One-percenters irresponsibly gather in Sturgis starting today
“Despite delta, Sturgis Motorcycle Rally poised to ride again” (ABC):
South Dakota’s Sturgis Motorcycle Rally, which begins Friday and runs through Aug. 15, is expected to draw upwards of 700,000 attendees. Last year’s rally, which took place during the height of the United States’ summer surge, had more than 400,000 estimated attendees, many of whom didn’t wear masks as they patronized bars, restaurants and concerts.
The downstream effect was tangible: At least 649 COVID-19 cases were linked to Sturgis, including secondary and third-degree contacts.
Republican Gov. Kristi Noem supports the rally, a major economic driver in the state.
“There’s a risk associated with everything that we do in life,” Noem wrote on Twitter Wednesday. “Bikers get that better than anyone.”
So… the 400,000 Fauci-deniers in 2020 were responsible for 649 out of the 35,392,284 total cases thus far reported out of PCR toaster ovens in the U.S. Reprehensible! (see this Bill Burr video at 6:40 for the correct way to say “reprehensible”)
See also “Oxford study: 2020 Sturgis Rally tied to more than 400 COVID-19 cases across 30 states, 1 death”:
More than 463 COVID-19 cases across 30 states were directly connected to the Sturgis Rally in August and September 2020. Seventeen patients were hospitalized and one person died, according the report by the Oxford University Press for the Infectious Diseases Society of America.
The #Science-informed righteous condemned the Sturgis gathering in 2020 and they are condemning it this year as well.
Let’s look at a smaller mass gathering that is not condemned and for which there have been no calls for shutdown. Provincetown, Massachusetts has a population of about 3,000, which expands with tens of thousands of additional visitors during summer weekend (certainly not to 400,000; the town has essentially just two streets). From Slate:
According to a report the agency released on Friday, the CDC’s latest findings were based on a July 4 COVID-19 outbreak in queer mecca Provincetown, Massachusetts, where among a cluster of 469 (with no deaths) at the time of study, an astonishing three-quarters of the infected had been fully vaccinated. As of July 31, the P-Town outbreak had ballooned to 965 cases.
It was about halfway through our weeklong stay when one vaccinated friend from New York City began to report not feeling well. Unable to stop coughing, he and his boyfriend drove to Outer Cape Health Services, where he tested positive for COVID and immediately fled the cape. Soon after that, I began to hear whisperings—whether at the Mussel Beach gym or traditional “high tea” gatherings by the pool at the Boatslip Resort—of a “gay cough” circulating among some out-of-towners.
The gathering in Provincetown caused 2X as many cases as Sturgis 2020, despite being only about 1/10th the size (could there be a behavioral difference comparing Harley riders to P-town visitors?). Shouldn’t we expect public health experts to demand a governor’s order to shut down the P-town scene? Why is it irresponsible for motorcycle enthusiasts to gather in South Dakota and responsible for New Yorkers and Bostonians to gather in Provincetown?
Addressing the national lifeguard shortage (July 2018):

View of the harbor from the public library:

A P-town shop in which all genders are welcome, but only one gender ID has a future (July 2018):


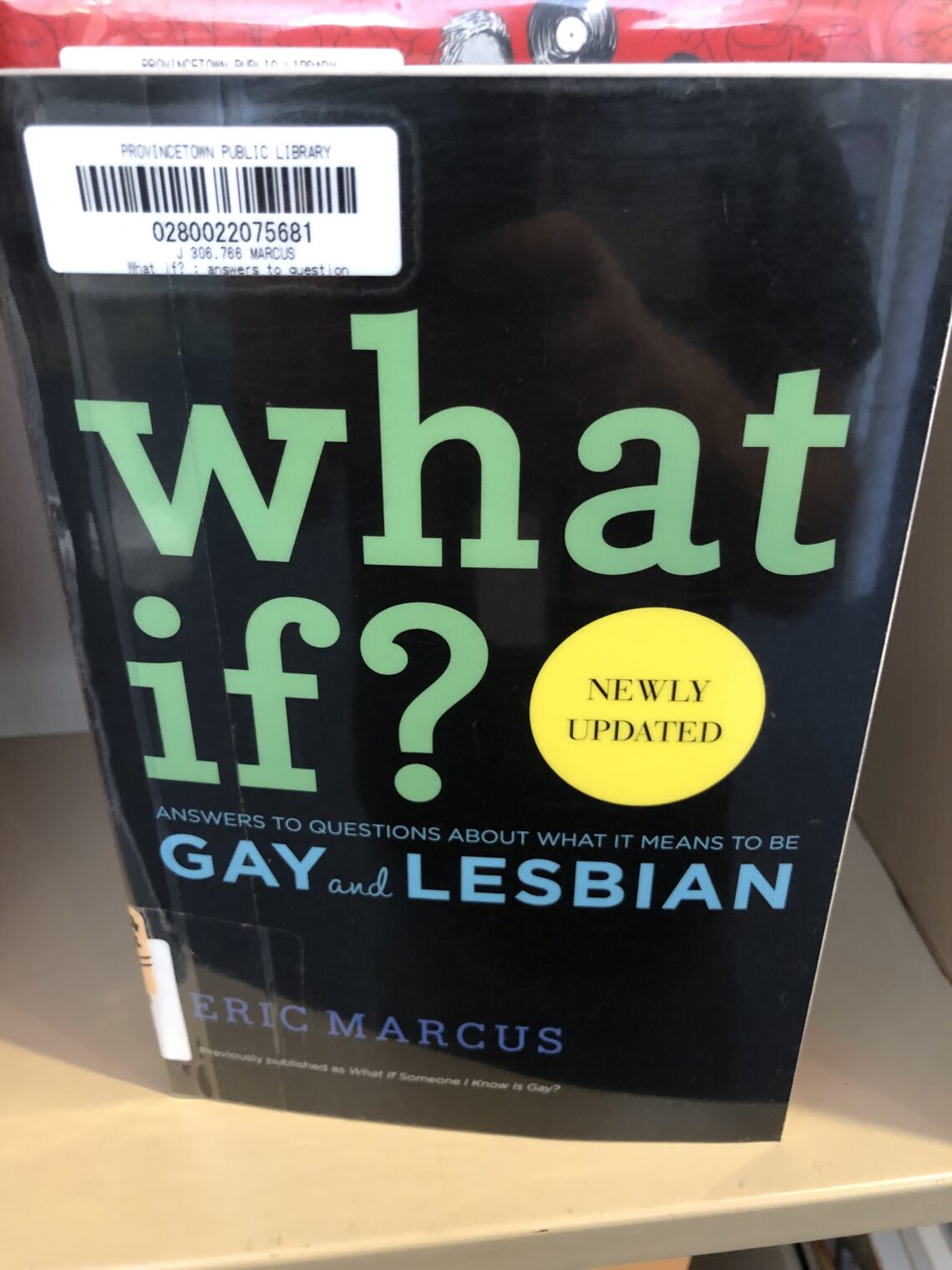
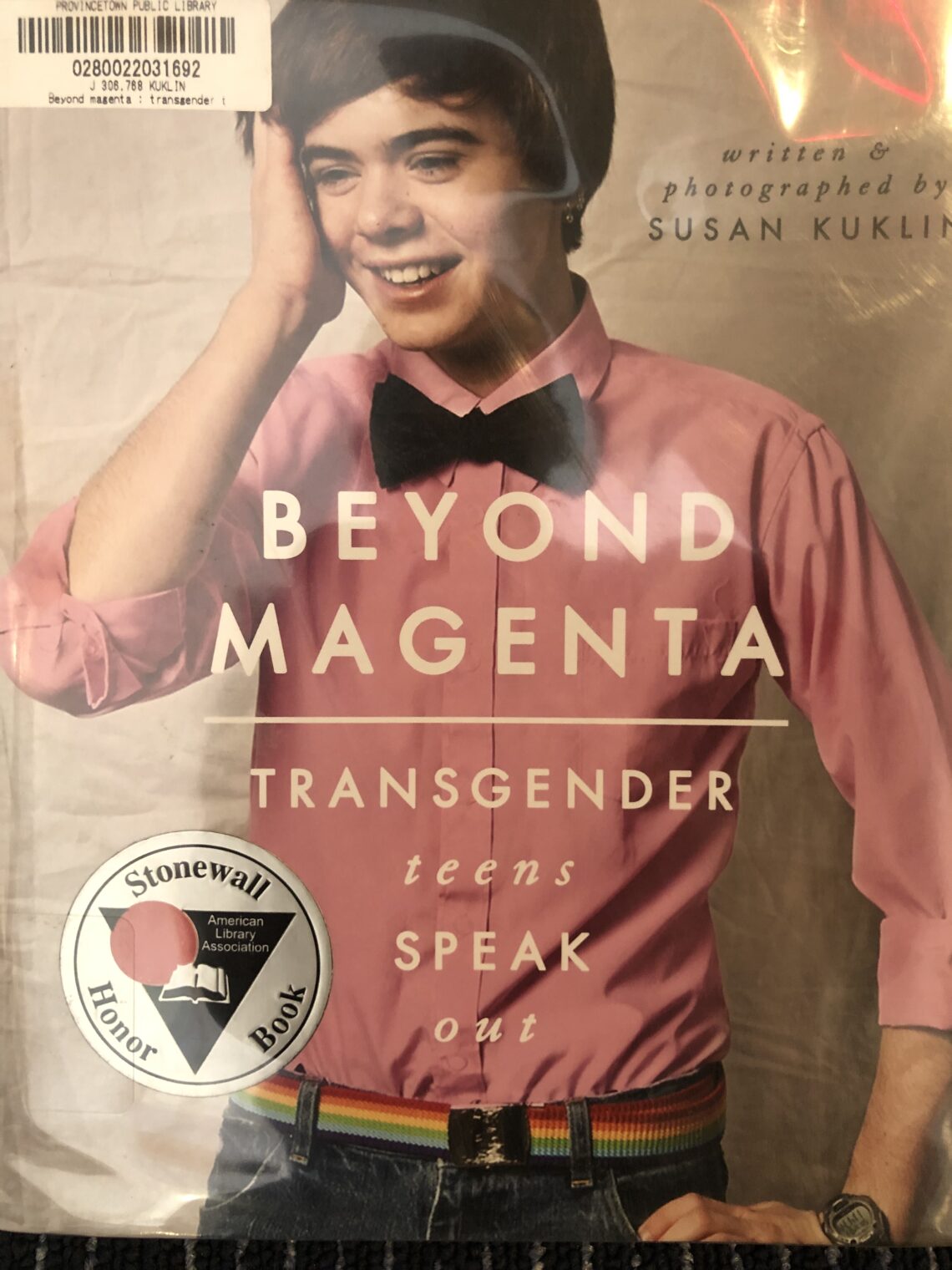
The featured Young Adult Non-Fiction section at the public library (March 2019):
What if we try to merge the rainbow of Provincetown with the value system of Sturgis? We get “Better a Sister in a Whorehouse than a Brother on a Honda” T-shirts in a rainbow of colors!