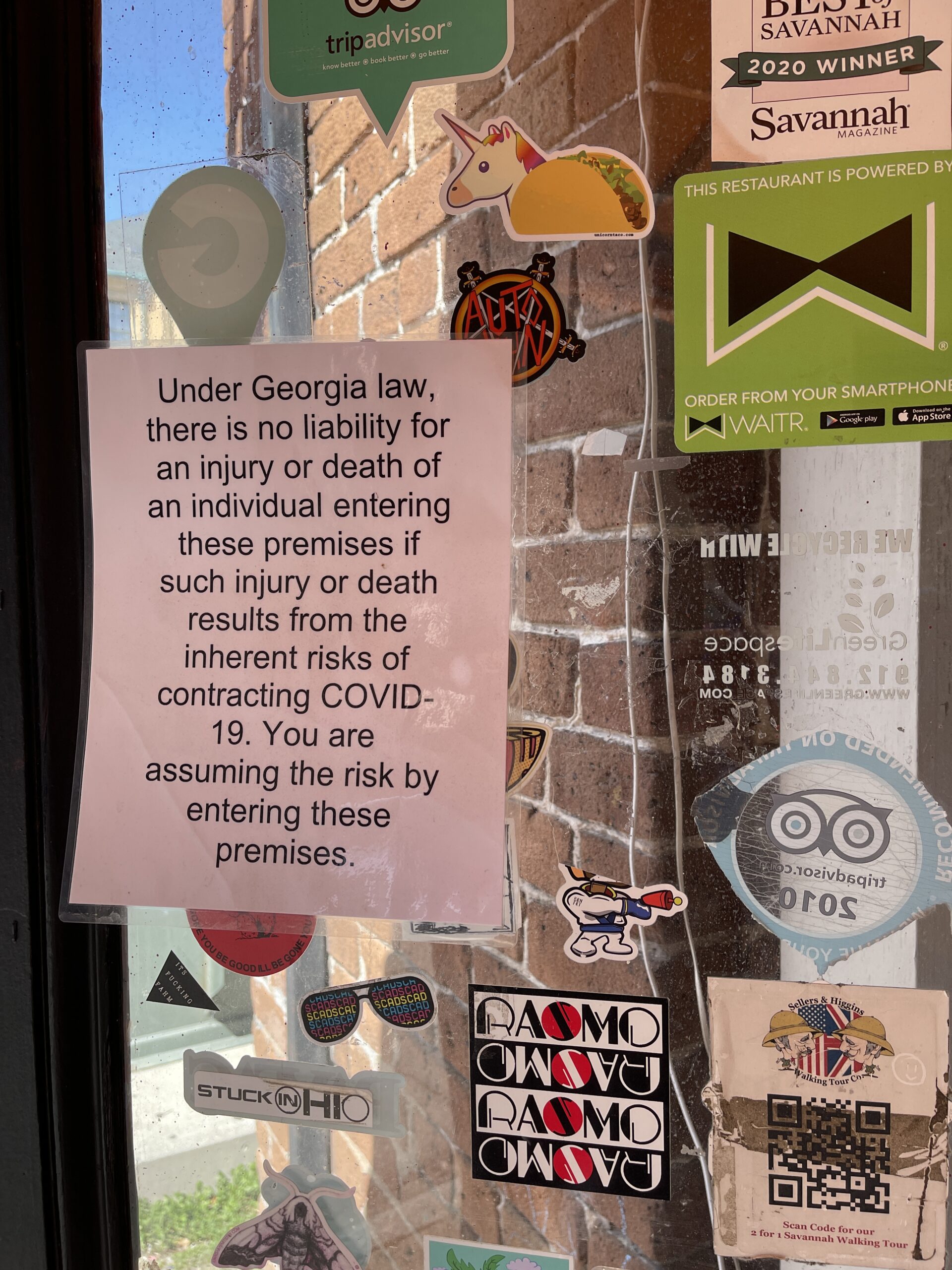
Half the stores and restaurants have a sign on the front door regarding “injury or death … from … COVID-19” and reminding customers of the heroic risks that they’re taking by entering. Example:
(If the law exempts businesses from liability, why do they have to post a sign? Maybe the exemption is operative only if they do post a sign?)
While the private economy shrivels, new government jobs have been created (Savannah schools have been mostly closed during coronapanic, but the paychecks to the teachers and administrators continue to flow). “City of Savannah introduces new COVID-19 resource team”:
25 City Marshals will now be patrolling the streets of Savannah in ATV’s as part of the city’s new COVID resource team.
The main goal of the team is to give out masks and educate both locals and tourists about the current mask mandate in the City of Savannah.
We saw these heroes out and about, but never did they leave the security of their vehicles. (Our exposed-to-coronarisk Uber driver was a recent immigrant from Morocco, but the socially distanced COVID resource team appeared to be drawn from the native-born.)
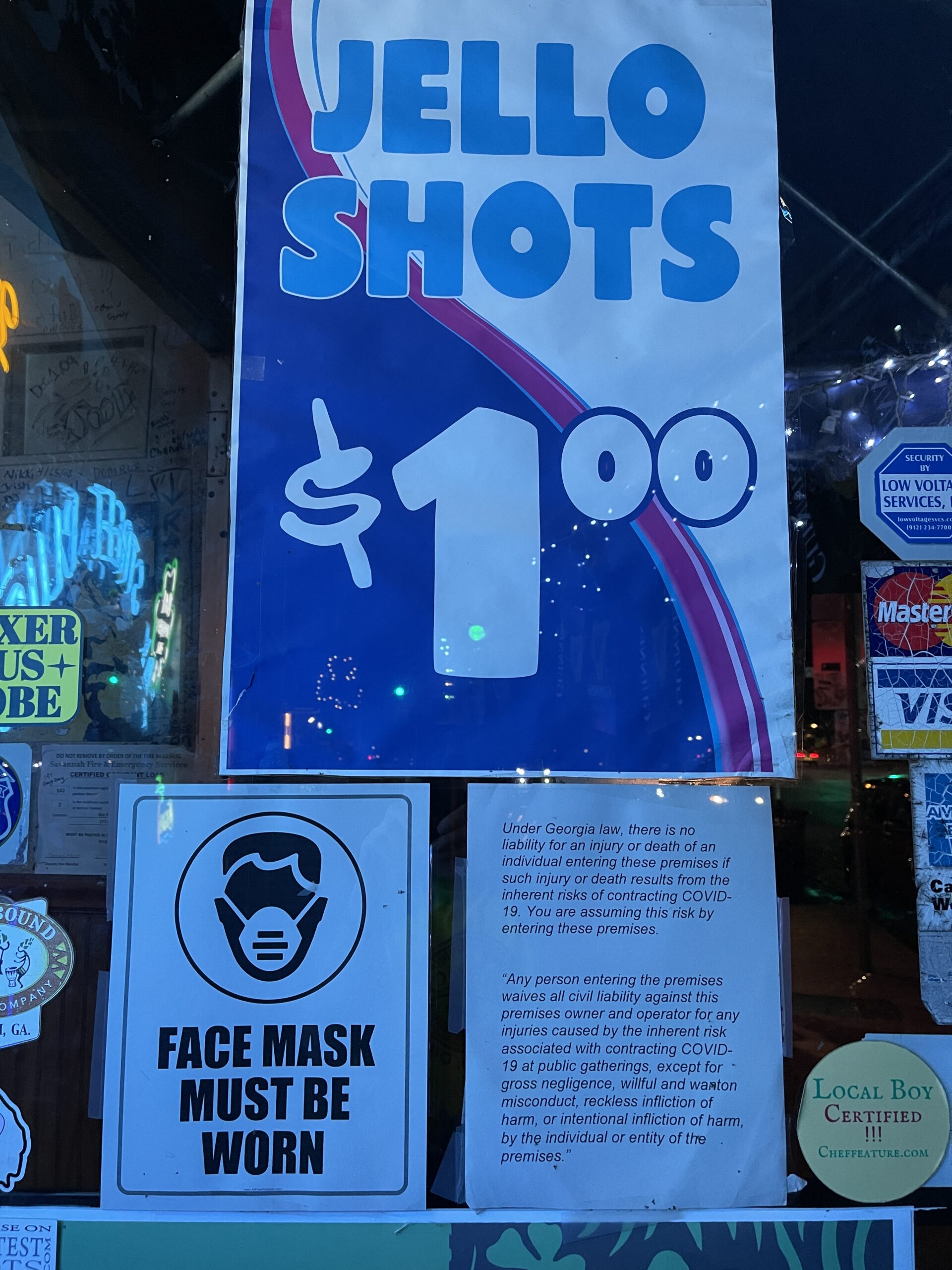
What’s the effect on a population that gets hit by these messages every few minutes and that is placed under a threat of $500 fines for noncompliance? About one third of people out walking were wearing masks. People mingled mask-free into the wee hours in the city’s many bars. I’m not sure if the sign offering $1 Jello shots was honored, but a casual walk-by revealed that the “Face Mask Must Be Worn” sign had no effect on those inside.
Here are some good citizens in front of the Elon Musk statue (“African American Monument”) on a windy sunny day by the river:
Note the range of styles… no mask, chin diaper, full mask. Even if one accepts that, contrary to what W.H.O. scientists said prior to June 2020, masks for the general public have some effect on the transmission of a respiratory virus (see the Czech Republic), it is tough to understand how the Savannah system is supposed to yield a different result than what would be experienced by a society in which government imposed no orders.
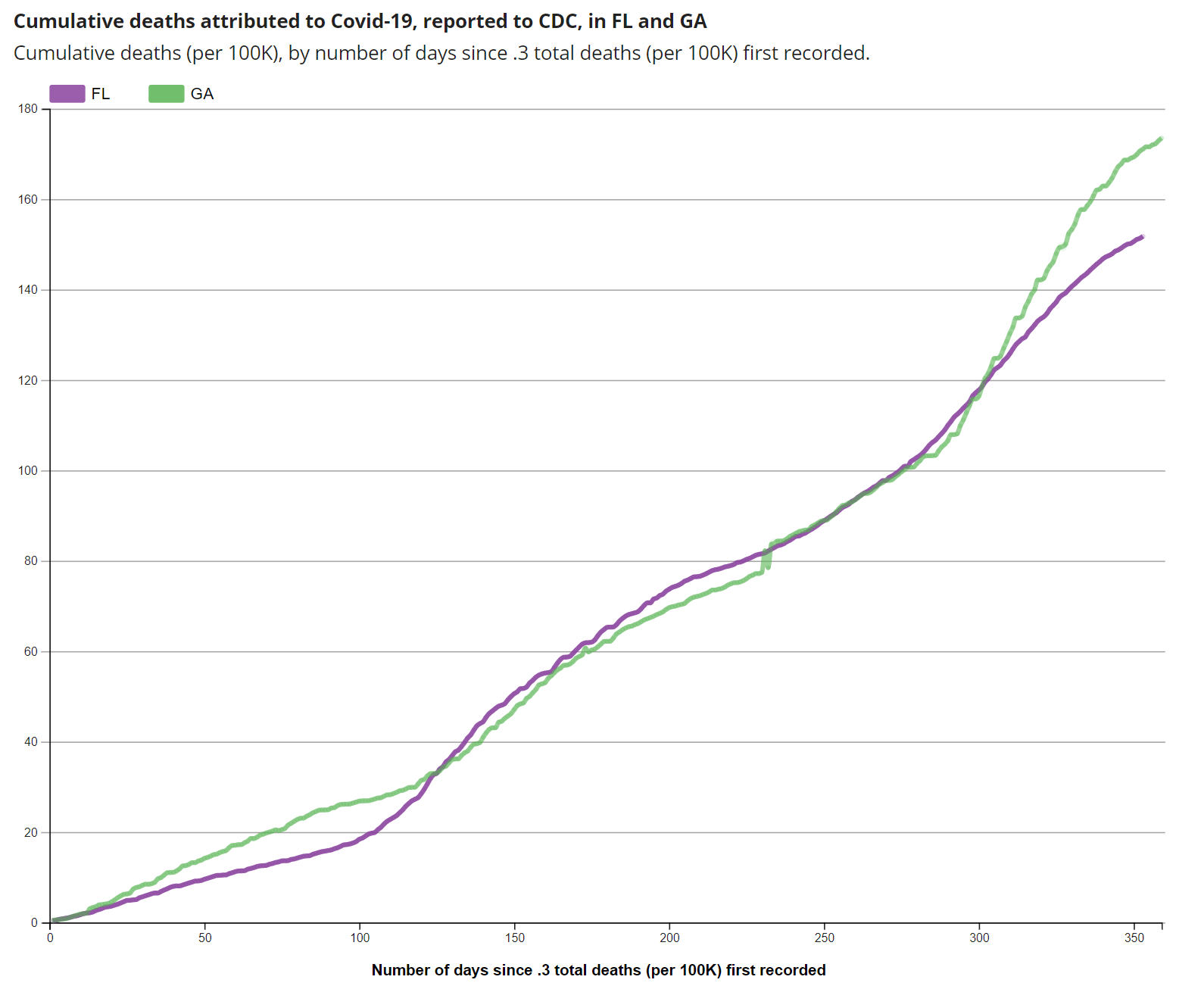
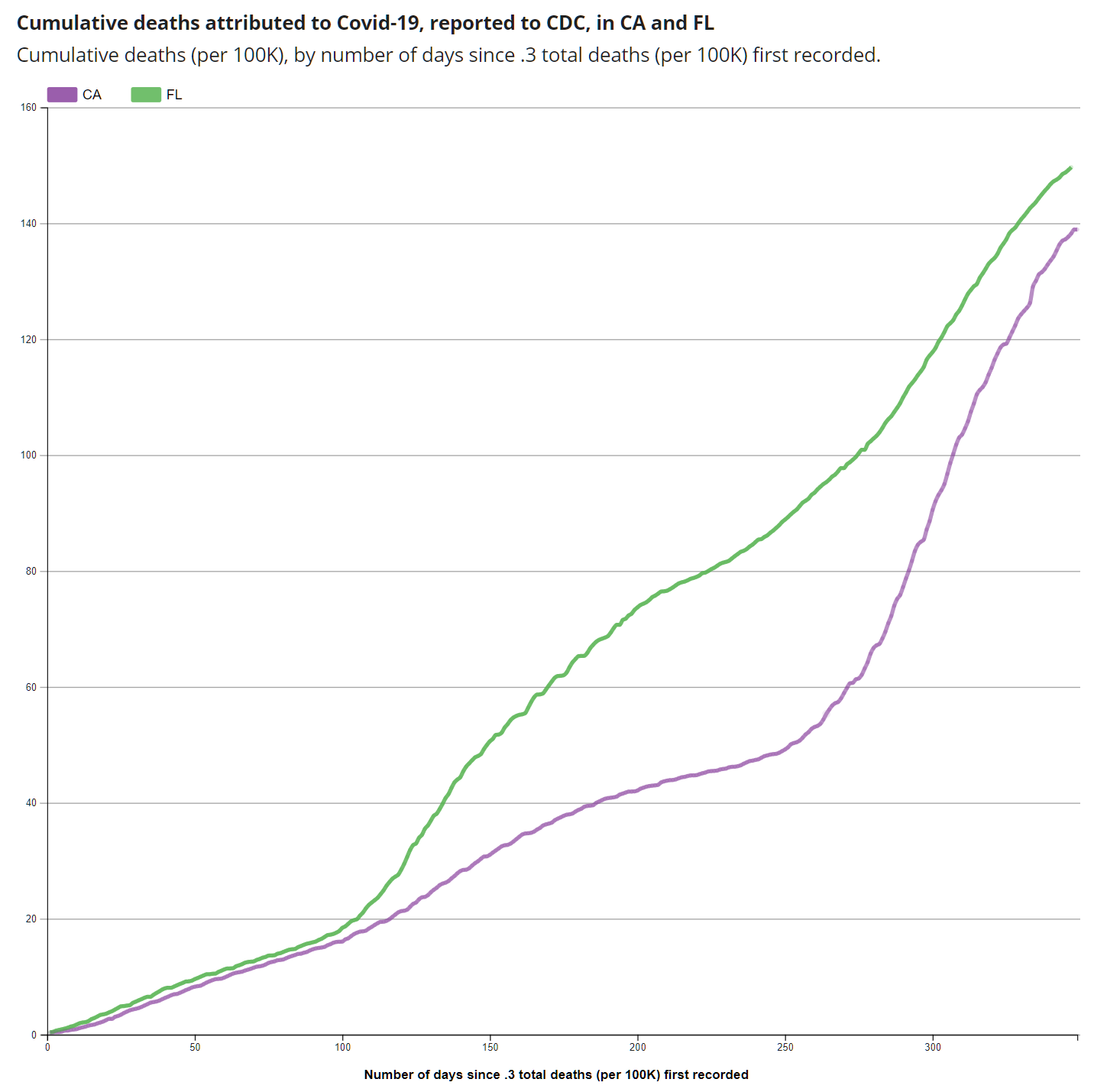
Compared to the mask-free Covidiots in neighboring Florida, how did Georgians do with their muscular interventions by city and county governments? From the CDC:
Meanwhile, let’s have a look at some of the stuff that folks in Savannah were able to build in the good old pre-COVID days (when yellow fever and malaria raged). A church with no BLM banner or rainbow flag (I’m convinced that Christianity is a completely different religion in Massachusetts vs. in Florida or Georgia!):
A ride from an unmasked horse:
A COVID-themed statue, “Come from the Four Winds, O Breath, and Breathe Upon These Slain That They May Live”:
The swan here does not seem to lack for breath:
Most of the famous squares seem to be themed around the American Revolution (i.e., the Rebellion of the Traitors), but here’s a problematic one, named after states’ rights and slavery advocate John C. Calhoun (not even from Georgia!):
An unmasked 12-week-old… (leash illegally held by an unmasked adult human):
Presidents Biden and Harris have failed to reach all of the local merchants:
It turns out that “Liberty” may overlap with “Bull”:
Some tips…
a hotel with a great lobby (“living room” overlooking the river): Hyatt Regency (we stayed at the Hilton Garden Inn and would not recommend due to noisy A/C unit next to bed)
The Collins Quarter for breakfast
Related:
August 2020 mask requirements in other cities and counties in Georgia, e.g., “Atlanta – Includes Atlanta’s airport, city parks and other public places. People under 10 and those with medical conditions are not required to wear masks. Anyone not wearing a mask at the airport will be asked to leave. In other parts of the city, violators could receive a citation and in a strict enforcement, charges with the possibility of jail time or a $1,000 fine.”
Mrs Merkel sounded the alarm on Tuesday after announcing tough new restrictions including a lockdown over the Easter holiday.
“We basically have a new pandemic,” Mrs Merkel told reporters in Berlin in the early hours.
“Essentially we have a new virus, obviously of the same type but with completely different characteristics,” she added.
Unless the coronavirus gets the memo about evolution being only a theory, Coronapanic now, coronapanic tomorrow, coronapanic forever?
(Note that Angela Merkel has a Ph.D. in quantum chemistry, but the misogynists at the Evening Standard call her “Mrs.” and not “Dr.” as would befit a colleague of Dr. Jill Biden, M.D., Ed.D.)
A late-1990s photo from Munich. Note the cultural appropriation (“Chinesischer Turm”) and the sitting ducks for a respiratory virus.
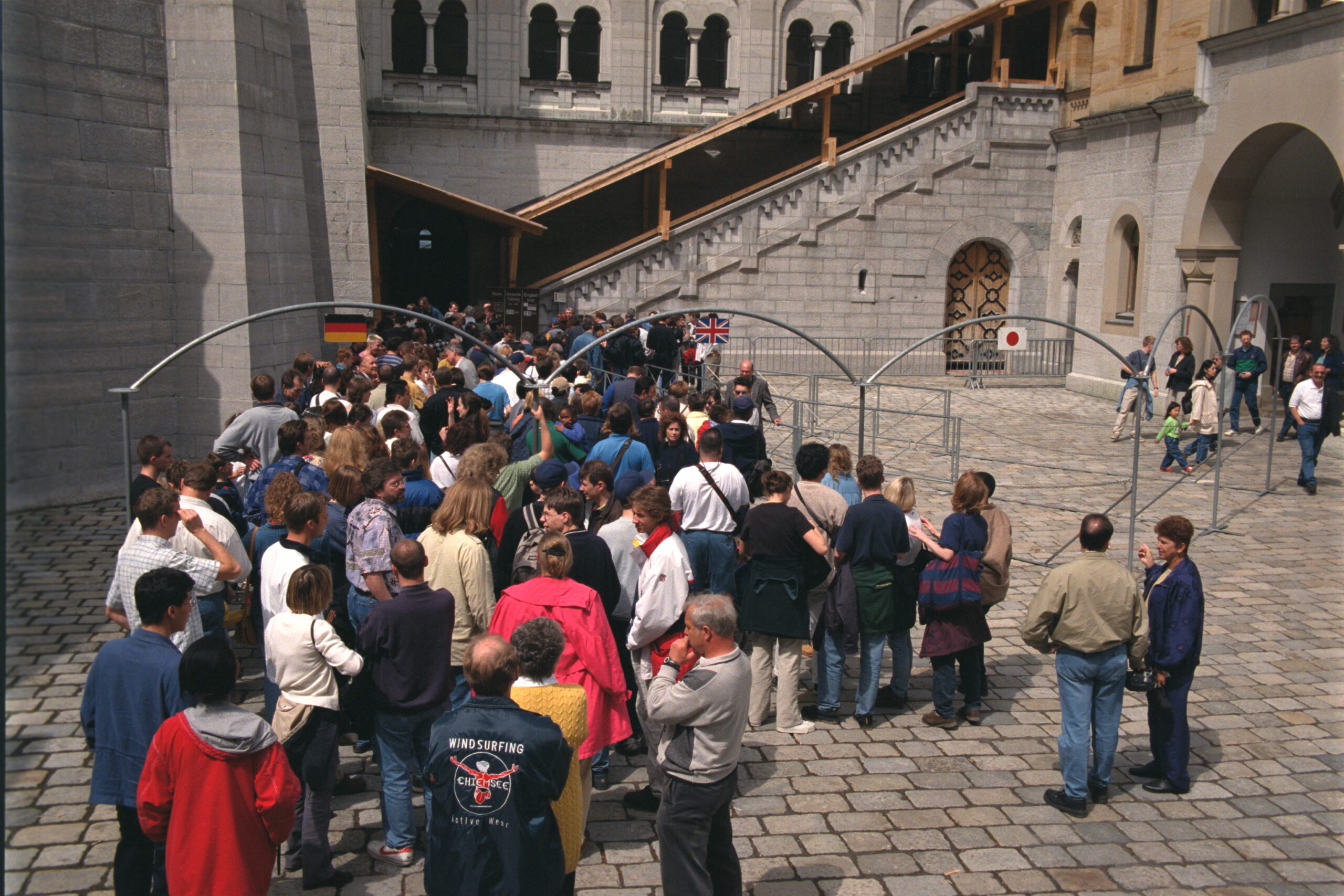
From the same trip (visit to Siemens, a major adopter of our ArsDigita Community System software), tourists try to cram themselves into Neuschwanstein.
Looking at these photos how humans used to behave, what is most shocking is that viruses didn’t drive us into our bunkers centuries ago.
… you will love The Lady and the Dale (HBO), a documentary regarding Elizabeth Carmichael, best-known for trying to bring Americans a lightweight three-wheeled automobile.
Ms. Carmichael was hugely successful from a biological/genetic point of view. From Wikipedia (10 kids total):
According to the FBI, Carmichael married four times while identifying as Jerry Dean Michael. She was charged with desertion for leaving her first wife, Marga, whom she met while stationed in Germany, and their two children. In 1954, she married a woman named Juanita, with whom she had two children before their relationship ended in 1956. In 1958, she married a woman named Betty Sweets after knowing her for four weeks. They conceived a daughter, but the marriage ended within a year. In 1959, she married Vivian Barrett Michael, her fourth wife, and together they had five children.
One aspect of the documentary is what happens to an opposite-sex marriage following a gender reassignment.
Americans are not as fascinated with engineering as with transgenderism and crime so the series does not explore what is most interesting to me: Why are cars so heavy?
Passenger rail turns out not to be fuel-efficient because railroad cars are so heavy, dwarfing the weight of even the most obese group of humans who might occupy a car.
The lightest cars on the market today weigh roughly 3,000 lbs. (Toyota Corolla, for example). Electric cars are heavier, e.g., a Tesla 3 is around 4,000 lbs. with a battery offering comparable range to a compact gasoline-driven car. The Chevy Bolt is around 3,600 lbs. Liz Carmichael’s Dale was 1,000 lbs.
It looks as though a prototype has been preserved in a Nebraska museum:
If we want to save our beloved planet, either by burning less gasoline or consuming less electricity, why don’t we slim down our vehicles to what is actually required to transport 500 lbs. of humans? Because we can’t make a car that rides comfortably at 70 mph unless it is heavy? First, with the U.S. population headed toward 500 million, it is unclear that anyone will be driving 70 mph. Second, could we improve the ride quality of lightweight vehicles with active suspensions?
Readers: Who has seen this show? What did you think?
Related: Can-Am Spyder, a modern 3-wheel vehicle made by a Bombardier subsidiary.
… a very small study using objective measures — weight measurements from Bluetooth-connected smart scales — suggests that adults under shelter-in-place orders gained more than half a pound every 10 days.
That translates to nearly two pounds a month, said Dr. Gregory M. Marcus, senior author of the research letter, published on Monday in the peer-reviewed JAMA Network Open. Americans who kept up their lockdown habits could easily have gained 20 pounds over the course of a year, he added.
Many of these people were losing weight before shelter-in-place orders were issued in their states, Dr. Marcus noted. “It’s reasonable to assume these individuals are more engaged with their health in general, and more disciplined and on top of things,” he said. “That suggests we could be underestimating — that this is the tip of the iceberg.”
3.5 percent identified as Black or African-American; about 3 percent identified as Asian-American.
What was the precise mechanism by which we went from fat to obese?
An earlier study by U.C.S.F. researchers looked at daily step counts, as tracked by smartphones, among nearly half a million people in nearly 200 countries. The number of steps people took declined by 27 percent a month after the World Health Organization declared the pandemic.
The concern about exercise also extends to children, who are known to pack on unhealthy pounds during the summer recess months when they are not in school. The risk is even greater for Hispanic and Black children than for white children, said Andrew G. Rundle, an associate professor of epidemiology at Columbia University’s Mailman School of Public Health, author of a recent paper that expressed concern that school closings would exacerbate existing racial health disparities.
My own recent efforts to diet with hushpuppies at Southern Soul Barbeque, a short walk from KSSI (St. Simons Island, Georgia, which also has an on-field hotel).
But why walk or waddle when you can drive? This car from Avis had ample horsepower (485, which is more than 2X the engine in a Cirrus SR20) for accelerating even the heaviest American into a low Earth orbit.
(There is no surer way to feel stupid than driving a Dodge Charger around a sleepy golf resort! It might have been smarter to take a crew car from the FBO.)
The coronavirus will never make it through our layers of blubber!
I wouldn’t recommended the experience for those who are anxious about COVID-19. While you’re constantly being reminded about how hazardous COVID-19 is, there isn’t enough room in the airport to be truly distant from those who are potentially infected. People sit glumly with their masks on, waiting to see how the Russian roulette game that they’ve chosen to play will turn out. Unless you believe in the effectiveness of crude non-N95 masks, it’s the same risk level as being in a crowded Miami club, but a lot less fun.
One of the great things about Internet, which even Facebook hasn’t managed to destroy, is that reader comments can be much more interesting than the original post. From RS:
Can we just say that about all other aspects of life? I would love if people who are anxious about COVID-19 would just stay home so the rest of us can get back to normal life. It feels like they’re holding society hostage so they can have the illusion of protecting themselves without having to do the one thing that actually protects them (staying home).
With a handful of exceptions (Florida, South Dakota, Sweden, Russia), it seems as though the coronanxious are in charge and able to force those who don’t mind coexistence with this virus and its myriad variants (the “covidiots”) into various forms of shutdown, mask theater, etc. The coronanxious have pretty much sat at home for a year anyway. It wouldn’t have cost them anything or increased their personal risk if they’d let the non-anxious carry on with their lives, education, and careers.
So that raises the question… why is it obvious that the coronanxious would prevail in setting government policy? (i.e., could we have predicted Mass Karenhood?) Is it because leaders tend to be old and therefore personally vulnerable? Is it because the restrictions imposed don’t hurt the elite and the elite are indifferent to the suffering imposed on the non-elite? (public school shutdowns aren’t a problem when your children and/or grandchildren are in private school…)
Note that more than 20 percent of Florida’s residents are over 65 (and therefore potentially vulnerable to COVID) while just 14 percent of Californians are over 65. So the COVID death rate among the elderly in Florida is almost surely much lower than in masked-and-shut California.
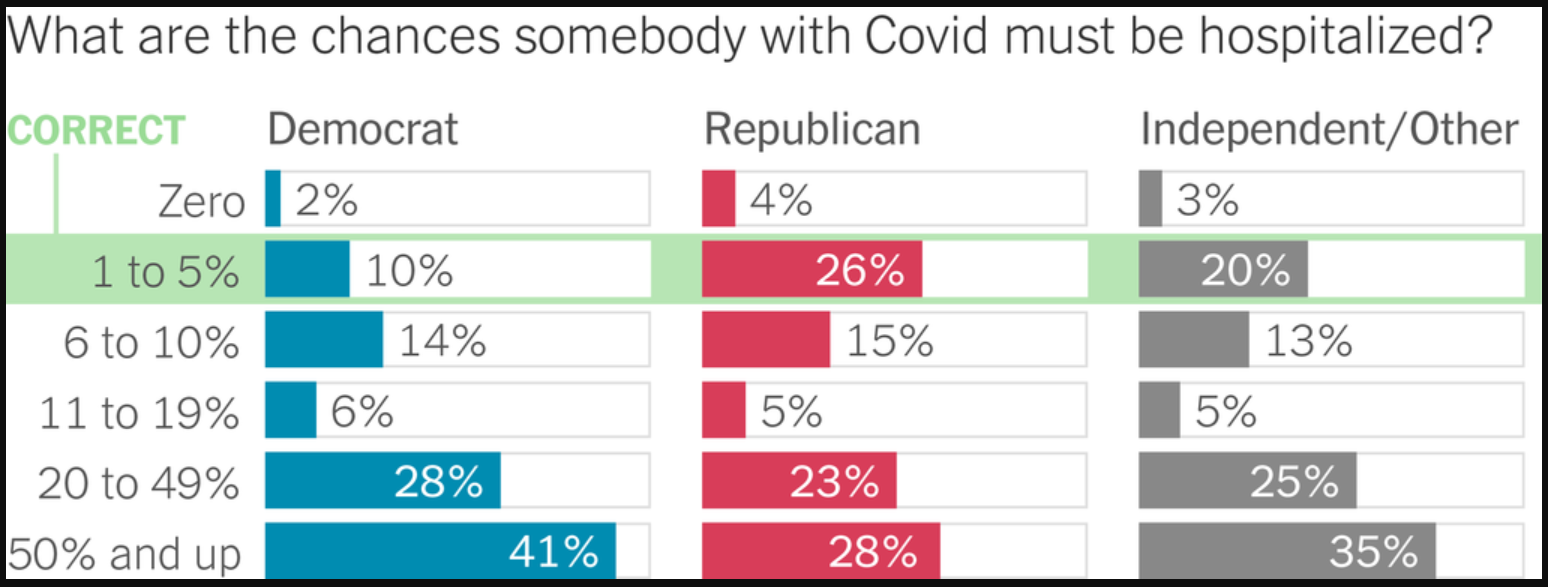
An objective measure of panic from one of America’s principal vendors of panic, the New York Times (March 18, 2021):
First of all, it is unclear whether the 1-5% hospitalized answer is actually “correct” if you consider “with Covid” to mean “could produce a positive PCR test”. With the CDC estimating that more than half of Americans have been infected with coronavirus, is it conceivable that COVID-19 means a 5 percent risk of hospitalization? We should have seen 2.5 percent of the folks we know carted off to the hospital (with a median personal network size of 472, the typical person should know 12 people who’ve been hospitalized with COVID). Leaving that aside. Casual inspection of this chart shows that 88 percent of Democrats overestimate the risk of hospitalization from COVID-19 while 70 percent of Republicans do. The journalists at the New York Times nonetheless report that “Republicans tend to underestimate Covid risks”. Based on the chart, it would be more accurate to say “Four percent of Republicans tend to underestimate Covid risks.”
I’m beginning to think that the Windows PC that I built in 2015 is ready for retirement (though if Joe Biden can be president at 78, maybe this PC can last until 2029?). In looking at new desktop PCs and motherboards I am struck by the paucity of USB-C ports (standardized in 2014). It looks as though 0 and 1 are the most common number of USB-C ports on a 2021 PC.
Wouldn’t it make more sense for all of the USB ports on a new PC to be USB-C and then use adapters for legacy components?
Not everyone was immediately captivated with technology’s advances. Just months after Cornelia [Vanderbilt] celebrated “reaching her majority,” author Willa Cather gave a speech in which she presciently waxed philosophical on the subject of the phonograph. “We now have music by machines, we travel by machines,” she said. “Soon we will be having machines to do our thinking.”
(Note that adulthood and voting in those days came at 21, not at 18!)
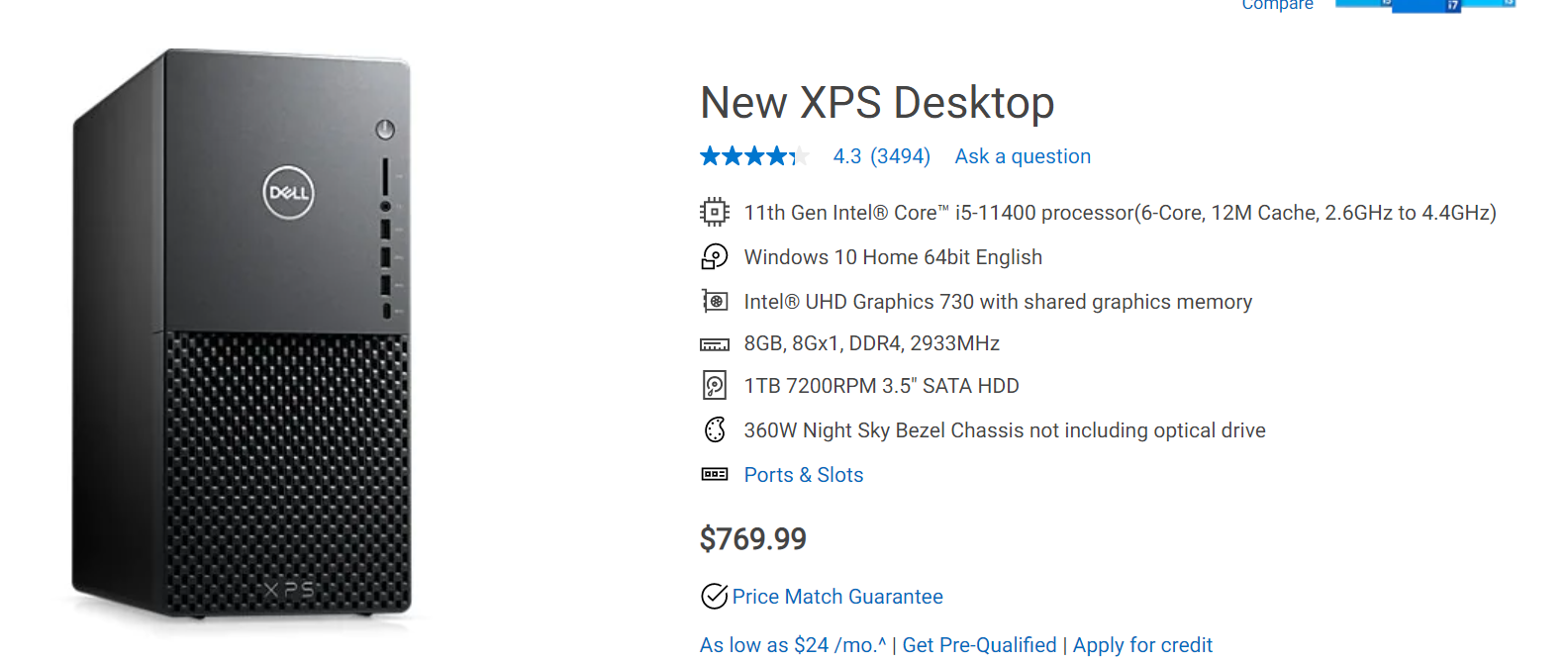
The great Willa Cather expected great progress from the world’s nerds. What do we have 100 years later? A Dell XPS desktop PC, “Engineered and designed with purpose for ultimate power and expandability”, equipped with a mechanical hard drive and a feeble 8 GB of RAM (is that even enough to run Windows by itself?).
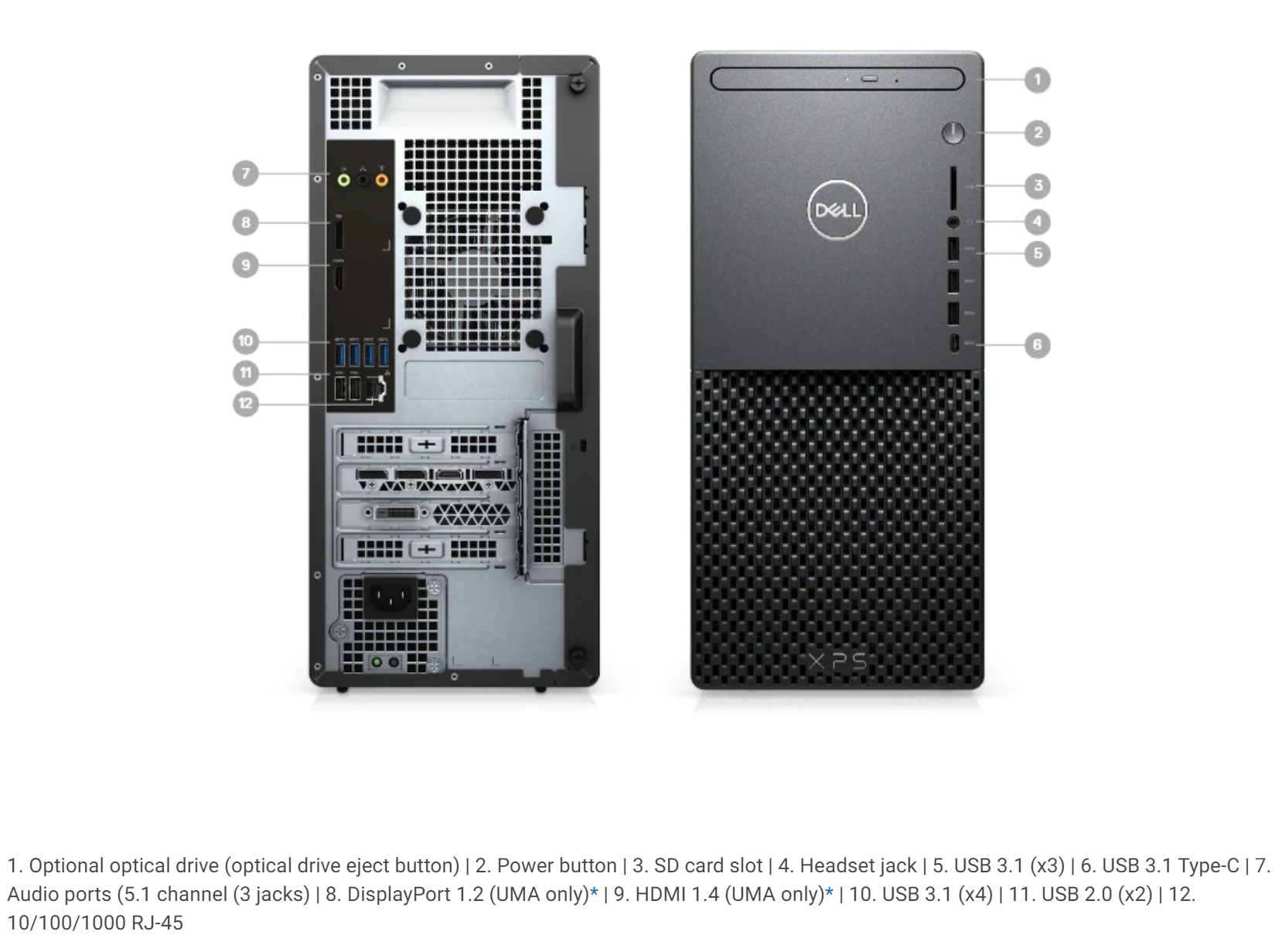
The machine has a single USB-C port and eleven legacy USB-A ports.
What if you want to spend $5,000 on an Alienware gaming desktop from Dell? You get… a 2 TB mechanical hard drive (also an SSD), a healthy 128 GB of RAM, and two USB-C ports (plus a bunch of USB-A ports).
Apple fanboys/fangirls/fanothers: even the Mac Pro includes two legacy USB-A ports (admittedly it also has four Thunderbolt ports). Why is this relic of old tech cluttering the clean design of an Apple product in 2021?
Related:
USB4 was standardized in 2019, but PC motherboards still don’t support it at all? (and therefore nobody should build a new PC right now because the USB4 motherboards are around the corner?)
Considering migrants who’ve arrived since 2014, of those who have said that they were under 18 years old at the time of border crossing (as these folks are undocumented, there is no way to know their actual age), 96 percent are still in the U.S. according to “Hundreds of minors are crossing the border each day without their parents. Who are they?” (Washington Post):
Central American and Mexican children, tweens and teenagers traveling without parents are crossing the border in soaring numbers, once more creating a logistical and humanitarian emergency for the U.S. government.
If the climbing trend line continues, the Biden administration will take in record numbers of unaccompanied minors this month, an influx made more challenging by the coronavirus pandemic.
To accommodate the growing numbers and meet social distancing guidelines, the administration opened a tent facility in Carrizo Springs, Tex., last month. The Biden administration is planning to open additional tent sites in the coming weeks and is looking at Moffett Field in California, Fort Lee in Virginia and other federal properties where it can set up temporary shelters.
Most unaccompanied minors cross the border into the Rio Grande Valley of South Texas. Some try to evade capture after crossing, but most seek out U.S. border agents to begin the process of making a humanitarian claim.
The odds of being deported are low. DHS statistics show that just 4.3 percent of the 290,000 minors who have crossed the border without a parent since 2014 have been returned to their countries. Of the rest, 52 percent had immigration cases pending. An additional 28 percent had been granted humanitarian protection by U.S. courts and 16 percent had been ordered to leave, but lacked a confirmed departure or deportation.
Most of these folks will end up on a lifetime of means-tested “not welfare” government programs, e.g., public housing, Medicaid, SNAP (“food stamps” or “EBT“), and Obamaphone. Why add to the working taxpayers’ burden by funding immigration courts, lawyers, border guards (the “welcoming committee” since the minors do not try to avoid being “captured”), and detention facilities (#TentsNotCages?) if the almost inevitable result is the “minor” staying?
Separately, should we be funding hot drinks from Chocolate Mayordomo for migrants passing through Oaxaca (photo from a 2005 trip)?
Also from 2005, modern-day migrants repopulate, at least during the daytime, a city that had been abandoned for more than 1,000 years (Monte Alban):